Guest Essay by Kip Hansen – 27 November 2020

There has been massive media attention on Covid-19 deaths – and there have been a lot of them. The CDC as of noon on 26 November 2020 was reporting that there have been 259,005 total Covid-19 deaths in the United States.
Yet anyone who reads widely is aware that there have been reports of a motorcycle accident victim being reported as a Covid death. There are many who correctly report that all people dying from or with Covid and even suspected of dying from-or-with Covid-19 are all being counted as certified reportable must-make-the-headlines Covid-19 Deaths.
[Note: This is a long and rather detailed explanation of what leads to the situation in which we find ourselves regarding Covid-19 Deaths reporting. Those who want a better understanding of the issue should continue reading. Readers with no or little interest can just accept this brief synopsis: “It’s Complicated” and move on to other posts. ]
Various experts, journalists, bloggers, and pundits tells us that “Covid Deaths” are being over-counted, mis-counted and even under-counted. Other pundits and media-reported experts desperately try to reassure us that Covid Death counts are correct and real – and that we should all stay concerned and follow all government mandates – which vary from “reasonable” to “obviously based on magical thinking” (closing bars and restaurants at 10 PM because that’s when the Corona Virus Zombies attack) — all this despite various governments having different and contradictory mandates (or even an absence of mandates) and the various States in the United States following differing rules and policies on Covid Deaths reporting. Those reporting “facts” like “US Covid-19 Deaths overestimated by 17 times” (based on this CDC comorbitity data) are sadly mistaken and misinform the general public, just adding to the general confusion on the subject.
Doctors, Coroners and Medical Examiners will calmly explain that “Cause of Death” is complicated and not simple. And they are right. Most of us think that when a person dies, it is obvious what killed him/her. But that is just not the case. In fact, everyone dies of a combination of ”heart stoppage” [cardiac arrest] and “cessation of breathing” which eventually leads to “brain death”. But these are not usually listed as the Cause of Death on a death certificate.
Covid Deaths are being counted and reported based on advice from the CDC, who has based its advice on advice from the Council of State and Territorial Epidemiologists (.pdf). More on what that means later.
The Primer: What is meant by Cause of Death?
When a person dies in a hospital or other setting, there is some doctor, coroner or medical examiner that fills out a death certificate – officially certifying that John/Jane Doe has died and reports the date, time, place, Social Security number and other personal details along with the circumstances and sequence of events that led to that death.
Here’s a CDC-annotated image of the Cause of Death portion of a typical death certificate:

We are interested here only in Parts I and II.
“Part I
This section on the death certificate is for reporting the sequence of conditions that led directly to death. The immediate cause of death, which is the disease or condition that directly preceded death and is not necessarily the underlying cause of death (UCOD), should be reported on line a. The conditions that led to the immediate cause of death should be reported in a logical sequence in terms of time and etiology below it.
The UCOD, which is “(a) the disease or injury which initiated the train of morbid events leading directly to death or (b) the circumstances of the accident or violence which produced the fatal injury” (7), should be reported on the lowest line used in Part I.”
[ source: CDC here – .pdf ]
Let’s look at a CDC example:
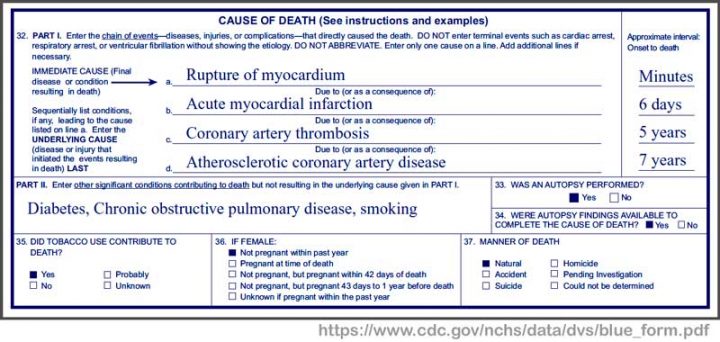
This patient had Coronary Artery Disease for seven years — which led to Coronary artery thrombosis from which the patient suffered for 5 years — which led to Acute myocardial infarction (heart attack) after which he survived for 6 days until — his heart ruptured resulting in death within minutes. Conditions contributing to his/her death were diabetes, COPD, and smoking. Each of these “significant conditions contributing to death, but not resulting in the underlying cause” are themselves known to cause a wide range of other serious conditions. For instance, smoking is believed to cause COPD and heart disease. Diabetes can cause cardiovascular diseases “including coronary artery disease with chest pain (angina), heart attack, stroke and narrowing of arteries (atherosclerosis).” Notice that there is a dedicated section “35” asking “Did tobacco use contribute to death?” For this patient, the doctor chose “Yes” – thus the CDC will count this death as one of the 480,000 annual tobacco deaths.
