
Guest essay by Indur M. Goklany
Don’t look just at deaths from coronavirus, look at cumulative deaths from comorbidities. Since most people dying from coronavirus also exhibit comorbidities,[1] and it is unclear how deaths are assigned to the former rather than one of the co-morbidities and whether there is a uniform accepted methodology from one doctor to another (or one hospital to another or one country to another) in the assignments, it is not clear how much credence can be given to coronavirus death estimates at this time.
This also means that we shouldn’t attempt cross-country and cross-jurisdictional comparisons because they could mislead. It is best to look at (and compare) aggregate excess deaths from all co-morbidities rather than just one or another co-morbidity. I would suggest looking at excess deaths against an average over the last 5-10 years for both all-cause deaths and deaths from all coronavirus-plus- comorbidities to get an idea about how devastating coronavirus has been versus an average year.
To compare deaths between jurisdictions, don’t look at absolute deaths, look at death rates, based on population sizes. It makes no sense to compare absolute numbers of deaths in Italy, UK, San Marino, and Sweden against those in the U.S.
Each area is different. From where I sit — in Northern Virginia — New York is another country. And from upstate New York, New York City is also another country. Risk factors such as population density, use of mass transit, presence of people who have recently travelled elsewhere, norms regarding appropriate social distance, household size, age composition of households, and all the other coronavirus risk factors are likely to be different in each area. One should, therefore, expect each location would have its own curve that would have to be flattened. Some areas may literally be “ahead of the curve” since these areas have had some advance warning before the virus was brought into their communities and may not need to take drastic measures to flatten the curve. Aggregating data across urban and rural areas does not make much sense.
I wouldn’t be surprised if at the end of the current period with most populated areas currently shut in by individual choice or government decree, once all the data are in, excess deaths for all causes are not negative relative to the 5- or 10-year average, since physical distancing should also reduce transmission of the flu (influenza and pneumonia kill about 50,000+ Americans annually)[2]. At least, I would hope that would be the case, so we can look back and see that some good came of our flattening our economy. At least one can hope.
[1]https://www.hopkinsguides.com/hopkins/view/Johns_Hopkins_ABX_Guide/540747/all/Coronavirus_COVID_19__SARS_CoV_2_
[2] https://www.cdc.gov/nchs/data/nvsr/nvsr68/nvsr68_09-508.pdf
This is an excellent idea. It does seem to be a ‘political’ decision to attribute COVID 19 as the cause of death where it is simply present at death. In the UK, I understand that COVID 19 is a notifiable disease which means that it is recorded as the cause even though it may merely be present. Contrast this with influenza or other respiratory infections which are not notifiable – in cases of co-morbidity, I understand the cause may be assigned to one of the co-morbidity diseases present, not necessarily the infection. The situation is similar in Italy where it was recently estimated that only 12% of deaths ascribed to COVID 19 were actually caused by it.
I hope the data needed to perform Mr Goklany’s analysis is available!
where it is simply present at death….exactly
and the CDC even says when it’s suspected…and not confirmed
CDC established coding credits COVID-19 as cause of death….if it’s suspected at all….
In other words…if you die of a heart attack….and they suspect (not tested)…that you have CV….you are listed as CV
here > https://www.cdc.gov/nchs/data/nvss/coronavirus/Alert-2-New-ICD-code-introduced-for-COVID-19-deaths.pdf
Your own link says no such thing you are suggesting … read it again slowly and carefully.
If the death certificate reads heart attack .. you are listed of dying of a heart attack.
The only reason you would get a covid19 id would be in the case COVID contributed to the death and via the definitions above it has to be a significant part.
“COVID-19 should be reported on the death certificate for all decedents where the disease caused or is assumed to have caused or contributed to death”
ROFL it’s a death certificate that isn’t as flippant as you seem to be suggesting. At the top it tells you the normal process if it’s only suspected you declare it as such and the body goes for autopsy to make determination. What I see is people who don’t understand the process making silly assumptions.
I should add the email is clearly for Doctors who are dealing with covid19 deaths and need a code to put on the death certificate. It has nothing to do with sites collecting data on covid19 like John Hopkins etc.
it only shows up in the death counts if it is the initiating underlying cause. And in regard to another comment, almost none of the COVID deaths are being autopsied and there is no reason why they would be.
Do you have evidence that autopsies are done, or merely assuming? Germany is advising against doing autopsies on deceased COVID patients.
Remember, you don’t get a point for more funding if the guy died of a bullet between the eyes. So maybe the guy who loaded the gun had COVID-19 (wink!) Voila! COVID-19 “associated” death!
the CDC has very specific instructions. It has to be the initiating underlying cause, which is specifically defined. I submitted a post on this, because I do think there are serious issues regarding underlying chronic conditions and who fills out these forms typically. You can also see the post at https://healthy-skeptic.com/2020/04/04/what-is-the-cdc-up-to-with-causes-of-death/
Kevin Roche,
I read your post at HealthySkeptic.com. Thanks for sharing it. It was excellent. It was well written, informative, and sensible. The absence of this sensible perspective feeds the current panic.
In the US, we don’t measure deaths from flu. The CDC estimates them based upon model runs. That’s why they typically offer a 2:1 range when stating total infections, total hospitalizations, or total deaths. Here, we are offered the illusion that the world is accurately measuring the progression of COVID-19 from SARS-COV-2, when in fact, we have no idea what we are measuring.
COVID-19 is now a mandatory reported disease. They will be tracking it from now on – confirmed or not.
“…look at what has happened since the emergence of Covid-19. The list of notifiable diseases has been updated. This list — as well as containing smallpox (which has been extinct for many years) and conditions such as anthrax, brucellosis, plague and rabies (which most UK doctors will never see in their entire careers) — has now been amended to include Covid-19. BUT NOT FLU.
That means every positive test for Covid-19 must be notified, in a way that it just would not be for flu or most other infections.
In the current climate, anyone with a positive test for Covid-19 will certainly be known to clinical staff looking after them: if any of these patients dies, staff will have to record the Covid-19 designation on the death certificate — contrary to usual practice for most infections of this kind.
There is a big difference between Covid-19 causing death, and Covid-19 being found in someone who died of other causes. Making Covid-19 notifiable might give the appearance of it causing increasing numbers of deaths, whether this is true or not. It might appear far more of a killer than flu, simply because of the way deaths are recorded.
If we take drastic measures to reduce the incidence of Covid-19, it follows that the deaths will also go down. We risk being convinced that we have averted something that was never really going to be as severe as we feared. This unusual way of reporting Covid-19 deaths explains the clear finding that most of its victims have underlying conditions — and would normally be susceptible to other seasonal viruses, which are virtually never recorded as a specific cause of death.
