Guest Essay by Kip Hansen – 27 November 2020

There has been massive media attention on Covid-19 deaths – and there have been a lot of them. The CDC as of noon on 26 November 2020 was reporting that there have been 259,005 total Covid-19 deaths in the United States.
Yet anyone who reads widely is aware that there have been reports of a motorcycle accident victim being reported as a Covid death. There are many who correctly report that all people dying from or with Covid and even suspected of dying from-or-with Covid-19 are all being counted as certified reportable must-make-the-headlines Covid-19 Deaths.
[Note: This is a long and rather detailed explanation of what leads to the situation in which we find ourselves regarding Covid-19 Deaths reporting. Those who want a better understanding of the issue should continue reading. Readers with no or little interest can just accept this brief synopsis: “It’s Complicated” and move on to other posts. ]
Various experts, journalists, bloggers, and pundits tells us that “Covid Deaths” are being over-counted, mis-counted and even under-counted. Other pundits and media-reported experts desperately try to reassure us that Covid Death counts are correct and real – and that we should all stay concerned and follow all government mandates – which vary from “reasonable” to “obviously based on magical thinking” (closing bars and restaurants at 10 PM because that’s when the Corona Virus Zombies attack) — all this despite various governments having different and contradictory mandates (or even an absence of mandates) and the various States in the United States following differing rules and policies on Covid Deaths reporting. Those reporting “facts” like “US Covid-19 Deaths overestimated by 17 times” (based on this CDC comorbitity data) are sadly mistaken and misinform the general public, just adding to the general confusion on the subject.
Doctors, Coroners and Medical Examiners will calmly explain that “Cause of Death” is complicated and not simple. And they are right. Most of us think that when a person dies, it is obvious what killed him/her. But that is just not the case. In fact, everyone dies of a combination of ”heart stoppage” [cardiac arrest] and “cessation of breathing” which eventually leads to “brain death”. But these are not usually listed as the Cause of Death on a death certificate.
Covid Deaths are being counted and reported based on advice from the CDC, who has based its advice on advice from the Council of State and Territorial Epidemiologists (.pdf). More on what that means later.
The Primer: What is meant by Cause of Death?
When a person dies in a hospital or other setting, there is some doctor, coroner or medical examiner that fills out a death certificate – officially certifying that John/Jane Doe has died and reports the date, time, place, Social Security number and other personal details along with the circumstances and sequence of events that led to that death.
Here’s a CDC-annotated image of the Cause of Death portion of a typical death certificate:

We are interested here only in Parts I and II.
“Part I
This section on the death certificate is for reporting the sequence of conditions that led directly to death. The immediate cause of death, which is the disease or condition that directly preceded death and is not necessarily the underlying cause of death (UCOD), should be reported on line a. The conditions that led to the immediate cause of death should be reported in a logical sequence in terms of time and etiology below it.
The UCOD, which is “(a) the disease or injury which initiated the train of morbid events leading directly to death or (b) the circumstances of the accident or violence which produced the fatal injury” (7), should be reported on the lowest line used in Part I.”
[ source: CDC here – .pdf ]
Let’s look at a CDC example:
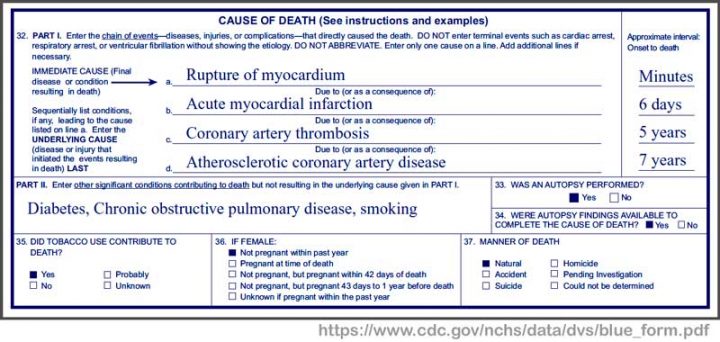
This patient had Coronary Artery Disease for seven years — which led to Coronary artery thrombosis from which the patient suffered for 5 years — which led to Acute myocardial infarction (heart attack) after which he survived for 6 days until — his heart ruptured resulting in death within minutes. Conditions contributing to his/her death were diabetes, COPD, and smoking. Each of these “significant conditions contributing to death, but not resulting in the underlying cause” are themselves known to cause a wide range of other serious conditions. For instance, smoking is believed to cause COPD and heart disease. Diabetes can cause cardiovascular diseases “including coronary artery disease with chest pain (angina), heart attack, stroke and narrowing of arteries (atherosclerosis).” Notice that there is a dedicated section “35” asking “Did tobacco use contribute to death?” For this patient, the doctor chose “Yes” – thus the CDC will count this death as one of the 480,000 annual tobacco deaths.