Let’s look at another example (from the same document):
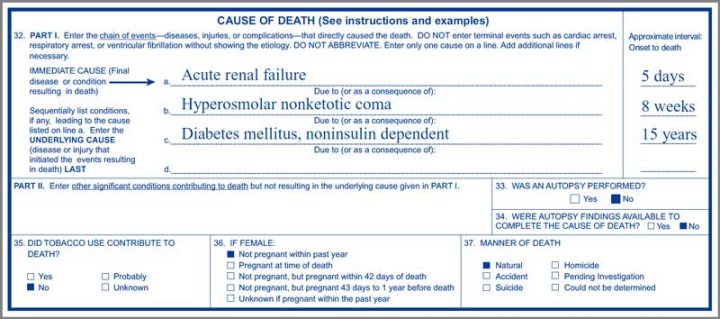
This person suffered from noninsulin dependent Diabetes mellitus, often called Type 2 Diabetes, for 15 years. As sometimes happens, this diabetes sufferer eventually went into a Hyperosmolar nonketotic coma in which she/he remained for 8 weeks before finally succumbing to Acute renal failure (kidney failure). The family of the patient would have told friends and neighbors that their loved one died of kidney failure. They may have mentioned this was probably the end-of-line result of his/her long-term diabetes. Type 2 Diabetes is known to cause the following conditions: Heart and blood vessel diseases, Nerve damage (neuropathy), Kidney damage (as in this patient), Eye damage, Slow healing, Hearing impairment, and even Alzheimer’s disease.
It is clear that this second patient died of acute kidney failure – “Acute kidney failure is most common in people who are already hospitalized, particularly in critically ill people who need intensive care” — and is not necessarily a direct result of diabetes – but assumed in this case as kidney damage can be caused by diabetes. The death certificate Part I sequence is reasonable and represents the doctor’s professional opinion.
“In certifying the cause of death, any disease, abnormality, injury, or poisoning, if believed to have adversely affected the decedent, should be reported. If the use of alcohol and/or other substance, a smoking history, or a recent pregnancy, injury, or surgery was believed to have contributed to death, then this condition should be reported. The conditions present at the time of death may be completely unrelated, arising independently of each other; or they may be causally related to each other, that is, one condition may lead to another which in turn leads to a third condition, and so forth. Death may also result from the combined effect of two or more conditions.”
Source CDC Medical Examiners’ and Coroners’ Handbook on Death Registration (.pdf)
So, you call the Cause of Death of these two patients. What was the Cause of Death of each? Did diabetes kill them both? The first patient via atherosclerosis which kicked off the sequence in Part I? The second from the diabetes induced coma or was the coma from simply caused by being in intensive care? Or was it the first patient’s life-long cigarette smoking causing the coronary artery disease? Or would you, as this doctor did, start the death sequence with his/her seven years of Atherosclerotic coronary artery disease? In each case, there are several sequences that would be reasonable and could have been correctly entered by the attending physician, a coroner, or later by a medical examiner.
The above are pretty common examples – long-term conditions which lead to the next condition that finally leads to death. We don’t see the personal information part of the Death Certificate so we don’t know the age of these patients. The age of the patient is often key to Cause of Death – but is not to be used as a cause itself.
“Common problems in death certification
The elderly decedent should have a clear and distinct etiological sequence for cause of death, if possible. Terms such as senescence, infirmity, old age, and advanced age have little value for public health or medical research. Age is recorded elsewhere on the certificate. When a number of conditions resulted in death, the physician should choose the single sequence that, in his or her opinion, best describes the process leading to death, and place any other pertinent conditions in Part II.” [ source: CDC my bolds – kh ]
And then this:
“For statistical and research purposes, it is important that the causes of death and, in particular, the underlying cause of death, be reported as specifically and as precisely as possible. Careful reporting results in statistics for both underlying and multiple causes of death (i.e., all conditions mentioned on a death certificate) reflecting the best medical opinion.
Every cause-of-death statement is coded and tabulated in the statistical offices according to the latest revision of the International Classification of Diseases. “
Source CDC Medical Examiners’ and Coroners’ Handbook on Death Registration (.pdf) – my bold — kh
There are over 69,000 ICD-10 diagnostic codes. Someone goes through every death certificate filed and translates the diseases and conditions the doctors, coroners and medical examiners enter in Parts I and II into ICD-10 codes (soon to be ICD-11 codes). There are so many codes that there are many online look-up tools and apps to help medical staff code up office visits and others to code up Cause of Death certificates. The first Death Certificate above might be coded: “ E08.01 Diabetes mellitus due to underlying condition with hyperosmolarity with coma” – which would cover Part I lines “c” and “b”. This diagnosis is billable. This app helpfully informs the staff if the ICD-10 code they select is “billable” – if not billable, we can safely suspect that office assistants coding office visits can search for a true but alternate diagnostic code that is billable. “All conditions mentioned on a death certificate” are translated to ICD-10 codes and eventually tabulated “for statistical and research purposes”. In our two sample Death Certificates, there are ten different diseases and conditions mentioned. Thus each of the ten condition codes eventually, at the CDC and WHO level, gets a little “tick-mark” – a plus one – added to the number of deaths involving that ICD-10 code.
Thus the huge number of deaths reported for which smoking is claimed to be the cause, as we see in this next quote from the CDC:
“Smoking is the leading cause of preventable death.Worldwide, tobacco use causes more than 7 million deaths per year. If the pattern of smoking all over the globe doesn’t change, more than 8 million people a year will die from diseases related to tobacco use by 2030.
Cigarette smoking is responsible for more than 480,000 deaths per year in the United States, including more than 41,000 deaths resulting from secondhand smoke exposure. This is about one in five deaths annually, or 1,300 deaths every day.”
[ source: CDC here ]
Most people simply accept those statements as fact, though they know of no one who put a cigarette in their mouth, lit up, and died as a direct result. Through many years of public health anti-smoking/anti-tobacco education we have been taught that smoking or otherwise using tobacco can lead to a long list of health problems, many of which cause or contribute to the eventual death of the smoker. In this case, a life-time of tobacco use is referred to, by public health officials, as a “cause” of death – though it probably would not be listed as a cause on a death certificate. Despite not being listed as a cause on the Death Certificate, the CDC and WHO unequivocally tells us that smoking is “the leading cause of preventable death”.