…..if we tracked flu or other seasonal viruses in the same way, we would also see an exponential increase. We would also see some countries behind others, and striking fatality rates.”
https://principia-scientific.org/an-explanation-of-why-the-covid19-numbers-appear-high/
LdB: COVID contributed
CDC: COVID-19 … assumed …
Perhaps, you read a bit too quickly, LdB. Perhaps, you are deliberately attempting to obfuscate. Whichever, you are mistaken.
Sorry you guys have no idea of the process … it is a DEATH CERTIFICATE not some random piece of paper. The doctor could rightly “assume” if he has been treating a patient on a ventilator and patient dies unless he suspects foul play he can assume it was covid19.
You are ignoring who that the e-mail is for a doctor treating covid19 patients giving them a code and they have a clear framework in signing a death certificate.
Anyhow I am done arguing this you people are crazy and just making stuff up based on ignorance.
Janice Moore –good catch! That was ‘Latitude’s point in his comment along this line above. From the CDC link he provided:
“Should “COVID-19” be reported on the death certificate only with a confirmed test?COVID-19 should be reported on the death certificate for all decedents where the disease caused or is assumed to have caused or contributed to death. Certifiers should include as much detail as possible based on their knowledge of the case, medical records, laboratory testing, etc. If the decedent had other chronic conditions such as COPD or asthma that may have also contributed, these conditions can be reported in Part II. (See attached Guidance for Certifying COVID-19 Deaths .. ‘ ”
“assumed to have caused or contributed to death” — pretty loose judgement call for getting the COVID-19 death count code! Even if someone had, say, pneumonia and COVID at the same time, the death could easily be counted as COVID?
There is an amusing part to the idea Doctors just put death by Covid19 on anyone who tests positive … you could shot and kill anyone with Covid19 and the death certificate reads death attributed to covid19. Your defense in court then becomes you didn’t kill the person as recorded on the death certificate covid19 got him.
Replying to Janice M. — Oh, yes, and adding to my other reply just now, there is the paragraph up near the top of that CDC page, probably relevant to how the numbers would be reported:
“Will COVID-19 be the underlying cause? The underlying cause depends upon what and where conditions are reported on the death certificate. However, the rules for coding and selection of the underlying cause of death are expected to result in COVID-19 being the underlying cause more often than not. ”
So, again, a pretty loose judgement call would appear to count a ‘multiple causes’ death as ‘COVID underlying’ , “more often than not”.
David your argument requires the patient to have already had pneumonia but not being treated by a doctor (so it isn’t bad or they are heroic) then subsequently getting covid19 so they are now positive. Now they are admitted for covid19 and subsequently die and are recorded. Yep under that exact situation the doctor could make a wrong judgement call 🙂
Same situation from car deaths if a person runs off road and dies but has a heart/stroke history but not bad enough to be able to conclusively test. Do you record the death as a car crash or a heart problem … the doctor has to make a judgement call.
Thank you for the affirmation, David B.. :). Yes, I was merely backing up Latitude dude and Grumpy.
And, nice analysis by you. You even got old LdB to fire off an analogy by which he shot himself in the foot. Heh.
and note on the CDC active COVID19 reporting site the dramatic drop off in the monthly trend of Pneumonia Deaths as the Corona Deaths begin to appreciably increase.
When monthly Pneumonia Deaths are running 2900, 2800, 2800, 2900 and then drop to 2000 as Corona deaths double up to 788, 1000 we can draw a reasonable conclusion that if Corona had never existed that those deaths would have occurred and been recorded as pneumonia.
That was my assumption as well. US winter deaths from pneumonia range from a base of around 30,000 a week up to 50,000 around mid-January. Last season was a low season and it looked like 2019-20 was following a similar pattern until January when the figures dropped to below any figure AT ALL for the last six years.
That can only (realistically) be because a large number of what “ought to be” pneumonia deaths are recorded as something else.
There are some anomalies in some of the UK figures. See here:
https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/weeklyprovisionalfiguresondeathsregisteredinenglandandwales.
There’s a downloadable xls file with an update due tomorrow (Tuesday).
anyone doubt that if you get admitted to a NYC hospital and are not infected that you will be within days …
Has anyone heard of any data in relation to Beijing and Shanghai? About say, 1000Kms from Wuhan supposed epicentre, with the major international cities shut down, I’ve heard absolutely nothing about the Chinese capital and major industrial centres. You would have to think they were devastated, but again have heard nothing, does anyone have any information?
That was why they jumped in with total quarantine of Wuhan and soon after the whole of Hubei. They would have been is serious shit if it had taken over their biggest cities.
I have seem a map of COVID accross RPC but it was just red blobs of varying intensity. There seemed little that was not at least a bit pink. The containment was reasonably successful. Sorry I don’t have a link.
https://blog.nomorefakenews.com/2020/04/05/covid-here-come-the-antibody-tests-quick-easy-and-insane/?
COVID: here come the antibody tests—quick, easy, and insane
4/5/20 Jon Rappoport
Welcome to the real world, where: “the discovery of a new virus (COVID) is unproven; the notoriously useless PCR diagnostic test for the virus renders case numbers meaningless; and the proposition that COVID is a real disease with one cause is a con job.”
Look here if you want to know more about Jon Rappoport: https://americanloons.blogspot.com/2014/05/1050-jon-rappoport.html
CONCLUSION: TOTAL WINTER DEATHS DO NOT MATTER, BUT COVID-19 DEATHS ARE MUCH MORE IMPORTANT.
Update of my previous post:
Data for Europe is now up to end of week 13 – to ~31Mar2020.
Note the downturn in deaths for under-65’s. and the upturn for over-65’s.
Not only has this year’s total winter mortality declined substantially for all ages, it has even declined substantially for those over 65 when compared to previous years. Repeating, TOTAL WINTER DEATHS ARE FAR LOWER THAN IN RECENT YEARS. We will learn from this full-scale experiment.
It seems ironic that when we wrote about HUNDREDS OF THOUSANDS OF EXCESS WINTER DEATHS due in part to high energy costs caused by false green climate hysteria, nobody listened, but now we are now prepared to shut down our economies due to A FEW THOUSAND DEATHS allegedly due to Covid-19, WHEN TOTAL WINTER DEATHS ARE ‘WAY DOWN.
CONCLUSION: TOTAL WINTER DEATHS DO NOT MATTER, BUT COVID-19 DEATHS ARE MUCH MORE IMPORTANT.
This data now extends to the end of Week 13, which corresponds to March 31, the end-date for the calculation of Winter Mortality and Excess Winter Mortality. We should also recognize that the Covid-19 flu is not over yet, and mortality figures are continuing to increase.
https://www.euromomo.eu/index.html
More data here:
https://www.worldometers.info/coronavirus/#countries
Regards, Allan
_________________________________________
https://wattsupwiththat.com/2020/03/30/covid-19-deaths-in-europe-excess-mortality-is-down/#comment-2951760
http://www.drroyspencer.com/2020/03/covid-19-deaths-in-europe-excess-mortality-is-down/
Roy Spencer wrote:
[excerpt]
“Given the global hysteria over the spread COVID-19, you might be excused if you are very surprised to learn that the most recent week of mortality data in the EU shows an actual decline from what is expected for this time of year.”