Let’s look at another example (from the same document):
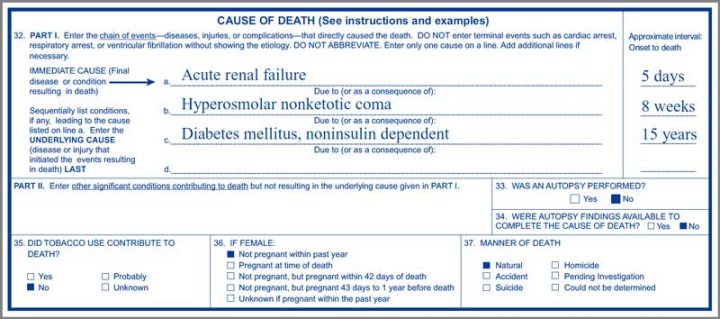
This person suffered from noninsulin dependent Diabetes mellitus, often called Type 2 Diabetes, for 15 years. As sometimes happens, this diabetes sufferer eventually went into a Hyperosmolar nonketotic coma in which she/he remained for 8 weeks before finally succumbing to Acute renal failure (kidney failure). The family of the patient would have told friends and neighbors that their loved one died of kidney failure. They may have mentioned this was probably the end-of-line result of his/her long-term diabetes. Type 2 Diabetes is known to cause the following conditions: Heart and blood vessel diseases, Nerve damage (neuropathy), Kidney damage (as in this patient), Eye damage, Slow healing, Hearing impairment, and even Alzheimer’s disease.
It is clear that this second patient died of acute kidney failure – “Acute kidney failure is most common in people who are already hospitalized, particularly in critically ill people who need intensive care” — and is not necessarily a direct result of diabetes – but assumed in this case as kidney damage can be caused by diabetes. The death certificate Part I sequence is reasonable and represents the doctor’s professional opinion.
“In certifying the cause of death, any disease, abnormality, injury, or poisoning, if believed to have adversely affected the decedent, should be reported. If the use of alcohol and/or other substance, a smoking history, or a recent pregnancy, injury, or surgery was believed to have contributed to death, then this condition should be reported. The conditions present at the time of death may be completely unrelated, arising independently of each other; or they may be causally related to each other, that is, one condition may lead to another which in turn leads to a third condition, and so forth. Death may also result from the combined effect of two or more conditions.”
Source CDC Medical Examiners’ and Coroners’ Handbook on Death Registration (.pdf)
So, you call the Cause of Death of these two patients. What was the Cause of Death of each? Did diabetes kill them both? The first patient via atherosclerosis which kicked off the sequence in Part I? The second from the diabetes induced coma or was the coma from simply caused by being in intensive care? Or was it the first patient’s life-long cigarette smoking causing the coronary artery disease? Or would you, as this doctor did, start the death sequence with his/her seven years of Atherosclerotic coronary artery disease? In each case, there are several sequences that would be reasonable and could have been correctly entered by the attending physician, a coroner, or later by a medical examiner.
The above are pretty common examples – long-term conditions which lead to the next condition that finally leads to death. We don’t see the personal information part of the Death Certificate so we don’t know the age of these patients. The age of the patient is often key to Cause of Death – but is not to be used as a cause itself.
“Common problems in death certification
The elderly decedent should have a clear and distinct etiological sequence for cause of death, if possible. Terms such as senescence, infirmity, old age, and advanced age have little value for public health or medical research. Age is recorded elsewhere on the certificate. When a number of conditions resulted in death, the physician should choose the single sequence that, in his or her opinion, best describes the process leading to death, and place any other pertinent conditions in Part II.” [ source: CDC my bolds – kh ]
And then this:
“For statistical and research purposes, it is important that the causes of death and, in particular, the underlying cause of death, be reported as specifically and as precisely as possible. Careful reporting results in statistics for both underlying and multiple causes of death (i.e., all conditions mentioned on a death certificate) reflecting the best medical opinion.
Every cause-of-death statement is coded and tabulated in the statistical offices according to the latest revision of the International Classification of Diseases. “
Source CDC Medical Examiners’ and Coroners’ Handbook on Death Registration (.pdf) – my bold — kh
There are over 69,000 ICD-10 diagnostic codes. Someone goes through every death certificate filed and translates the diseases and conditions the doctors, coroners and medical examiners enter in Parts I and II into ICD-10 codes (soon to be ICD-11 codes). There are so many codes that there are many online look-up tools and apps to help medical staff code up office visits and others to code up Cause of Death certificates. The first Death Certificate above might be coded: “ E08.01 Diabetes mellitus due to underlying condition with hyperosmolarity with coma” – which would cover Part I lines “c” and “b”. This diagnosis is billable. This app helpfully informs the staff if the ICD-10 code they select is “billable” – if not billable, we can safely suspect that office assistants coding office visits can search for a true but alternate diagnostic code that is billable. “All conditions mentioned on a death certificate” are translated to ICD-10 codes and eventually tabulated “for statistical and research purposes”. In our two sample Death Certificates, there are ten different diseases and conditions mentioned. Thus each of the ten condition codes eventually, at the CDC and WHO level, gets a little “tick-mark” – a plus one – added to the number of deaths involving that ICD-10 code.
Thus the huge number of deaths reported for which smoking is claimed to be the cause, as we see in this next quote from the CDC:
“Smoking is the leading cause of preventable death.Worldwide, tobacco use causes more than 7 million deaths per year. If the pattern of smoking all over the globe doesn’t change, more than 8 million people a year will die from diseases related to tobacco use by 2030.