As in many complicated subjects, there are varying definitions in use for the same terms – in this case “cause of death”. There is the general everyday use – like “something that directly causes the death of a person, if it hadn’t happened, they wouldn’t have died”. So, a person gets lung cancer, probably or presumably because they had been a life-long smoker, and dies from the lung cancer. We know they died of lung cancer but accept that smoking led to that death. It is this definition that the WHO uses above. But it is not the official definition that is to be used on a Death Certificate as Cause of Death, which is in the quote far above, labelled Part I.
Those readers who watch any of the popular crime and police television series know that Cause of Death in trauma deaths is even more complicated — “homicide, accident or suicide?” — though those TV Medical Examiners are always portrayed as having almost paranormal insight – “blunt trauma to the head…but that’s not what killed him.”
One last quote from the handbook for medical examiners:
“Precision of knowledge required to complete death certificate items
The cause-of-death section in the medical examiner’s or coroner’s certification is always a medical opinion. This opinion is, of course, a synthesis of all information derived from both the investigation into the circumstances surrounding the death …. It represents the best effort of the medical examiner or coroner to reduce to a few words his or her entire synthesis of the cause of death.”
[ emphasis in the original – kh ]
Bottom Line: Cause of Death determination and reporting is complicated and highly dependent on the training and opinion of the person making the report.
# # # # #
Reporting of Covid-19 Deaths
Here’s the pivot point on Covid-19 Deaths:
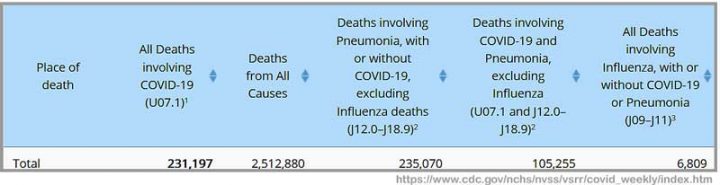
This is from the CDC’s weekly Covid report. See the Column 2 heading? It says “All Deaths Involving Covid-19 (U07.1)1”. The keyword is INVOLVING. To be perfectly clear, what is being reported by the CDC, as collected by the National Center for Health Statistics, are All (every one) Deaths (people dying) that Involved Covid-19. See the little footnote indicator “1”?
Footnote 1 says: “COVID-19 deaths are identified using a new ICD–10 code. When COVID-19 is reported as a cause of death – or when it is listed as a “probable” or “presumed” cause — the death is coded as U07.1. This can include cases with or without laboratory confirmation.”
Not just verified cases in which Covid-19 was the immediate cause of death. At least, to be even clearer, not necessarily what you, the average reader, would consider THE cause of death.
So, what exactly are they counting when the CDC and WHO report Covid-10 Covid-19 Deaths? The World Health Organization’s official guidelines are:
2. DEFINITION FOR DEATHS DUE TO COVID-19
A death due to COVID-19 is defined for surveillance purposes as a death resulting from a clinically compatible illness, in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID disease (e.g. trauma). ….
A- RECORDING COVID-19 ON THE MEDICAL CERTIFICATE OF CAUSE OF DEATH
COVID-19 should be recorded on the medical certificate of cause of death for ALL decedents where the disease caused, or is assumed to have caused, or contributed to death.
[ my emphasis – kh source: WHO here .pdf ]
Note that the Death Certificate — Cause of Death Part II is “Other significant conditions contributing to…”. So, there is where Covid-19 (ICD code U07.1) would be written for any death in which Covid wasn’t “caused, or is assumed to have caused” but only contributed to the death. If the decedent was a “Covid case” then he/she becomes a “Covid Death” if they die. Read on . . .
For the general public, who want to know “How many people are being killed by the SARS-CoV-2 Pandemic?”, this definition does not supply the answer to their question. The vagueness and breadth of these definitions is exacerbated, in this “possibly-too-broad” sense, by the definitions being used to define “What is a Covid-19 case?”. We see that the WHO definition of a Covid death includes “a probable or confirmedCOVID-19 case”.
So, how do WHO and the CDC define or advise doctors how to define/determine a Covid-19 case?
Clinical Criteria
At least two of the following symptoms: fever (measured or subjective), chills, rigors, myalgia, headache, sore throat, new olfactory and taste disorder(s)
OR
At least one of the following symptoms: cough, shortness of breath, or difficulty breathing
OR
Severe respiratory illness with at least one of the following:
Clinical or radiographic evidence of pneumonia, OR
Acute respiratory distress syndrome (ARDS).
AND
No alternative more likely diagnosis
[ source: CDC here ]
So, by this definition, I could at this very moment be declared to be a Covid-19 case. I have muscle pain (myalgia) and a headache — two symptoms – — and yesterday, I had a cough — and, if I have reported to the ER and doctors are both rushed and spooked by the pandemic, there might be “no alternative more likely diagnosis”, in their minds at least. (Of course, I have these symptoms for reasons well known to me and my personal physician but this might not save me in the ER.) Especially if they also ask me a bunch of epidemiological questions:
“Epidemiologic Linkage
One or more of the following exposures in the 14 days before onset of symptoms:
Close contact** with a confirmed or probable case of COVID-19 disease;
OR
Close contact** with a person with:
clinically compatible illness
AND
linkage to a confirmed case of COVID-19 disease.
Travel to or residence in an area with sustained, ongoing community transmission of SARS-CoV-2.