Mortality monitoring in Europe
https://www.euromomo.eu/index.html
Not only has this year’s winter mortality declined substantially for all ages as Roy Spencer stated, it has even declined substantially for those over 65! This data only extends to the end of Week 12, whereas the end of week 13 corresponds to March 31, the end-date for the calculation of Winter Mortality and Excess Winter Mortality. We should also recognize that the Covid-19 flu is not over yet, and mortality figures are continuing to increase.
https://www.worldometers.info/coronavirus/#countries
Roy’s above analysis is consistent with my proposed methodology published on 29Mar2020 at:
https://wattsupwiththat.com/2020/03/28/us-states-ditching-misguided-reusable-plastic-bag-incentives-to-reduce-covid-19-contamination-risk/#comment-2949993
[excerpt]
“One objective measure would simply be to count total deaths from all causes and compare that the past years, country-by-country – if the total death rate in Winter 2019-2020 (1Dec2019 to 31Mar2020) is no greater that other years, then we can start to understand the big picture. Right now, we are tilting at windmills – some people think this flu is the “end-of-the-world”, and others say it is “nothing special” compared to other seasonal flus.
I only had access to limited data but came to this conclusion, also on 29Mar2020:
https://wattsupwiththat.com/2020/03/28/us-states-ditching-misguided-reusable-plastic-bag-incentives-to-reduce-covid-19-contamination-risk/#comment-2950298
Trying to see the Big Picture of Covid-19 – difficult with a moving target and poor/limited data:
…
Covid-19 Winter Deaths to date = ~2.6% of USA average Excess Winter Deaths
…
Covid-19 Winter Deaths to date = ~0.3% of Total USA Winter Deaths
…
Whether one considers Covid-19 deaths as ~2% of average Excess Winter Deaths or ~0.3% of Total Winter Deaths, Covid-19 is not that significant as a cause of death to date.
If Covid-19 extinguishes in the Spring like most seasonal flu’s, it will have had a minor or negligible impact on Total Winter Deaths – negligible if these people were already mortally ill and would have died this winter anyway from other causes.
If Covid-19 deaths continue to accelerate after 31Mar, then it could qualify as a serious pandemic.
Fasten your seatbelts. Faites vos jeux.
Regards, Allan
the hysteria by the media may prolong this , but HCQ works… all worried should at least take as preventive.. Believe I was infected.( no test) with Coq the symptoms diminished, cough and related. Have used COq for some time and with no ill effects. as a uber driver, the infection was by contact in Nov. Symptoms @ur momisugly thanksgiving ,persisting until now.. whenever the cough returns I use HCQ and it abates… by the way I am a arthritis victim. hope this will change the perspcective of use.
Trump MUST FIRE Fauci immediately.
Figures for the UK and Europe shows deaths are down this year due to mild weather, a lower than average flu season and ironically the lock down has prevented many who would have caught flu but didn’t and lower deaths from car accidents. The covid 19 pandemic is as of the beginning of April is difficult to see
http://inproportion2.talkigy.com/
Tonyb
Tonyb
Thank you for that link. I’ve been telling my family that I didn’t think that CV19/coronavirus would have a huge impact on total deaths in the UK compared to a “bad” Flu winter like 2017/18. When 2020 is taken as a whole year will there be anything exceptional in total deaths?
See my link above. ONS figures are currently (up to March 20) showing nothing out of the ordinary in UK death numbers.
Right now the US is testing more people then anyone else, it has less cases per million then most other hot countries and has less deaths per million then most other countries.
Right now….
You’re always going to find something wrong, even if it’s right. Loser.
It’s a reasonable point. China is done ( and no one believes their figures anyway ). EU is past peak COVID infection, so I guess you could crudely double current figures to get final. US is still ramping the exponential, so saying “right now the US … has less cases/million” is senseless.
Compare Germany+Italy+Spain+UK+France to the US, roughly the same population and theoretically medical abilities. The US is doing better, not sure why everyone keeps saying the EU is closer to peak then the US, the US first infections where right around the same time as EU and as far as I see only Italy may have peaked in the EU, and their numbers I think are grossly under reported do to lack of testing, UK as well. With in the next week at the rate of testing going on in the US we will pass all of these countries combined in testing as well.
The US is doing as well as any country if not better in its response to this crisis and its a bigger country with many more issues to handle. At this point its also probably only one of 2 or 3 countries that is giving reasonably accurate information.
My point was that Simon is clearly anti-Trump, and anti-US. Just about every one of his posts shows it.
Most person that die in the US WITH Chinese coronavirus are being counted in the CCV death numbers including people in terminal care Hospice for other issues on “do not resuscitate” orders. These deaths are being referred to as death from “complications from Covid-19”.
There are some countries that would not count these people as CCV victims.
The number of US tests per day may be higher but on a per-capita basis, ~38 countries have tested more than the US (sort the last column of https://www.worldometers.info/coronavirus/#countries).
USA has a death rate of 29deaths/milllion from CV19.
Taiwan CV19 death rate is 0.2deaths/million.
The US figure is continuing to climb rapidly, still doubling every 3 days, so very poor result compared with Taiwan. Taiwan demonstrates what can be achieved with an effective pandemic response. Key element in their result is being skeptical of any official information out of China; a lesson for the rest of the world. AND know that WHO is controlled by China.
Until 100% of population tested, and periodically, we wont know who can get back out to mingle and work. Herd immunity wont be known until well after the herd is culled of the frail and old.
Meantime, perhaps NY’s hospitalizations per population could be useful as a predictor measure going forward for all the states just starting to accelerate, NJ MA MI FL TX etc.
Agree that counting deaths gives little actionable information, when 95% have comorbidity and 75% of those are 70+ it shouldn’t be a surprise that other deaths by “×” will have gone down. The regular deathrate at 70+ is already high compared to 30 year olds. Doubt that death by covid will reflect a change in overall death rate.
Like it should be no surprise NYC ER visits for under 25’s has dropped dramatically. No sports, no bars, less driving, no injuries, and a little more pragmatism before rushing in.
NYC area is probably a special case, like Northern Italy, as it had the greatest number of direct flights from Wuhan, was the number one tourist destination for Chinese nationals, has a large and vibrant Chinese community, high population density, large public transportation system, pollution, climate, etc.
Scissor,
Also, pre-CV-19 there were ~3000 flights per night across the N Atlantic (per 757/767 pilot friend of mine who routinely flew the routes to UK, France, Portugal, Spain, etc. out of Newark)
Zack,
Why would you need to test 100% of the population periodically to give the ok for immune people to return work? Once we have antibody testing up and running, people seeking permission to return to work could go through a drive-through testing center and self-administer a nasal/throat swab for active covid-19 infection and a finger-stick blood test for antibodies. Based on the covid test being negative and the antibody test being positive, they could be given an uninfected/immunity certificate that employers could rely on to allow the person to safely return to a job dealing with the general public. (Still maintaining social distancing, face masks, frequent hand-washing, and other reasonable precautions until a vaccine has been distributed).