Cigarette smoking is responsible for more than 480,000 deaths per year in the United States, including more than 41,000 deaths resulting from secondhand smoke exposure. This is about one in five deaths annually, or 1,300 deaths every day.”
[ source: CDC here ]
Most people simply accept those statements as fact, though they know of no one who put a cigarette in their mouth, lit up, and died as a direct result. Through many years of public health anti-smoking/anti-tobacco education we have been taught that smoking or otherwise using tobacco can lead to a long list of health problems, many of which cause or contribute to the eventual death of the smoker. In this case, a life-time of tobacco use is referred to, by public health officials, as a “cause” of death – though it probably would not be listed as a cause on a death certificate. Despite not being listed as a cause on the Death Certificate, the CDC and WHO unequivocally tells us that smoking is “the leading cause of preventable death”.
As in many complicated subjects, there are varying definitions in use for the same terms – in this case “cause of death”. There is the general everyday use – like “something that directly causes the death of a person, if it hadn’t happened, they wouldn’t have died”. So, a person gets lung cancer, probably or presumably because they had been a life-long smoker, and dies from the lung cancer. We know they died of lung cancer but accept that smoking led to that death. It is this definition that the WHO uses above. But it is not the official definition that is to be used on a Death Certificate as Cause of Death, which is in the quote far above, labelled Part I.
Those readers who watch any of the popular crime and police television series know that Cause of Death in trauma deaths is even more complicated — “homicide, accident or suicide?” — though those TV Medical Examiners are always portrayed as having almost paranormal insight – “blunt trauma to the head…but that’s not what killed him.”
One last quote from the handbook for medical examiners:
“Precision of knowledge required to complete death certificate items
The cause-of-death section in the medical examiner’s or coroner’s certification is always a medical opinion. This opinion is, of course, a synthesis of all information derived from both the investigation into the circumstances surrounding the death …. It represents the best effort of the medical examiner or coroner to reduce to a few words his or her entire synthesis of the cause of death.”
[ emphasis in the original – kh ]
Bottom Line: Cause of Death determination and reporting is complicated and highly dependent on the training and opinion of the person making the report.
# # # # #
Reporting of Covid-19 Deaths
Here’s the pivot point on Covid-19 Deaths:
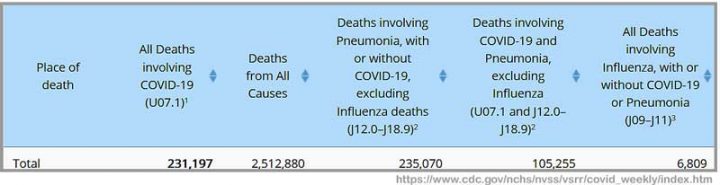
This is from the CDC’s weekly Covid report. See the Column 2 heading? It says “All Deaths Involving Covid-19 (U07.1)1”. The keyword is INVOLVING. To be perfectly clear, what is being reported by the CDC, as collected by the National Center for Health Statistics, are All (every one) Deaths (people dying) that Involved Covid-19. See the little footnote indicator “1”?
Footnote 1 says: “COVID-19 deaths are identified using a new ICD–10 code. When COVID-19 is reported as a cause of death – or when it is listed as a “probable” or “presumed” cause — the death is coded as U07.1. This can include cases with or without laboratory confirmation.”
Not just verified cases in which Covid-19 was the immediate cause of death. At least, to be even clearer, not necessarily what you, the average reader, would consider THE cause of death.
So, what exactly are they counting when the CDC and WHO report Covid-10 Covid-19 Deaths? The World Health Organization’s official guidelines are:
2. DEFINITION FOR DEATHS DUE TO COVID-19
A death due to COVID-19 is defined for surveillance purposes as a death resulting from a clinically compatible illness, in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID disease (e.g. trauma). ….
A- RECORDING COVID-19 ON THE MEDICAL CERTIFICATE OF CAUSE OF DEATH
COVID-19 should be recorded on the medical certificate of cause of death for ALL decedents where the disease caused, or is assumed to have caused, or contributed to death.
[ my emphasis – kh source: WHO here .pdf ]
Note that the Death Certificate — Cause of Death Part II is “Other significant conditions contributing to…”. So, there is where Covid-19 (ICD code U07.1) would be written for any death in which Covid wasn’t “caused, or is assumed to have caused” but only contributed to the death. If the decedent was a “Covid case” then he/she becomes a “Covid Death” if they die. Read on . . .
For the general public, who want to know “How many people are being killed by the SARS-CoV-2 Pandemic?”, this definition does not supply the answer to their question. The vagueness and breadth of these definitions is exacerbated, in this “possibly-too-broad” sense, by the definitions being used to define “What is a Covid-19 case?”. We see that the WHO definition of a Covid death includes “a probable or confirmedCOVID-19 case”.
So, how do WHO and the CDC define or advise doctors how to define/determine a Covid-19 case?
Clinical Criteria
At least two of the following symptoms: fever (measured or subjective), chills, rigors, myalgia, headache, sore throat, new olfactory and taste disorder(s)
OR
At least one of the following symptoms: cough, shortness of breath, or difficulty breathing
OR
Severe respiratory illness with at least one of the following:
Clinical or radiographic evidence of pneumonia, OR
Acute respiratory distress syndrome (ARDS).