Member of a risk cohort as defined by public health authorities during an outbreak.
**Close contact is defined as being within 6 feet for at least a period of 10 minutes to 30 minutes or more depending upon the exposure. In healthcare settings, this may be defined as exposures of greater than a few minutes or more. Data are insufficient to precisely define the duration of exposure that constitutes prolonged exposure and thus a close contact.”
[ source: see previous quote ]
So, if I were in the Emergency Room, the ER doctor might ask me these questions: Do you know anyone who isn’t feeling well? Have you been in close contact with them for more than 10 minutes? Have you attended any meeting with more than 10 people in the last 14 days? Have you been to church or a party? Have you visited a restaurant or a bar? Any YES epidemiologically qualifies me as a Covid case. More questions: Do you wear a face mask whenever you are out of your own home? in your car? in WalMart? at the park? while mountain biking? Any NO qualifies me as a Covid case epidemiologically.
You can see how easy it is to be classified as a Covid-19 case. And they haven’t even tested me yet. (Read the link to see why even testing wouldn’t save me.) They would report me as a Covid case even if I tested negative – I might not be positive “yet”.
And while I describe my pending Covid-19 Case classification jokingly, it is a very real scenario. And, heaven forbid, were I to die of almost anything (except obvious trauma) in the next 14 days, I would become another Covid-19 Death statistic.
As most of us know by now, advanced age is a key factor in the vast majority of Covid-19 deaths:
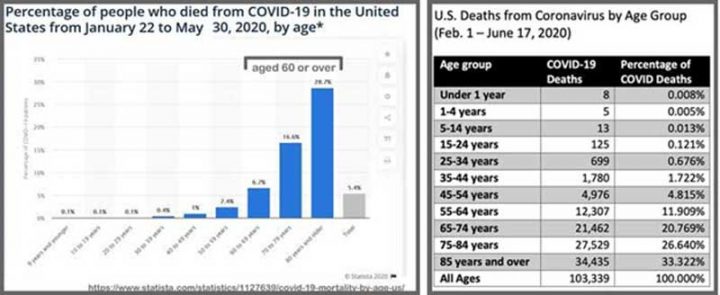
Eighty percent (80%) of Covid-19 deaths are of those 65 years of age of or older – and a full one-third of the deaths occur in those over 85 years. If you are an adult today, then you were born between 1925 and 2000. At your birth, you could expect to live (life expectancy at birth) between 58 to 72 years, depending on your birth year. Those who are dying at 85 or older had a life expectancy at birth of less than 61 years. [My life expectancy at birth was about 66 years – so I have beaten the odds and hope to continue to do so for many years more.]
If this does not seem significant to you, I’ll repeat the CDC quote on reporting cause of death for the elderly – those 65 year of age or older.
“Common problems in death certification: The elderly decedent should have a clear and distinct etiological sequence for cause of death, if possible. Terms such as senescence, infirmity, old age, and advanced age have little value for public health or medical research. Age is recorded elsewhere on the certificate. When a number of conditions resulted in death, the physician should choose the single sequence that, in his or her opinion, best describes the process leading to death, and place any other pertinent conditions in Part II.” [ source: CDC my bolds – kh ]
For the elderly, the aged, the older citizen, which comprise the majority (80%) of Covid-19 deaths, any illness or condition that leads to breathing problems is prone to being classified as a Covid case, and thus a Covid-19 death in “a clinically compatible illness, in a probable or confirmed COVID-19 case”.
Bottom Lines:
- It is complicated.
- Make no mistake, there are lots of people dying deaths that involve confirmed, assumed, or suspected Covid-19.
- Somewhere between “Most” and “Almost All” of those deaths involved other conditions that were already killing the patients – sometimes slowly, sometimes rapidly.
- The official health organizations have their own reasons for what they are counting and they are counting exactly what they say they are counting – but it is not what you or I would expect them to count. They are counting, as the CDC does, “All Deaths Involving Covid-19”.
- The Covid-19 Death statistics represent the counts of the WHO, the CDC and other National and State public health agencies. The general public often mistakenly thinks those counts mean deaths in which Covid-19 was the immediate cause of death – deaths in which the person was killed by Covid-19. That is not the case – it is far more complicated than that.
- The common citizen would have grave doubts about including each and every one of those dead people in the count of “Deaths Caused by Covid-19” if they were tasked with the job of reviewing all of the details of each death. Our citizen might make up our own sensible classifications: such as: ”Old Age complicated by Pneumonia initiated by a viral respiratory infection: maybe Covid-19 or influenza or the common cold”.
- Doctors (and here), Coroners and Medical Examiners are not immune to taking easy shortcuts. The official definitions for Covid-19 cases (in the essay) make it an easy choice for hurried doctors, and official guidance requires at least Covid-19’s mention on Death Certificates, under a vast array of normal circumstances during this pandemic. This is exacerbated by RT-PCR tests returning “positive” test results for very small amounts of viral RNA fragments in asymptomatic people.