This is the approach that we should all be demanding. Otherwise the cure will be far worse than the disease.
Scissor-
First US case was in WA state. Sacremento shortly after.
Once community aquired in NYC, flight frequency from China becomes kind of irrelevant to case load. Though I agree regularly riding elevators must have an effect on transmission speed. But depth?
Hospitalization per population gives you a good guess as to the curve’s outcome, if not it’s shape. Of course, stretch hospitalizations for Memphis or Toledo out over time relative to NY, but why presume a different volume?
Rich Davis-
You wouldn’t.
Cases of pneumonias have plummeted this year while cases of COVID-19 have gone up. It’s easy to create a panic-demic when you rob one mortality group to inflate another.
US pneumonia deaths – weekly
https://pbs.twimg.com/media/EUyBMdvWAAEZAwX?format=jpg
And it’s even easier when you tell doctors to issue death certificates with COVID-19 as the cause of death if they know it was the cause, or if they assume it was the cause or contributed to death without a test.
\CDC’ Guidance for Reporting COVID-19 on Death Certificate
https://pbs.twimg.com/media/EUvXWJ5WsAA7ti5?format=jpg&name=large
They used to call pneumonia the “old man’s friend” because it ended their life swiftly. There was a similar euphemism for flu.
Thanks icisil, that graph is very telling, rob one mortality group to inflate another seems to be a good summary.
Great chart on pneumonia. This entire post offers lots to think about.
Been saying this since I heard this joke as a CHILD:
It isn’t the fall that kills you, it is the sudden stop at the end.
We’ve known for decades that the flu doesn’t kill you it is the pneumonia or the infection you got at the hospital. The SUV didn’t kill the pedestrian the driver did. And when they revise all the numbers, that will not make headlines. Heck, they are still revising the numbers for the 2008 supposed recession! What’s the latest Leftist Democrat tactic? Ret Con? Or something like that. Rational people call it rewriting history and reject it.
Wrong. Go look up cytokine storm. Gotta go work on a serological test for COVID-19. Not a joke.
Huh?
How is the current Abbott 15-min test not adequate? The whole idea that I have been repeating here since somebody else suggested it (apologies that I can’t give credit where due), is to test apparently-healthy, asymptomatic people to qualify them to return to work.
Not disputing you that sick people suffer from cytokine storm.
Huh 2? A LOT has been revealed about how they are inflating the number of deaths attributed to this virus since you replied. In fact, one doctor pointed out that if someone came in from being hot by a bus and tested for the Chinese virus and the died if the injuries that current guidance said cause of death should be listed as Wuhan Flu.
https://swprs.org/a-swiss-doctor-on-covid-19/
Good for Sweden!
Re: “international pressure … to [skew the data to support alarmism]”
Fear = control.
(See “The Prince” by Machiavelli)
I am not a fan of F.D.R. in general, but in his 1st inaugural speech, he got it right:
… This is preeminently the time to speak the truth, the whole truth, frankly and boldly. Nor need we shrink from honestly facing conditions in our country today. This great Nation will endure as it has endured, will revive and will prosper.
So, first of all, let me assert my firm belief that the only thing we have to fear is fear itself—nameless, unreasoning, unjustified terror which paralyzes needed efforts to convert retreat into advance. …
**********
Sadly, as you (i cisil) accurately observed on the recent CM of B post, mind-numbing fear is causing even some of the best of us to reason illogically (e.g., using the logical fallacy of a false dilemma, i.e., either we passively do nothing at all OR we dictate an economy-crippling, liberty-smashing, “lock down,” failing to mention that there are rational, far less damaging, alternatives).
WR: By ‘skewing the data’ one can only win some days or a week. Than the curve retakes its exponential behavior and fear returns. Look at the death curve for Sweden: https://www.worldometers.info/coronavirus/country/sweden/
By ‘doing our experiments’ however we learn that ‘social distancing’ (1.5 meter), ‘using masks’ and ‘transparancy’ all are key solutions. Who does not like exponential death curves and who does not like fear introduces those three, retakes control over the epidemic and restarts the economy in a smart way.
Taking away the fear is done by ‘control’. Not by hiding facts: fear will soon be back.
My favorite countries for a holiday in present circumstances: South Korea, China or Taiwan. Not my own country (the Netherlands), Sweden or US. And in regard to the future I think the Netherlands is doing a good job by bending the curves already. Social distancing works. Of course we will like to restart our economy fully as soon as possible. The South Korean solution of ‘transparancy in information’ and/or the introduction of ‘smart apps’ could help a lot. See for a proposal for the last one the Abstract of: https://science.sciencemag.org/content/early/2020/03/30/science.abb6936
I was with you until you in passing gave credibility to whatever China has been/is doing and has been telling the world it has been/ is doing.
40 years ago, I was among the first to take a hard look at the fallout of Mao’s delusional Great Leap Forward which the Chinese told the world was a resounding success. We concluded that between 30-50 million people died and were treated like pariahs in the Sinophile academic world- today it is generally accepted that 45 million perished during those three years.
The Communist Party tried the same trick with the massive 1976 earthquake which they told the world was a flea fart – it turned 1MM plus people died.
Today’s WSJ has an excellent account of how the Chinese used the WHO to lie about and manipulate the Coronavirus storyline – an analysis from UofSouthampton apparently shows that if they had come clean on what was going on, 95% of current global cases would have been prevented.
Based on 40 years of China watching and the social media information that has trickled out past the censors over the past weeks, my hunch is that the real number of coronavirus casualties In China is at the very least one OM plus several factors and not inconceivably closer to two OM the official 3,300 or so.
To mention China in the same breath as South Korea and Taiwan, countries that have been models of transparency, it missing the point completely (in Dutch: de plank misslaan).
I don’t think he said China was a model of transparency, he said “My favorite countries for a holiday in present circumstances:”
Not quite the same thing. Consider yourself triggered ( and not by Wim’s words ).
Tetris: “To mention China in the same breath as South Korea and Taiwan, countries that have been models of transparency it missing the point completely (in Dutch: de plank misslaan).”
WR: I am well aware of the differences between China, South Korea and Taiwan. And like Greg said, I mentioned them together ‘as a holiday destination’. In regard to protection against the danger of the virus they are the safest destinations these days.
Like you I am well aware about the history of China: during my studies geography I even did a minor in ‘Chinese history’ because I wanted to know more about the old culture and about the communist experiment which at that time still was going on, just because I was interested in what was really happening in China. At that time China was very closed, a complete mystery for people outside of China. And like you I discovered that the ‘official words’ were far from reality.