AND
No alternative more likely diagnosis
[ source: CDC here ]
So, by this definition, I could at this very moment be declared to be a Covid-19 case. I have muscle pain (myalgia) and a headache — two symptoms – — and yesterday, I had a cough — and, if I have reported to the ER and doctors are both rushed and spooked by the pandemic, there might be “no alternative more likely diagnosis”, in their minds at least. (Of course, I have these symptoms for reasons well known to me and my personal physician but this might not save me in the ER.) Especially if they also ask me a bunch of epidemiological questions:
“Epidemiologic Linkage
One or more of the following exposures in the 14 days before onset of symptoms:
Close contact** with a confirmed or probable case of COVID-19 disease;
OR
Close contact** with a person with:
clinically compatible illness
AND
linkage to a confirmed case of COVID-19 disease.
Travel to or residence in an area with sustained, ongoing community transmission of SARS-CoV-2.
Member of a risk cohort as defined by public health authorities during an outbreak.
**Close contact is defined as being within 6 feet for at least a period of 10 minutes to 30 minutes or more depending upon the exposure. In healthcare settings, this may be defined as exposures of greater than a few minutes or more. Data are insufficient to precisely define the duration of exposure that constitutes prolonged exposure and thus a close contact.”
[ source: see previous quote ]
So, if I were in the Emergency Room, the ER doctor might ask me these questions: Do you know anyone who isn’t feeling well? Have you been in close contact with them for more than 10 minutes? Have you attended any meeting with more than 10 people in the last 14 days? Have you been to church or a party? Have you visited a restaurant or a bar? Any YES epidemiologically qualifies me as a Covid case. More questions: Do you wear a face mask whenever you are out of your own home? in your car? in WalMart? at the park? while mountain biking? Any NO qualifies me as a Covid case epidemiologically.
You can see how easy it is to be classified as a Covid-19 case. And they haven’t even tested me yet. (Read the link to see why even testing wouldn’t save me.) They would report me as a Covid case even if I tested negative – I might not be positive “yet”.
And while I describe my pending Covid-19 Case classification jokingly, it is a very real scenario. And, heaven forbid, were I to die of almost anything (except obvious trauma) in the next 14 days, I would become another Covid-19 Death statistic.
As most of us know by now, advanced age is a key factor in the vast majority of Covid-19 deaths:
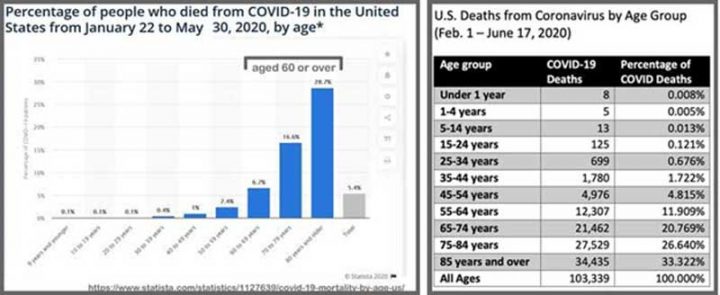
Eighty percent (80%) of Covid-19 deaths are of those 65 years of age of or older – and a full one-third of the deaths occur in those over 85 years. If you are an adult today, then you were born between 1925 and 2000. At your birth, you could expect to live (life expectancy at birth) between 58 to 72 years, depending on your birth year. Those who are dying at 85 or older had a life expectancy at birth of less than 61 years. [My life expectancy at birth was about 66 years – so I have beaten the odds and hope to continue to do so for many years more.]
If this does not seem significant to you, I’ll repeat the CDC quote on reporting cause of death for the elderly – those 65 year of age or older.
“Common problems in death certification: The elderly decedent should have a clear and distinct etiological sequence for cause of death, if possible. Terms such as senescence, infirmity, old age, and advanced age have little value for public health or medical research. Age is recorded elsewhere on the certificate. When a number of conditions resulted in death, the physician should choose the single sequence that, in his or her opinion, best describes the process leading to death, and place any other pertinent conditions in Part II.” [ source: CDC my bolds – kh ]
For the elderly, the aged, the older citizen, which comprise the majority (80%) of Covid-19 deaths, any illness or condition that leads to breathing problems is prone to being classified as a Covid case, and thus a Covid-19 death in “a clinically compatible illness, in a probable or confirmed COVID-19 case”.
Bottom Lines:
- It is complicated.
- Make no mistake, there are lots of people dying deaths that involve confirmed, assumed, or suspected Covid-19.
- Somewhere between “Most” and “Almost All” of those deaths involved other conditions that were already killing the patients – sometimes slowly, sometimes rapidly.
- The official health organizations have their own reasons for what they are counting and they are counting exactly what they say they are counting – but it is not what you or I would expect them to count. They are counting, as the CDC does, “All Deaths Involving Covid-19”.
- The Covid-19 Death statistics represent the counts of the WHO, the CDC and other National and State public health agencies. The general public often mistakenly thinks those counts mean deaths in which Covid-19 was the immediate cause of death – deaths in which the person was killed by Covid-19. That is not the case – it is far more complicated than that.