# # # # #
Addendum:
There has erupted a flap concerning Genevieve Briand’s research at John Hopkins on U.S. Covid-19 Deaths: I supply these links on the controversy:
Covid-19 Deaths: A Look at U.S. Data
pdf file: https://drive.google.com/file/d/1iO0K75EZAF8dkNDkDmM3L4zNNY0X-Xw5/view
William Briggs: https://wmbriggs.com/post/33680/
Twitter Thread on the Paper: https://mobile.twitter.com/jhunewsletter/status/1332100136152035330
YouTube: https://www.youtube.com/watch?v=3TKJN61aflI
John Hopkins News-Letter retraction notice: https://www.jhunewsletter.com/article/2020/11/a-closer-look-at-u-s-deaths-due-to-covid-19
Author’s Comment:
I have mentioned previously that I come from a medical family and studied the prerequisites for medical school in university, before changing majors for personal reasons. Our home was filled with the joys of new life and the sorrow of babies’ and children’s deaths. My generation fought and died by the thousands in the misguided military intervention in Viet Nam – some of these were my cousins and high school and college friends.
We are all sad when lives are cut short.
Covid-19, the illness caused by the SARS-CoV-2 virus, is shortening the lives of thousands in the United States and around the world. One blessing is that it is mostly shortening the lives of those who have already had a life – as opposed to stealing the entire lives of our children and young people.
Public health organizations have valid reasons for counting “All Deaths Involving Covid-19” using their own internal definitions, which are suitable for epidemiological studies and research when combined with all the other information being collected to produce that statistic. That statistic, created with their surveillance and epidemiological definitions, is not suitable for release to the general public without a long and complicated explanation – releasing just the number, and labeling it as Covid-19 Deaths is a form of misinformation.
The media, politicians, health agencies and governments have utterly failed to effectively communicate the reality of Covid deaths, failed to illuminate the caveats and complexities of Cause of Death reporting and instead of have repeatedly just reported this “Big Number” in a usage that is seems to be intentionally misleading.
Opinions vary on this subject.
Address your comments to “Kip…” if speaking to me.
Thanks for reading.
# # # # #
One of the best articles I’ve read on the subject! Thanks WUWT! Now I have grave concerns about Biden’s new advisor.
https://www.google.com/amp/s/www.foxnews.com/politics/biden-coronavirus-adviser-emanuel-vaccine-distribution.amp
Here in the UK the number of deaths are given as “people who have died within 28 days of testing positive for corona virus” no matter what the actual cause of death.
I note that Euromomo is reporting in its latest weekly update that across the 26 European states involved there have been a total of 6,310 excess deaths. Wales. where I live and which recently came out of a further 2 week lockdown and is now about to face increased retrictions again from next Friday, is shown as having no excess deaths
Dave Andrews ==> Gads — that’s worse and “worser”! Died within 28 days of a positive test? Really? Can you give a link to the definition?
Kip, 28 days is the improvement from the previous definition of COVID deaths. The new method was introduced in the summer. Previously, anyone who had ever had a positive test, was counted as a COVID related death. It became widely known, and was losing public confidence, but authorities were still arguing against even this tightening of the definition. Of course, any mention on the death certificate is also included.
https://www.gov.uk/government/news/new-uk-wide-methodology-agreed-to-record-covid-19-deaths
Paul ==> Thanks for the link = incredible.
Come on, guys, PLEASE, just do the math!
In normal times, the UK records about 600,000 deaths per year. That’s about 50,000 deaths per month, which is 50K/66.65M = 0.075% of the nation’s population.
In other words, an average UK resident already has about a 0.075% chance of dying within the next month, without a Covid-19 diagnosis.
So, how does that compare to your chance of dying within the next month with a Covid-19 diagnosis?
Let’s calculate that. In fact, I’ll do two calculations: (1) over the entire epidemic, and (2) over a recent week, because the case fatality rate has been falling.
Over the entire epidemic, UK residents have had about a 4% chance of dying if they have a positive Covid-19 diagnosis (calculated as total deaths as of Nov. 30, 2020 divided by total cases as of seven days earlier, using the statistics from worldometer).
More recently, that death rate has decreased to about 1.9% (calculated by comparing deaths from Nov. 18 to Nov. 25 to confirmed new cases over the previous week).
About 88% of Covid-19 deaths occur within 28 days of diagnosis. So, multiplying by 0.88 yields the percentage of people who have a positive Covid diagnosis, who can be expected to die from Covid-19 within the next 28 days: 3.5% averaged over the entire epidemic, or 1.65% averaged over a single recent week.
Dividing 0.075% by 1.65% = 4.5%. In other words, if you have a positive Covid-19 diagnosis, you’re 22 times more likely to die from Covid-19 in the next month than to die from something else.
So, will everyone PLEASE stop repeating the nonsense that the number of Covid-19 deaths is greatly inflated by people dying “with Covid” who did not actually die “from Covid”?
Dave ==> have you looked at Genevieve Briand’s stuff? Watched he YouTube –worth the time if you are really interested in parsing the Covid-19 deaths question.
Turkeys in Turkey….
https://abcnews.go.com/Health/wireStory/turkeys-virus-figures-confirm-experts-worst-fears-74445462
ResourceGuy ==> There is the same problem we are seeing everywhere. Hospitalized cases are important and meaningful — asymptomatic, non-infectious cases are an epidemiological fantasy to stoke fear and panic.
From the recently censored John Hopkins paper.
https://andmagazine.com/talk/2020/11/28/how-many-people-are-really-dying-in-this-pandemic/
Kip, again this was a brilliant article. There were rumors about hospitals getting more money for Covid deaths. Liberal fact checkers said it was conspiracy theory. It isn’t.
https://www.google.com/amp/s/www.abc10.com/amp/article/news/verify/verify-do-hospitals-get-more-funding-by-marking-deaths-covid-19-related/103-36834bad-1113-4f67-8804-5d97e6593745
John ==> For our readers, ABS News found :
“Also, earlier this month, HHS announced a second round of federal relief for hospitals in high impact areas, totaling $10 billion.