Later I visited Sjanghai, I think in 1992: the militairy were still very present at the airport and ‘western service’ was not yet common.
I have been very astonished about the big jump the economy in China made after Deng Xiao Ping came into power in 1978. Deng quoted the old proverb “it doesn’t matter whether a cat is black or white, if it catches mice it is a good cat.”
China has been an organised society since three or four thousand years and knew many ups and downs. It shows better than whatever country that the right leadership makes the difference between failure and succes. Deng made the difference; China now has been booming for decades. Many things they do much more efficient than the West from whom (after Japan) China learned how to produce.
I have been following critically the numbers China gave about the virus. I came to the conclusion that for understanding what happened the trend was well enough visible when it became clear to me that what has been measured has been done rather consequent. No big changes in measuring were made without mentioning them. In the end China (and other SE Asian countries nearly completely controlled the virus, while ‘The West’ (Europe, US) said ‘we are prepared’ for the virus but weren’t . We did not have mouth caps (still not), not enough protecting clothing, no pop-up hospitals, no system to control everything needed to secure public health in case of a real dangerous virus etc. etc. Because of a lot of ‘not understanding’ and arrogancy (‘we have the best medical system’) we were not able to keep the virus out of our countries and when it was there we could not test our people in time. This while China and other SE Asian countries had given us one and a half month extra to prepare. They did the good job and we were failing.
So now we need to learn from Asian countries how to continue. And of course we need to find our own way, also learning from all experiments that we are doing ourselves. Our cat will not be black or white: it will have many colors. Changing over time.
Greg: “I don’t see the point you are trying to make about Sweden.”
WR: When you compare the ‘Total Deaths” graphics of Sweden and The Netherlands (the orange lines) you see a regular line in the Netherlands (and also in most other countries) and a ‘bumped’ one for Sweden. Changing what is measured is reflected in those bumps. In the “Daily New Deaths” graphic below orange one you see the irregularity.
In Sweden the virus has the same potential as in other countries. Perhaps the fact that Swedish people live more apart from each other will help do keep the total effect lower than elsewhere. Crowded places have a big disadvantage. And like elsewhere people in Sweden will already be more careful because of all the information they get from elsewhere: Swedes are well informed.
Let’s follow how the Swedish experiment works out.
Greg, Wim
To even reference China – as a holiday spot (not) or otherwise- without explicitly pointing out that we know they’re lying about their numbers, is by extension lending credence to their propaganda.
Taiwan saved its ass because the openly state and operate on the basis that they not believe anything the comes from China. Good example to follow.
Mr. Rost,
The same type of exponential function describes regular influenza.
The public does not fear the flu to the extent that they will allow an economy-wrecking, liberty-smashing, “lock down.”
The public is allowing such a “lock down” over COVID19.
What variable changed?
FEAR factor.
Based, as this post’s author, i cisil, Greg, Willis, and many others have shown, on incompetently handled at best, skewed at worst, data.
That is, the fear you refer to is based not on fact but on misinformation.
It is removed by truth.
Tyranny leaves the fear in place – until the excuse for UNNECESSARY heavy-handedness goes away.
Truth removes the fear and frees people to do only what is rational and NEEDED.
“…the truth shall set you free.”*
*(this quote applies analogously to issues besides one’S eternal destiny)
Dear Mrs. Moore, dear Janice,
Let me first say that I read many of your comments. And I wouldn’t have done so when they weren’t worth to read, partly because they were funny to read but also because I liked your critical view. So where do we diverge?
I have looked at many numbers. And there is one number that has been more scaring than others. This number is even more scaring for the Western world than for China. You can find it on the main page of https://www.worldometers.info/coronavirus/ : the first two graphics.
We know that between the moment of testing and death there are some 8 or 9 days. Therefore the present number of deaths (last number: 69,427, April 5) refers to the number of tested cases eight days ago: 723,390 for March 29. Nearly ten percent (9.6%) of tested cases died, the most in the western world and there are still 46,031 serious or critical ill people.
Compare this number with the WHO (at March 3) estimated 3.4% case fatality rate and with the final outcome for China: 3,331 deaths for 81,708 cases which makes 4.1%.
The overall (!) yearly death rate for the whole population (mortality) for flu is around 0.1%. The medical system is able to handle these quantities. If 70% of the population becomes infected with the corona virus (in a very short time, several months) the death rate will be 70% of a percentage between 3.4% and 9.6%. The outcome will be that this virus is much more virulent than flu, some 34 to 96 times and even when the number of non tested (asymptomatic and very mild) cases is half of the total number of infected people this virus is 17 to 48 times as deadly and disruptive. The virus is also called SARS-CoV-2 and we already knew the potential of SARS.
Who reads about the Spanish flu (1918) can only imagine that at that time (when there was no organized lockdown) many societies also (!) came to a standstill by that epidemic. This has not been well noticed because all societies and economies already were upside down because of the First World War.
While this virus follows the same graphics as flu, the magnitude of this virus is of another order. In my view: disrupting societies and economies anyhow – if uncontrolled and even when only temporary not-controlled.
As I argued elsewhere* we are fearful because we don’t control this virus. We (in the West) have never been prepared for this virus. We were preparing for imaginary [environmental] problems that ‘might – could – may’ happen – ‘if’ and ‘when’ – etc. in the year 2100. That failure in mainstream thinking has been dominating tens of years and now we are paying the price for our ‘not being prepared’ for a real danger. We only have the choice between an economic disruption and a societal disruption or a combination of the two. All three options plus the direct impact of the virus on individuals and their families are causing damage and are causing fear. Either way, we are already “in the middle of it”.
The ‘good’ news is that when everyone is ‘social distancing’ and when someone else would be able to produce many billions of facemasks for the period directly after the first wave (hopefully soon) we can regain control of the virus until we have a better solution. Than we only have to find smart solutions to fully restart the economy.
* https://wattsupwiththat.com/2020/04/01/do-lockdowns-work/#comment-2954405
Dear Wim,
How kind of you to tell me that…. You really encouraged me….
I have said enough (for now, heh). I would just like to be friends.
So, as we sit, you and I, at this table in the town square, you with your cup of strong Dutch koffee, me with my cup of sweetened Darjeeling, I hand you the plate of chocolate chip cookies and say, “Please, help yourself.”
Take care, over there.
Janice
#(:))
P.S. My Swiss (German) friend has addressed her greeting cards to me “Mrs.” also (and she knows that I am single). Unlike “Frau” (or “Vrau”), “Mrs.” is used only by married women in the U.S.. Even widows (unless they were born before ~1940) do not use “Mrs..”.
Most of us single women and MANY married women (such as myself, back then….) use “Ms.”. Very few use “Miss” (unless she is a grade school teacher – it is more commonly used there – easier for a lot of little kids to say for some reason).