- The common citizen would have grave doubts about including each and every one of those dead people in the count of “Deaths Caused by Covid-19” if they were tasked with the job of reviewing all of the details of each death. Our citizen might make up our own sensible classifications: such as: ”Old Age complicated by Pneumonia initiated by a viral respiratory infection: maybe Covid-19 or influenza or the common cold”.
- Doctors (and here), Coroners and Medical Examiners are not immune to taking easy shortcuts. The official definitions for Covid-19 cases (in the essay) make it an easy choice for hurried doctors, and official guidance requires at least Covid-19’s mention on Death Certificates, under a vast array of normal circumstances during this pandemic. This is exacerbated by RT-PCR tests returning “positive” test results for very small amounts of viral RNA fragments in asymptomatic people.
# # # # #
Addendum:
There has erupted a flap concerning Genevieve Briand’s research at John Hopkins on U.S. Covid-19 Deaths: I supply these links on the controversy:
Covid-19 Deaths: A Look at U.S. Data
pdf file: https://drive.google.com/file/d/1iO0K75EZAF8dkNDkDmM3L4zNNY0X-Xw5/view
William Briggs: https://wmbriggs.com/post/33680/
Twitter Thread on the Paper: https://mobile.twitter.com/jhunewsletter/status/1332100136152035330
YouTube: https://www.youtube.com/watch?v=3TKJN61aflI
John Hopkins News-Letter retraction notice: https://www.jhunewsletter.com/article/2020/11/a-closer-look-at-u-s-deaths-due-to-covid-19
Author’s Comment:
I have mentioned previously that I come from a medical family and studied the prerequisites for medical school in university, before changing majors for personal reasons. Our home was filled with the joys of new life and the sorrow of babies’ and children’s deaths. My generation fought and died by the thousands in the misguided military intervention in Viet Nam – some of these were my cousins and high school and college friends.
We are all sad when lives are cut short.
Covid-19, the illness caused by the SARS-CoV-2 virus, is shortening the lives of thousands in the United States and around the world. One blessing is that it is mostly shortening the lives of those who have already had a life – as opposed to stealing the entire lives of our children and young people.
Public health organizations have valid reasons for counting “All Deaths Involving Covid-19” using their own internal definitions, which are suitable for epidemiological studies and research when combined with all the other information being collected to produce that statistic. That statistic, created with their surveillance and epidemiological definitions, is not suitable for release to the general public without a long and complicated explanation – releasing just the number, and labeling it as Covid-19 Deaths is a form of misinformation.
The media, politicians, health agencies and governments have utterly failed to effectively communicate the reality of Covid deaths, failed to illuminate the caveats and complexities of Cause of Death reporting and instead of have repeatedly just reported this “Big Number” in a usage that is seems to be intentionally misleading.
Opinions vary on this subject.
Address your comments to “Kip…” if speaking to me.
Thanks for reading.
# # # # #
Kind of like while the Corona deaths went up, all other causes of death dropped by a comparable amount. 45 minute presentation, but it’s worth the watch:
https://youtu.be/3TKJN61aflI
That’d be a lot more interesting if it were actually true.
Look at euromomo.eu , an official european web site set up about 10y ago exactly for the purpose of detecting and monitoring pandemics.
https://euromomo.eu/graphs-and-maps/
We see that there was a high but short peak in march/april and a tiny bump of a “second wave”, which is now basically over with only the over 65 group yet to fall back fully to the time of year average.
France is still assigning about 600 deaths per day to COVID against an average daily death toll of 1600-1800 per day from all causes. Scroll down to the bottom and you will see that “excess deaths” z-score is very close to zero now, ie totally average daily fatalities.
If people are dying of covid-19, it just replacing deaths by other causes. THERE IS NO HEALTH CRISIS IN FRANCE.
There is a political crisis, with Macron directing the entire operation from with meetings of a “national defense committee” for which there are no recorded minutes and the everything other than the fact a meeting is taking place is classed “secret defence” : national security top secret, so even those present are forbidden from divulging anything. In any case most are generals and police commanders. This is NOT about health issues.
“consulted October 15th, this might look slightly different now”
Well this vid was posted Nov 13th and it does look different. They do not even provide a link the description. Lamez.
There is an open source project which accumulates covid and recently added excess mortality data.
https://github.com/owid/covid-19-data/blob/master/public/data/excess_mortality/excess_mortality.csv
Sadly the totals seem to come in rather late, so excess deaths is a few weeks behind. I think they wait for verified data whereas other sources use non validated figures for recent weeks.
I have not plotted US data from there yet.
OK here is the plot. Note third peak is not yet showing.
https://climategrog.wordpress.com/excess_us_2010-2020/
Worth seeing this in the context of the 8000 people who die every day at this time of year.
This was posted at the JHU site where they removed the Briand analysis.
https://ourworldindata.org/grapher/excess-mortality-raw-death-count?tab=chart&stackMode=absolute®ion=World
I read the words “it’s complicated” in the third paragraph and the writer went on to make sure it really was complicated.
very old white guy ==> I didn’t make it very complicated — it has always been very complicated.
Government bureaucrats are involved.
They make everything complicated.
Results in their job security.
Excellent learning. Thank you.
Can someone clarify if a “confirmed case” is the same as a positive test?
Also, the CDC is saying that the actual number of infections could be 8 to 10 times higher.