Of that second-round money, HHS reported 63 California hospitals received $50,000 for each eligible coronavirus patient they admitted between Jan. 1 and June 10, 2020. That’s a combined total of more than $607 million.”
So, yes, certainly hospitals have had an incentive to add Cocid-19 to death certificates — and diagnoses– at least in the “conditions contributing to” section — each mention being worth 50 thousand dollars to the hospital….
To wit: THE QUESTIONS:
Do hospitals receive more funds if they say a death is related to COVID-19? And does this mean the number of coronavirus death are false or inflated?
THE ANSWER:
ABC10 can verify that hospitals do get reimbursed for coronavirus related care, which unfortunately includes deaths.
As for the the second part of our viewer’s question, a medicare spokesperson said it is unlikely.
“Claims with inaccurate diagnosis or DRG would be subject to recoupment and/or other potential civil or criminal charges for false claims.”
So far, it is unverified that hospitals are falsifying records for financial gain.
John ==> YES $50,000 per Covid case, including Covid death.
Death certificates are often garbage in/garbage out. For instance if you die in your sleep at age 105 we are required to say cause of death, so you put in cardiac arrest, yep the heart stopped. Then you are required to say why a cardiac arrest so you put down heart disease, etc. You are not allowed to die of old age at 105 in your sleep. Death certificates are helpful but very crude.
Flu usually spikes in Dec-march time, varying year to year and usually in one of these months we have marked difficulty getting patients to hospitals, often needing to go outside of our area so ICU’s being full in the winter is common. With social isolation occurring around the world we are seeing far fewer flu cases than usual. We may well have offsetting issues where we are seeing an increase in covid deaths and decrease in flu deaths. The efforts at social distancing etc. are going to be much more successful with a less infectious agent (flu).
This of course does not explain the decrease in other causes of mortality. I suspect some of this is related to how things are categorized but we have seen time and again that all cause mortality drops when hospitals close. Not going to hospitals reduces mortality in the short term but then there is the price months down the road when the patients start dying in higher numbers due to putting off necessary procedures and treatment. While hospitals have not closed, patients avoiding hospitals and physicians putting off elective treatments are effectively the same as partial closure.
I think we need to get through the entire winter and then revisit these numbers to have a full understanding.
An aside. In the winter you have an increase in viral illnesses. Patients are coming in testing positive for covid and a secondary virus such as a rhinovirus. It is possible that by slowing the spread of Covid in the summer, we will have caused increased winter mortality rather than minimizing deaths. Much remains unknown but I fear political correctness will prevent adequate evaluation.
Dr. Gossom ==> Thanks for your input.
Thank you for the insightful comments, Dr. Gossom.
Although I understand your reasoning about the effect if time-shifting cases from summer to winter, I very much doubt that, overall, “by slowing the spread of Covid in the summer, we will have caused increased winter mortality rather than minimizing deaths.” I am confident that the opposite is true, for several reasons:
1. Most obviously, because Covid-19 vaccinations are about to begin. A case delayed until he has been vaccinated (plus a few more weeks) is a case avoided completely.
2. Because treatment regimens have improved, contributing to a decrease in the case fatality rate. So a case delayed from early in the pandemic to late in the pandemic has a lower risk of dying.
3. As you pointed out, the same measures which have slowed the spread of Covid-19 have also reduced the number of flu cases, and presumably also the number of colds and other communicable diseases. That should also reduce the number of patients having simultaneous infections, with both Covid-19 and those other diseases.
“With social isolation occurring around the world we are seeing far fewer flu cases than usual.”
Maybe we are seeing many ordinary flu cases falsely called COVID cases, because there are financial incentives to do that. I don’t see any incentive to NOT blame COVID if there are any flu symptoms at all, or if pneumonia was present, whether there was a positive COVID test result or not. I’m not even sure we should call COVID infected people with no symptoms “sick”. Lots of people carry viruses in their body for most of their lives, such as herpes simplex. Are they considered “sick” most of the time when they have no cold sore outbreak?
“we have seen time and again that all cause mortality drops when hospitals close”.
The obvious solution to death is to close all the cemeteries.
Richard, ordinary flu cases are not falsely being called Covid cases.
Within hospitals, flu cases and Covid cases are, of course, distinguished by testing for flu and Covid, so there can be no confusion (except for a few hours, until the test results are in). Outside of hospitals, there are no financial incentives for identifying Covid cases.
Medical mistakes certainly happen, but speculation that government assistance to hospitals to help them withstand the financial hardships caused by the Covid pandemic is leading hospitals to falsely diagnose patients with Covid are baseless speculation.
It is unsurprising that social-distancing, mask-wearing, disinfecting often-contacted surfaces, etc., are reducing flu numbers cases. However, the Covid pandemic in the U.S. began near the end of the 2019-2020 flu season, and the 2020-2021 flu season has just begun. So it remains to be seen whether flu case counts will remain low through the winter flu season.
Epilogue:
Thanks to all the readers who have commented and added to the conversation. Lots of input from professionals on the front lines: Nurses, Doctors, Coroners etc.
I have just watch Genevieve Briand’s presentation at John Hopkins — the presentation that the nambies at the John Hopkins News-Letter supposedly “retracted” . Note: they only retracted their news article on Briand’s findings –since they didn’t ever publish the findings they cannot and did not retract Briand’s findings.