“Mrs. Moore” is my mom 🙂
There. Perhaps, that information will be useful to you. And, lol, perhaps, it will just amuse you. Either way – worth sharing. 🙂
Ms. Moore: “Mrs. Moore” is my mom 🙂
WR: Thanks Janice, next time I will write to you! 🙂
🙂
Nice to see you pop up now and again Janice with your special brand of kick @ur momisugly$$ attitude, humor and prodigious eclectic info. The mass media and control freak politics have made so many people timid and unresourceful. We used to be tough to herd around.
When I was a kid, there weren’t antibiotics and families were quarantined (quarante = 40 (days)) if someone came down with scarlet fever or a host of other untreatable diseases. We live in a comparative paradise, abundant food, goods, clean air, water… and were sick with fear because of the constant barage of end of world fear mongering by the left.
Keep at it Janice!
Gary! Thank you 🙂
Good to see you, too. I was glad to read that you did not get polio. That appeared to me to be a very close call. And, though you probably don’t, I thanked God.
Sure was kind of you to take the time to say hello.
Thank you.
And, yes, indeed, so easily led….. Perhaps, it is not because people are more stupid or lazy about research or have weaker characters than it is because of the HUGE propaganda machine most of the mainstream news sources have become.
People are pretty much the same – just being fooled instead of informed.
Take care.
Many countries already do that on a death certificate, if the death cause is not clear the body is sent for autopsy to make a finding. You are singling out Sweden as doing something no-one else does which is incorrect. I can only speak for the Australia system where the official figures are as per death certificate and there is no “with” numbers involved.
Apparently, they’ve stopped doing autopsies in Germany under the pretext that it is too dangerous, which is nonsense because they already have the capability to safely do autopsies for ebola and prion disease.
https://swprs.org/a-swiss-doctor-on-covid-19/
My first comment went into moderation because of the “k” word. Instead of me reposting, search for this in this link:
“The German Robert Koch Institute now advises against autopsies of test-positive deceased persons”
https://swprs.org/a-swiss-doctor-on-covid-19/
Yes exactly. Please can the other contributors on this topic on this site please read this excellent summary and take it on board before they pen their next pieces. (Though one still seemed to be under the impression that reported cases is a helpful variable for comparison, which has surely been completely debunked by now.)
In comparing countries, deaths are by far the most accurate statististics – number of infected is wildly inaccurate. Note that at one point the U.S. supposedly had half the infected but only one eighth the deaths worldwide. Either our healthcare system is wildly more efficient than other advanced countries, or the infected numbers are wildly understated.
I am willing to wager a case of Modello that total deaths in the US in March 2020 is less than March 2019. The implementation of the restriction of economic activity will overcome any increase due to the virus. The infection has been consistent in every state since the beginning of testing. We are 4-6 weeks further into this pandemic than anticipated due to asymptomatic patients not being counted.
No wagers, Marty. Too much hysteria and false data.
I am of two minds on this. It’s wonderful that my countrymen are self isolating in order to protect the health of their elders. On the other hand I am reminded of this piece of wisdom from an old Icelander to wit, “Ships are safe in harbors but ships are not meant to stay in harbor.”
The people of Ecuador decided to party hardy even when the government advised them to isolate. Because of their already weak infrastructure, they now have bodies waiting in the streets to be picked up by ambulances that never come.
On the other hand, if we truly wreck the economy trying to stay safe, how could that be called wise? We don’t want to drag ourselves down to the level of Ecuador. Life expectancy in Ecuador is about 77 years. In Canada it is about 82 years. link Chopping five years off our life expectancy trying to protect ourselves from coronavirus (and wrecking the economy in the process) has to be counterproductive.
We are in the midst of a huge experiment. I hope we learn from the experience.
You’re making an assumption that they all died from coronavirus. There’s little testing.
Do you have any links to reports from Ecuador? The latest info I can find is that there have
been 3465 cases and 180 deaths in Ecuador which while bad is not so bad that bodies are lying in the street. Canda has a much higher number of cases (15443 which is about twice the rate that Ecuador is reporting) and a higher number of deaths (277 which is better than Ecuador which is not surprising given the better healthcare available).
Here’s a link, and another link.
One story says the undertaker couldn’t get out to collect the bodies because of a curfew. It could be true but I’m taking it with a grain of salt. The other possibility is that the numbers are much worse than reported.
US is way behind Taiwan in restricting the CV19 case load. Taiwan government is injecting just USD2bn into its economy to offset loss of Chinese tourism – way less than US needed per head of population to keep food on many tables. Taiwan is predicting 2% growth in 2020.
Australian response was faster and more decisive than the USA. Australia has been quite effective in flattening the cumulative curve to date:
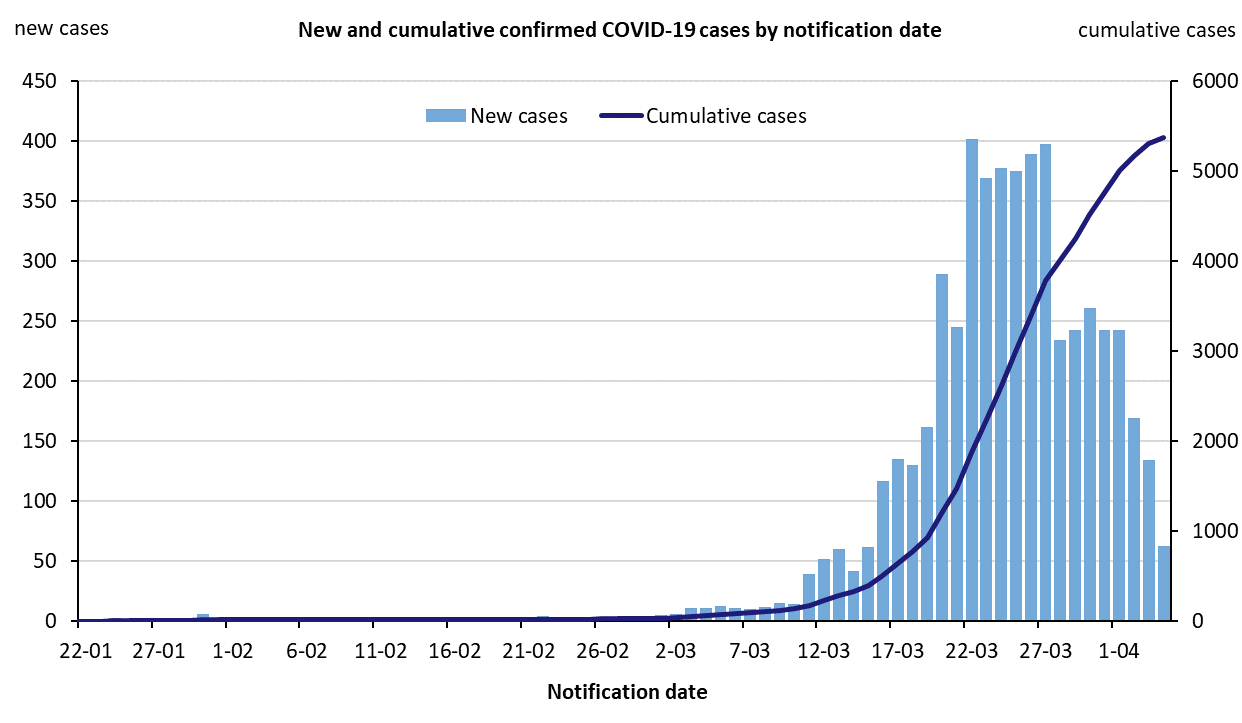 ?itok=TSijkOvq
?itok=TSijkOvq
Death rate in 1.5deaths/M compared with 29deaths/million in USA.