Isn’t this a good thing that 10s of millions more have been infected, but not required hospitalization?
Thanks WUWT ==> Only in Covid-19 reporting — you can be considered a case with a cough and fever. That would be confirmed if you tested positive for Covid-19 on a 40 CT RT-PCR test — even though you really are suffering from the common cold.
No , you don’t even need the cough.
What the media is laughably calling “cases” of COVID-19 is nothing more than a ( possibly false-) positive PCR test.
Medically you are not a “case” of anything if you present no symptoms: you are NOT ILL, so you can’t be a “case”.
Greg ==> You are correct. Influenza reporting by the CDC is of SYMPTOMATIC ILLNESSES — not “cases” by testing. Persons without illness, without symptoms, are, as you correctly point out, not cases. see: https://www.cdc.gov/flu/about/burden/2018-2019.html
Gee, I’m not a medical professional, but I’ve been saying this all along.
Donna ==> and you were right all along. That’s why, in my Where Are All The Sick People? survey, I asked specifically about people sick enough to stay home from work, school, or normal activities — what we would consider being sick.
If the actual number of infections is 8 to 10 times higher, then North Dakota is at herd immunity, or will be soon, since a full ten percent of its residents have now been reported to have had Covid-19.
While I doubt that the 8 to 10 figure is accurate, even if it’s 5 to 6 then they should be rapidly approaching herd immunity. One good test of that is whether they endure a Thanksgiving/Christmas surge, or if the recent peaking of cases in early November holds and cases continue downward from here on.
Other states with highest percentage of confirmed cases: S. Dakota, Iowa, and Wisconsin.
Thanks WUWT ==> Sorry, worse than that….not only didn’t they require hospitalization, they probably didn’t even know they were sick — well, strictly speaking, they weren’t sick at all as they had no symptoms,
When they started testing everyone on a positive, symptomatic patient’s contact tree, more of the asymptomatic/minimally symptomatic were uncovered. Otherwise none of those had any reason to get tested unless they were in a group required to be tested for one reason or another (think food service).
Richard ==> Listen to the Mike Yeadon YouTube — https://www.youtube.com/watch?v=8bX-wFVBP94
Kip,
One of the odd observations about COVID-19 is the degree to which its mortality statistics mimic normal age related mortality statistics. I know for certain that influenza pandemics do not do the same as influenza kills a disproportionate share of the very young. The 1918-1919 pandemic killed an unusual number of adults in mid life, and so forth.
A way to explain this odd observation easily is to consider that some number of deaths belonging to “normal mortality” are classified as COVID-19. It is, in a sense, a case of circular logic. Does one get a distinctly different age distribution of deaths confining one that small subset of person dying strictly of COVID-19?
“…confining one’s attention to that …”
There is a paper by Professor Spiegelhalter (U. Cambridge) that showed the age profile of of UK Covid deaths follows almost exactly the age profile of normal deaths, i.e. Covid “cases” died when they were expected to die.
“ Use of “normal” risk to improve understanding of dangers of covid-19”
I wish I could give a direct link but there is a Youtube video that covers an in depth study explaining why the 1918-21 Flu pandemic killed so many young, otherwise healthy, Americans. Basically they had missed being exposed as young children to an earlier far less lethal strain that would have provided a better immune response. There were many other areas of the world where the death toll was as high or higher because the population was “virgin territory” as it circled the globe in 3 distinct waves; Melanesia and interior China especially.
>>
. . . I come from a medial family . . . .
<<
Don’t we all–or wish we did.
Did you really mean “a medical family?”
Jim
Jim ==> I love detail readers — even my editor (a past professional) missed that one! Thanks.
Kip, I didn’t want to be a jerk, picking nits, but the reference to COVID-10 did catch my eye.
I greatly appreciate the time and effort that you clearly put into your article. If I may also say so, I appreciate the robust comments and the many other informative articles and stories on WUWT. Thanks, too, to Anthony and Charles for making the site a great place to visit!
badEnglish
bad ==> well done, sir or madam — you get the Astute Reader award. I had been tying ICD-10 and Covid-19 so many times my fingers must have combined hem!
Hanseen
If BoldEnglish gets an Astute Reader award, can the rest of us get “Participation Awards” ?
Richard ==> In keeping with modern educational theory, all the children get an award, “just to be fair”.
Thanks Kip. I don’t think there is an easy way to tease this apart. Even comparing excess death rates is fraught.
For example, in Australia influenza deaths are down because of the lockdowns. Road deaths this year are also down, nobody was allowed to drive far for many months.
Now people have much more freedom to move, will road deaths in Australia surge, because everyone has forgotten how to drive?
I think the statistic to watch is ICU beds. Covid survival with ICU intervention available is good. If ICU beds run out, the prognosis for people who need ICU care but can’t get a bed is not so good. Of course having said that, I can’t find good stats on how many people who contract Covid progress to needing ICU care.
Eric ==> As far as I’ve seen. the stats for surviving the ICU with Covid are pretty bad — of course, they only put you in the ICU if you are dying…..
ICU beds and ICU nursing is very very expensive for the hospitals, and they (like hotels) profit from keeping “occupancy” above a certain profit base.