Briand speaks accented somewhat halting English (French I think…) though she has taught in several US universities. Her YouTube presentation is very good despite the language thing, which makes listening a bit of a chore. Very interesting and much along the lines of what I have written above — I recommend it to those who have the time and interest. She uses nothing but official CDC data — but her take on the data is spot on and surprising!
Thanks for reading.
Read more — Read widely — Read Critically
# # # # #
And never trust the government.
Particularly world gummint-
https://www.msn.com/en-au/news/other/only-a-one-in-17-billion-chance-hydroxychloroquine-doesn-t-work-medical-professor/ar-BB1bseNF
The most pertinent metric is simply: a rise of EXCESS DEATHS in 2020.
The CDC tracks such matters and finds that yes… there has been an unexpected high number of deaths this year compared to the previous fives years or so, adjusted for demographics.
Unless there’s another explanation, EXCESS DEATHS in 2020 can reasonably be attributed to COVID-19, whether directly or indirectly.
But isn’t that the problem? Compared to what base line-
https://www.statista.com/statistics/1124915/flu-deaths-number-us/
And being common or garden flu that affects the aged frail and immune compromised to often be categorised as some other cause? After all with annual flu shots and all the copious medications we like to think we’ve got the problem licked and who wants on their headstone- ‘Caught the flu and died’. Least of all the medicos who under the circumstances would prefer something a bit sexier on the death certificate. In that respect you don’t hear much at all about ‘caught a cold and died’ and does died of a cold figure in the death stats at all?
‘Caught the flu and died”
Not good enough for a headstone
Need more details:
He was 98 years old,
with one foot in
a puddle of oil, and
the other foot on
a banana peel,
while walking to the
COVID vaccine room
in his nursing home,
he fell down and died:
Cause of death: COVID-19
Kip,
Thank you for your work in preparing this article.
Monger ==> Thank you. It is interesting to me how others — non-writers — view the work of serious writers. Some seem to think that an essay like this represents just the time it would take them — the non-writer –to whip out a “comment” of the same length (and here are some here, essay length comments). The truth is that an essay like this one can take a month of research and data collection — a bit at a time — looking for this fact and that — finding real authoritative references — and then days of full-time writing and editing (only to still find the occasional typo or omitted word).
Of course, I also write “quickies” — something banged out in a single day and then edited the next.
I appreciate your appreciation!
Just as pertinent would be a comparison of total annual deaths. I can find on the web the US had 2,839,205 deaths in 2018 which was 25,702 deaths more than 2017. But I can not find any such data for 2019 to act as a further baseline. Can anyone tell me how many died in the US in 2019?
Basil ==> The CDC has two sources for All Deaths — which do not return the same number, though they are in the same ballpark. FluView data returns (this is a PROVISIONAL number — won’t be official for more than a year yet) of 2,845,793.
The same data set gives 2,831,836 for 2018.
Except COVID deaths are overstated.
An excess deaths estimate for 2020 will not verify the whether the “COVID deaths” numbers from the CDC are accurate. Many people seem to think excess deaths estimates prove the CDC “COVID death” numbers are accurate. I disagree.
All other 2020 flu deaths are understated — suspiciously low.
All deaths related to flu should be combined for an excess deaths analysis to avoid the likely bias toward calling any flu death (always a wild guess) a “COVID death.””
There are actually financial incentives to call all deaths with symptoms of flu “COVID deaths”.
There is a lot of guesswork to call any death a “flu death”, when there will almost always be other medical problems. So the total flu deaths is a questionable number to begin with. Most doctors thinj CDC overstates “flu deaths”. Asj your own doctor.
And then total US mortality can rise five percent just from random variations along with population growth and an aging population .
Even a 10% rise in one year — not likely but possible — could be mainly be a random variation.
COVID must lead to other causes of death rising in 2020 and 2021 too, such as suicides, homicides and people afraid of going to doctors and hospitals in 2020 — that’s wild guess too.
Look at https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm: the excess death rate is clearly not a random variation. The spike in January 2018 was due to a really bad flu season (estimated at 60,000 deaths): it is obvious that 2020 has excess deaths way beyond that.
The excess death rate at the national level matches up in temporal patterns with national COVID death estimates – https://www.worldometers.info/coronavirus/country/us/ (big hump in the first wave, medium hump in the 2nd wave, 3rd hump starting in October). Excess deaths are actually higher than the COVID deaths, indicating that the COVID deaths are an undercount.
Moreover, if you actually drill down state by state (click on the state name in worldometer, or use the drop-down menu in the CDC site), you can see that the temporal trend in excess deaths in each state track the COVID reported deaths. That’s just as true in lockdown states like New England as in mask-optional states like the Dakotas: that shows the excess deaths aren’t mainly a function of the lockdowns, but of the pandemic itself. (I’m not saying that are no incidental deaths due to panic, just that they aren’t needed to explain the giant spike in mortality: also, there are likely reduced deaths due to the lockdowns as well, due to decrease in other contagious diseases and in car accidents)
And the excess deaths can be a large percentage of normal deaths: North Dakota usually has 150 deaths a week in November, but this year has been having 250 deaths/week. That’s not a random fluctuation.
Can’t help but notice that Griff has failed to comment on this post after repeatedly spreading misinformation on US COVID mortality numbers on other posts. Typical!
Thank you for the most informative article this layperson has read since this began: not difficult to understand and with links to support. I also appreciate all the comments which allow me to see clarifying or disagreeing viewpoints. A few blogs I read include this feature, for good or for bad, which demonstrates that the author is willing to accept feedback (and comment on it, if desired). Have a blessed December and be safe.