Australia is considering legal action against USA/UK dual listed Carnival Corporation/Carnival PLC for it contribution to CV19 deaths in Australia – about 20% of deaths can be traced to Ruby Princess.
Lies, damned lies and statistics. h/t Mark Twain
Basically, all these “experts” are farting numbers out their @ur momisugly$$e$. No one, even the doctors calling the deaths, knows what the PRIMARY cause of death is. Being definitive costs money and doesn’t really change anything.
This entire “pandemic” is a complete fabrication to destroy the world’s economy, increase the power and control of the state, and create profit for a few at the expense of the many.
And if you think that the “numbers” they come up with in a year or two will be any more accurate (strike that) accurate in ANY way, you are a complete idiot. What country will benefit in ANY way if they report accurate or even vaguely realistic numbers? NONE. The ONLY motivation is to profit off the panic, not prepare for the next pandemic.
And that angry emoticon is d@ur momisuglymn right I’m pissed off. (that’s for another site that analyzes your comment and offers to help you make it a happy comment)
Full agreement. When and if Joe and Mary general public comprehend what has been done to them over the last few months there will be hell to pay, and rightfully so. I’m disgusted by the scare mongering across all media outlets.
Sweden has this right. One of the few times for them.
My question which machivellian group or individual dreamt this up, I’m convinced someone did, and I have to look to the Orient.
Sweden is now paying medical staff double normal salary to get them to face up to the growing case load. That does not happen in annual flu season.
https://sverigesradio.se/sida/artikel.aspx?programid=4916&artikel=7445789
Most of the Swedish population are not dingbats either. They are self-isolating irrespective of the lack of government enforced controls:
https://www.gstatic.com/covid19/mobility/2020-03-29_SE_Mobility_Report_en.pdf
The US is infested with dingbats as evidenced by the number of Climate true believers. Without government controls those dingbats would be happily hosting the dangerous virus that leads to CV19 deaths.
I have lost all respect for Mockton as as ann intelligent assessor scientist which he does not appear to be from his 1,5 AGW warming calculations which mean nothing it could be minus 2 anyway he appears just to be a a high froliking British politician with some knowlegde of mathematics and physics good for him and I have published 27 articles in biology veterinary science and viruses (Elsevier) my father attended classes with Einstein so for his confomt so now lets exagerate his death from coronaviruses 10000 per day from this deadly virus to satisfy his stupid cravings of death so now we have normally 170000 people dying per day normally lets say there are 80000 deaths from his coronavirus to date to satisfly his date so lets say 80000 dioe from corinavirus over 4 months that is 80000/120days = 665 per per day WORLWIde Please provide me with data that this deviates from the normal death rate. The British Scientists arenow amongst the most ignorant scientific people in the world they used to be the smartest look up roman empite same story
Guest essay by Indur M. Goklany
roman empite = Roman empire?
CofB is a highly intelligent chap but he is also a macheavelian manipulator. That is why I have been critical and mistrusting of him even when he was on the “right” side of the climate issue.
Sorry, using the estimated flu numbers to challenge the severity of COVID-19 is just meaningless bc the numbers are just that: an estimate. Nobody confirmed them. Confirmed flu deaths are in the hundreds for many countries.
Excess mortality by average for communities – not whole countries – might be the only somewhat reliable comparison though there will be still a lot of positive and negative confounding factors.
Been doing this for weeks. Total Mortality will show up an epidemic if one exists, and show how big it is relative to other epidemics…
While the data from the nchs is incomplete with lots of caveats, the difference is very large to what is reported in the MSM. As of April 3,2020 the number of US deaths from COVID stood at 1,150 . Here is the link
https://www.cdc.gov/nchs/nvss/vsrr/COVID19/index.htm
eo April 5, 2020 at 4:41 pm
Thanks for the link.
It’s very difficult to know who or what to believe. The CDC, the news media or family members who are medical professionals.
Oh, I’ve bookmarked that link and will watch it.
the antigen test is more useful to determine if the herd immunity is working. Some people or most of the population could have been already infected by the they did not show any symptoms or the symptoms could be so mild it does not even warrant seeing a doctor. Testing if the individual is positive or infected will only cause further hysteria and possibly psychosomatic reaction further overloading the health system and worst could result to serious mental health problems. The hysteria is causing serious problems especially in areas with very low educational levels. Health workers are being socially abused and stigmatized for potentially spreading the virus in the community.
it’s the “highly educated” that are pushing the hysteria
That’s not reasonable. If people who are not sick now are given antibody tests that show that they are immune and have certainty (ok near certainty) that they have nothing further to fear, you think that somehow that will make them panic? Even those who test positive with mild or no symptoms know that they have about 14 days to the point of immunity. And those mild and asymptomatic cases are the ideal candidates for hydroxychloroquine treatment. Those who have serious symptoms NEED to know what they are facing and probably more than 50% will find out that they have something less serious than covid-19. So who are the people who are going to panic?
If people can be shown to be immune, those people go back to work and bring our economy back. How can you oppose that? Not testing is a choice to continue in ignorance, most likely worrying when there is nothing to fear.
Bear in mind as I proposed earlier, appropriate testing needs to combine active infection (swab test) with immunity (antibody finger-stick blood test).
Is there any certainty that immune means not a carrier?
Is there any certainty that antibody presence means immune?
AndyHce—
Please read my comment directly above yours. That is why the swab test must be administered along with the immunity blood test. Otherwise the person showing immunity could still be contagious.
Now I’m sure some will think about the risks of false negative on infection combined with a positive immunity test. That is why we need to continue social distancing even after returning to work.
Not sure if someone could calculate it, but the risk of a false negative infection/positive immunity test result leading to infecting somebody despite masks and social distancing needs to be balanced against the certainty of economic depression causing deaths.
You could also condition the return to work on a number of days after the positive immunity test, to reduce the impact of any false negative infection test.
We’ve got to get back to work as soon as possible! There isn’t any certainty in life. We always need to balance risks. Would you pay a million dollars for a $100,000 life insurance policy?
The question has to be asked as to whether the Wuhan coronavirus effects the ability of the body to deal with comorbidities like AIDS which kills in the same way by not being a direct cause of death.