Kip, I’ve seen claims survival is now around 60%, so if ICU beds run out you may see a doubling of the death rate amongst people who should have been admitted to ICU but can not find a bed. But its anyone’s guess what impact if any this would have on the “Covid deaths” statistics.
Eric ==> Even New York City, at the height of its “murdering of old folks in nursing homes”, did not run our of ICU beds and ventilators. The hospital ship sent by the Federal Government and the emergency hospital built in Javitts Center went unused.
It is only little Podunk hospitals that are at any danger of running out of ICU beds, but only because they have so few to begin with — the same situation occurs EVERY year in which we have a bad flu season in the U.S. These smaller hospitals usually end their excess really sick patients to bigger regional hospitals. My local hospital does the same — sends the to Albany Medical Center – which has as almost as many employees as my town has residents.
I read that some hospitals have plenty of ICU beds, but not enough staff for them. That gets reported by MSM, though, as “running out of ICU beds”. Maybe they should hire back the people they laid-off during the shutdown.
And hospitals are at 100% capacity in the Midwest. So says the MSM. But this Midwest hospital executive says his are always at 100% this time of year (click on image for full comment).
https://twitter.com/AlexBerenson/status/1332719838251380736
I know it was a simple oops and not a Freudian slip, and yet ” These smaller hospitals usually end their excess really sick patients to bigger regional hospitals.” Ending the patients was a tad ….
…mouse ==> Thanks — love a careful reader.
“they only put you in the ICU if you are dying”
Not true at all.
A few years ago, a member of my family was in ICU for several days. She was quite ill, and probably would have died without the intensive care. But she was eventually moved from the ICU to a standard hospital room and was discharged sometime later.
I spent a night in the ICU once because I fainted from GI pain (probable vasovagal response). The most miserable night of my life. Between the auto blood pressure cuff inflating every 15 minutes and all the noise from the other patients, I didn’t get a wink of sleep. But I was nowhere near death.
last yr and prior flu seasons we had the RAH and Vic hospitals saying they were running short of beds due to huge influx of flu patiets, funny how no ones mentioning it now?
hell of a lot of oldies would have died as that strain the new VicB was savage and we had H1N1 doing the round too
and vax wasnt working, people who had regular jabs were still keeling over
oz ==> In a mood of prescience, I wrote about The Flu in the spring of 2019. https://wattsupwiththat.com/2019/02/22/100-years-later-the-flu/
The Briand study refutes all those worries by showing that the proportion of deaths by age is unchanged. We believe that covid kills the elderly at a vastly higher rate, so we should observe a proportionate increase in deaths among the elderly; and the increase should be even more apparent if fewer young are dying from other causes (e.g. car accidents) while they are safe at home. Briand did not find this. So, which is it? Covid is a merciless killer? or, you were about to die anyway?
Michael ==> I have not done a deep dive in Briand’s study — saw it after the essay was finished and about to be published. I threw in the links for those interested.
In a study from two hospitals from New Jersey, they found that 89% of deaths attributed to COVID were patients who had already, previously posted Do-Not-Resuscitate ofders. This is a strong corroboration of Briand. I found that info on the BLAZE.
Michael,
Nice name. The criticisms of Briand point out that 300,000 more people will die this year than last year. But the USA has 2 million more people than last year. I think she may be into something. She is a superb statistician.
I work on a Covid unit. I have a cough. I have a headache. I have GI symptoms. Therefore I have Covid. No, I have bronchitis (chronic), allergies (leading to the bronchitis) and IBS. And I tested negative for Covid, twice. So what do I do? I lie on the form every shift to say I have none of these symptoms or I would never work. This is what I deal with. I can’t wait for retirement.
tired ==> Thanks for sharing the Nurses’ Viewpoint. Appreciate it and all you do.
Thanks. I do apologize for the whining though! On a more helpful note, I’m working on a PCU where we care for Covid patients that require PCU level of care. We commonly have patients with ESRD, end stage COPD, end stage (fill in the blank) who are transitioning to palliative or hospice care. The only difference is that as they are Covid + they languish on our unit. With very few exceptions Covid does not play a significant role in the patients’ deaths They were actively dying in any case. But many are absolutely being labeled as straight up Covid deaths. While this isn’t some gut feeling, as I have seen the death certificates, I have nothing to substantiate my statement.
I don’t wish to down play the actual severity of the disease. I just despise anyone who plays politics with any disease. I thought the circus surrounding HIV was bad…that wasn’t even a warm up for this disaster
Tired Old Nurse ==> Good input from someone on the front lines — ground truthing much of what I have said in this essay.
No one wants to downplay the loss of life — but many are terrified by the loss of jobs, the loss of common freedoms, and the destruction of much of the economy through edicts that do no good, only harm.
Thanks for your service and doing what needs to be done
I get sniffles due to allergies so I too have to lie occasionally
I have asthma, hay fever and allergies but spend a few hours per week in a sensitive work situation where if I get sick lots of people could be exposed.
My view, if I can keep the symptoms suppressed with my usual medications, nothing unusual is happening. If my symptoms seem unusually bad, if my usual medications seem to be struggling to suppress my symptoms, I have a Covid test. So far I’ve had two tests since the start of the year, both negative.