Marc ==> And thank you for your kind words. Isn’t it interesting how many differing views there can be, even of the very same numbers — and even the very same words! (like a clear definition).
I have been a web professional since 1995 — and the thing that is good about the web is that one can communicate with so many people from different places and backgrounds. But it takes a dedicated site operator and dedicated moderators to keep a site like this going — the heroes are Anthony Watts and Charles and the other, unsung moderators. They do all the real work.
Ditto. Very well stated Marc B.
“Victoria has recorded its first COVID-related death in more than a month, after a woman aged in her 70s died from complications related to the disease.
The Department of Health and Human services (DHHS) said the woman was diagnosed with coronavirus in late July and was cleared as an active case in late September.
However, because she did not make a full recovery from the original infection, her death is considered COVID-19-related.”
https://www.msn.com/en-au/news/australia/victoria-records-first-coronavirus-death-in-more-than-a-month-after-woman-in-70s-caught-virus-in-july/ar-BB1bthZu
Yeah right you are there docs. Nothing to see here Coroner. Move along.
observa ==> Yes, they are counting, like in the U.S. — Covid-19 RELATED or INVOLVED deaths. Sometimes their logic seems like “deaths involving heart stopping”…..
Would have preferred an in-depth analysis of the differences in COVID attribution internationally. There is a panic driving effort to maintain rapt attention and it would be beneficial to know that the U.S. is not doing 10 times worse than the rest of the world. Everyone here saw the news going around yesterday that the U.S. is twice as negative as anywhere else in its news coverage?
On a related note, we are on track for COVID to be about 1/4 the U.S. per capita death rate of the 1918 virus. I can grieve the loss of a loved one in a car accident without banning cars.
Coach ==> It is difficult enough for this one old man to find and collate information on a single country that is fairly open with its data — an international comparison would take months…if possible at all.
There have been some comments indicating how other countries are actually defining Covid cases and Covid deaths — many are not following the WHO definitions.
UK? “people who have died within 28 days of testing positive for corona virus”.
Even before Genevieve Briand’s paper I had looked at the CDC data concerning all deaths. I saw that overall death increase was not statistically significant from previous years. That was odd. Then, I looked at various other causes of death. You would think that those numbers wouldn’t change or if they did, might actually increase. That’s not what’s happening. These common deaths are decreasing. Are they decreasing? Of course not. These deaths get folded in to the Covid count. That’s why total overall deaths have seen no statistically significant increase in death. They’re gaming the numbers. Why are they gaming the numbers? There are many reasons but one of the most prominent is to use as a hammer against Trump.
Joz ==> “Why” question are almost always impossible to answer.
As I say, they are counting what they say they are counting — but it is not what you or I might count given the same stack of Death Certificates.
Covid is carrying away a lot of older folks — it is a nasty nasty disease — worse than most of the recent influenzas — not as bad as the worst. Probably not worth destroying the national economy to slow its inevitable spread and death toll.
“That’s why total overall deaths have seen no statistically significant increase in death” People keep saying that, but there is a huge increase in total death rates. See https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm
Neiman Marcus,
That certainly says there are more deaths this year than for the last five. So what is Genevieve Briand talking about, and what is Kip Hansen talking about? Am I missing something here?
But I agree with Mr. Hansen, shutting down the economy and devastating the lives of tens of millions to extend the lives of people who are already into “extra innings,” as we say in baseball, questionable, and is it even working?
keep closing down the economy and soon there will be NO mom and pop stores left open. since small business employs most people, there will be a lot of people out of work/behind in payments/etc.
next, reiterate ad nauseum how bad a capitalist economic system (which we don’t have anyway) is to blame. repeat the blame game ad nauseum.
voila!! the final outcome is socialism for you and me, agree or be taken care of and thrown into the oven.
remember who did this when you and your children are hungry and powerless to change it.
Kip,
Is this the biggest news of this Century? They lied, almost all the deaths were going to happen anyway, Covid only kills those on their last legs, or as Rud put it, those with not much road left?
If there are no new deaths compared to last year, or only the 0.6% due to the annual increase in the population of the USA, we have destroyed a prosperous economy, put tens of millions out of work, shut down hundreds of thousands of businesses that were doing just fine, and all for what?
Unbelievable.
Mass hysteria.
So this statistic from Dr. Briand, heart disease deaths are down? Stroke deaths are down? Diabetes, cancer, Alzheimers, respiratory illnesses including the flu and pneumonia are all Down, But this new vicious disease is killing all those people previously dying from known causes?
The truth must come out. CDC needs to tell the truth, not protect the idiot Governors, Mayors, and Directors of the various Departments of Public Health whom have foisted this prevarication on the US of A. Did they do it to get rid of Trump?
Mr. Trump is still there, maybe he does not know what has happened.
The truth must come out. “Help us Obe-Kip, you are our only hope….”
And I do not know why my business partners turned off the website, the project is ongoing.
Michael ==> Many people are dying, many people always die. Covid-19 is carrying away many of my generation — and the one just preceding mine. It isn’t that people aren’t dying of Covid-19– it is that what this means is different for the CDC and WHO than it would be for us.
So,
The election is not over yet. Two huge questions: Can the rules of the elections be changed right before the election due to Covid?
And,
Can votes arriving after Election Day, from the mail-in ballots not requested by any voters, still be counted? Both questions must go to the Supreme Court, both completely un-precedented. I liked the old rules, you vote on Election Day or you did not vote. Some people are sick, so now you can mail in your ballot late? Makes no sense….