This is a rather nice visualization that bears on the essay. It compares COVID_19 deaths to the average of 15 daily causes of death in the US over the month of March.
https://public.flourish.studio/visualisation/1712761/
This is data, not models. From last to third in a month. My guess is number one with a bullet nationally on the Billboard charts inside of 10 more days. Exponential growth is like that.
That’s why the egregious lockdown is the only thing that has a chance of working (eventually — 3 week delay between infection and death). We missed our chance to follow South Korea, test like crazy immediately starting in January, not mid-March, and actually control the spread. The Center for Disease Control forgot that its name is its mission.
I think if we tested grocery store workers, hardware store workers ( essential business) we could cut down in spread even more. Basically anyone that interacts with public or works in buildings that the public still goes to.
Maybe we could put a star on their foreheads 😉
How about let the things end (the possible pandemic) to analyse data, taking all the possible factors into account to make some ideas and then elaborate hypotheses and finally and hopefully take some conclusions… You all seem like climate alarmists about the Covid-19 these days… quick conclusions about partial or flawed data.
JN,
When lives are in IMMEDIATE jeopardy from a real measurable threat, you use what data you have, and recompute as new data comes in. Not the same situation as CAGW at all. I wish people would stop comparing the two. My jeep and an F1 race car both have four wheels and an internal combustion engine, but nobody would seriously compare them.
At least, I would hope that would be the case, so we can look back and see that some good came of our flattening our economy. At least one can hope…
—————————
And at last people will understand and finally accept that Obumer deserves a proper Nobel Price for saving the World from the sea level rise.
And WHO definitely should be awarded a Nobel Peace price sharing it with UN and Italian and maybe SK governments.
That will be some good balsam for the Global economical severe wound there.
And very refreshing, comforting and reassuring to the masses…
One only can hope… for such mesmerizing “cheering” victories.
And all will go back to some new normal in the farm.
cheers
How do we trust that standards for measuring and recording are consistent from country to country or from region to region? I’m still not convinced that the numbers are worth fussing over.
Comparing apples to frogs makes little sense.
Also, how can we assume that testing does not have a saturation point, where the max number of people who will test do test, while other people carrying the virus with minimal effects do not care to be tested, and all the people who are willing to be tested HAVE been tested at a particular point?
Escalation of people getting tested and found positive does NOT mean an escalation of cases per se. There may be so many more cases out there that simply never make it to testing, out of choice or circumstance, and we can NEVER know those numbers, because the people simply get over there symptoms and get on with life.
We should have had “Corona” Serum Antibody Tests available months ago to get THE MOST IMPORTANT DATA required to manage an epidemic…namely the number of people who have had the infection. Currently estimates run between 0.1% (the confirmed cases) and 35% (from models like the one cited 4 weeks ago by the Director of the Ohio Health Department). Somewhere between 330,000 cases and 115,000,000 cases. It’s 100% certain that it’s way over 330,000…but it might actually be more than the 115 million…WE. DON’T. KNOW.
That is absolutely NOT GOOD ENOUGH. It borders on criminal malpractice. It is certainly Outrageously bad science and terrible public health management.
We have been UNNECESSARILY flying blind managing an epidemic that threatens the WHOLE ECONOMY without good infection rate data. Singapore was using Antibody Testing WAY BACK IN FEBRUARY…it wasn’t a perfect test…but it was far better than flying blind. And much can be learned about Antibody Testing (for a specific virus) by using even imperfect tests (and it’s not hurting anybody doing the tests).
Fauci admitted (during a Press briefing) that the CDC has not made Antibody Tests a Priority. What? Why the hell not? Accelerating the development of Antibody Tests would in no way hinder any of our other efforts. And it would have better informed us on the best course to take with $TRILLIONS and many thousands of lives at stake.
It’s like the CDC and the FDA wanted to avoid having any data that might argue against keeping the lockdown in effect past the end of April. Why else not do something so doable?
The FDA has finally approved 1 Antibody Test (Cellex)…and several more tests are close to approval. If the CDC had made the Antibody Tests a priority from the start, we would now have a GREAT DEAL MORE KEY INFORMATION required for intelligent epidemic management.
I’m fairly certain that I had the virus (my doctor agrees…it was his provisional diagnosis) but I need to know for sure. Everybody should know if they have Antibodies against the virus and are immune…and would be able to go back to work or freely socialize. Getting everybody (who wants it) that crucial information should have been a TOP PRIORITY from the very start.
Even a fairly poor test (say with 10% false positives) would provide ~100 times more accuracy than we have now about the % of our population who have had the infection and are now immune. Right now we have virtually no idea. That is REALLY BAD SCIENCE…and really bad PUBLIC HEALTH management.
Anytime a so called scientist shows no concern about the lack of a key bit of information THAT IS EASILY GOTTEN (like Fauci did publicly)…you can be certain that the scientist (or Public Health Official) is not really engaged in a valid scientific endeavor…and is not doing a good job of managing an epidemic.
Docsiders do you know how often false positives and false negatives occur from this test?
Could you point to a good source for information on Cellex?
Thanks
I searched high and low for the Cellex false positive and false negative numbers to no avail. But the FDA criteria is > 95% accuracy for the EUA approval.
False positives less than 5% would provide substantial and nearly perfect protection for a well designed “go back to work” plan.
Going back to work would expose worker #1 to fewer than 50 other tested workers (per the plan)…so on average worker is exposed to half a worker (worker 2). Worker 2 has been feeling well for over 2 weeks and has not run a temperature the last 2 weeks (mandatory testing at work) so communicabity is not very likely (social distancing and good viral hygiene is practiced at work). Plus now we know awfully well where any hot spots are in the country where Viral and Antibody testing gets stepped up. Strict quarantine of vulnerable people (the ones likely to get very ill or die) is tightened up (taking the pressure of the healthcare system).
We are doing none of this rational management because the FDA and the CDC were ok with waiting for a more perfect test…while the economy burned.
Meanwhile, anybody with a positive Virus test triggers Antibody testing of all contacts the last several weeks, and any positive results triggers more tracking.
That’s how an epidemic is managed…and a key ingredient is an Antibidy Test…even a bad one with a 10% false positive rate like the one used 6 weeks ago in Singapore…that was not used forensically in the US.
That’s evidence of maddening incompetence or wickedly totally evil intentional mismanagement.
Docsiders, I saw a clip of that briefing, one of Laura Ingraham’s videos available on the internet (saw it just yesterday), with Dr. Birx following Dr. Fauci to assure us that antibody testing is being made a priority *now*.
I wonder how much of this is bad experts leading the way, or is it just experts running as panicky as they think they must, pressured by a press-says-do something-this-instant mentality? If gathering key bits of evidence was not perceived as doing much of anything to “save lives”, then I agree with you, it sure does seem like bad procedure.
Nice article Anthony! Its really good to have a guy like you setting the record straight without bias.