I’ve had 4 for various reasons since March all negative
But I was doing my usual amount of travel before that and I’m convinced I had it
In December I had a 18 hour bout of vomiting then I had a week of blah in mid January
But no way to tell
Depending on the test, it might have a false positive/false negative issues. Too much testing will get you one of these. I rely, instead, on oximeter readings.
Thus, only if something is driving my health down will I take a test. Meanwhile, I maintain aviation D (and Zinc supplements) to maintain very high blood levels aiming at 50 ng/d levels, ie, well above a high of 30.
This is the single best way to maintain your health. Dr John Campbell has over a dozen YT vids on Vitamin D and the best studies showing that it’s the best, simplest, and cheapest independent preventative (as well as treatment).
“I lie on the form every shift to say I have none of these symptoms or I would never work.”
Something similar happened to me at my gym (before covid). When I listed all of my conditions (well treated by standard medication), they wouldn’t let me join, so I got a new form and told them I had no illnesses. Sometimes I get really tired of all the nannies about.
A very good, detailed explanation of the subject
And if I try to post a link to this piece the thought police will come down hard on me, here in canada.
“Thoughtful” is not really allowed.
I was banned from the CBC because I posted the link to the worldometer corona virus page for Sweden
I did this to counter another commenter who said Sweden blew it and the numbers prove it
But this page shows Sweden had ~1500 cases per day in the first wave and peaked at over 100 deaths per day
In October they shot past 5000 “cases” per day, now averaging 7500 a day, 5x increase
But deaths peaked at mid 30s per day last week and now are down in single digits, so 1/10 the daily deaths of first wave
Elementary math gives Death/cases in the second wave 1/50th of first wave
Isn’t that at least somewhat significant?
Pat ==> See the links at the end re Genevieve Briand’s research on the topic.
Kip, I see nothing in those links regarding Sweden?
I’m interested because they are basically the only western. Developed country that followed a different path.
Various online trolls are trying to state Sweden now says they screwed up but that is just panicking politicians.
I have not read such a thing from the architect Tegnall, who does regret not protecting old folk homes better but he seems to still believe the path.
And really, Sweden has always been the model progressive state, if someone said there was proof they deliberately under protected the old folks in order to thin that part of the herd I would easily find a way to believe it.
But for now I’m ok with “mistake”.
Pat, I’ll differ that Sweden is a model for the world.
Their rate of death per million is close to the Netherlands, which has used harsher control measures and controlled more distancing.
But Sweden is unique with a low population density, an engrained culture dedicated to physical distancing, and two houses per household. In short, the opposite of the Dutch.
Thus, Sweden isn’t a model that’s adaptable or easily translatable elsewhere. It’s too unique.
Density is not as relevant as some may think :
– Most of the worst clusters developped where the density is not very high, in Italy (near Bergamo) and in the east of France for example.
The density distribution may be somewhat more relevant :
– for example, in Sweden, 87% of the population lives in 1.5% of the country.
Another point of interest is the vulnerable population distribution in connected networks with paths (travelling doctors, patients) and nodes (hospitals, nursing homes, family houses) :
– in most of european countries a low density of such networks, means just that their paths are longer (the nodes are roughly similar except in countries with very high GDP per capita as in Norway which can afford many little nursing home structures for example).
Another important piece of information is how many vulnerable people live in a country when an epidemic strikes :
– there were many (relative to the total population) in Sweden due to a low or negative excess mortality in the years before the SRAS-COV2 pandemic.
From this point of view (and others) here is a publication in which a comparison is made between Sweden and other Nordic countries :
https://youtu.be/J3vDsKEOIQI?t=345
Here is a publication that makes an analysis of different parameters (among them, population, lockdowns, temperature, GDP, etc.) with respect to SRAS-COV2 mortality :
https://www.frontiersin.org/articles/10.3389/fpubh.2020.604339/full
How do you fit two houses in a household?
Sweden has a higher % of urban population than the UK.
Sweden Sweden Sweden
I’m sick of hearing about Sweden
They had partial lockdowns — high schols and most colleges
They banned gatherings of 50 (or maybe it was 500) people or more
They did NOT treat COVID like an ordinary seasonal influenza.
Reasons to NOT use Sweden as an example of good policies:
– The pandemic is still in progress — conclusions could change.
– Some nations will have good or bad results by chance, which can never be explained.
– Nations that received the most incoming airplane flights fro China (such as Italy), and later incoming flights from Italy, were likely to suffer the most. How many Chinese people flew to very cold Sweden in late 2019 and early 2020 — I’d guess not many.
– Sweden is in the top 20 for deaths per 1000,000 population
– Their GDP went down a lot in the first half of 2020
– There are dozens of other nations with better results
What is the fascination with Sweden?
That social distance was voluntary? I like that, but people avoided certain businesses that were open, but social distancing was a problem, and the businesses suffered for about three months, just like there WERE mandatory lock downs.
After about three months, Then the Swedish decided the worst was over and voluntarily began returning to those businesses. I hope they were right. Their typical refusal to wear masks did not help. But probably would not have made much of a difference in the hospitalization and death numbers.
This diagram from CEBM, UK shows a radial polt of all deaths through the weeks in the year for recent years.
You can clearly see the Covid 19 first and second waves, with no need for cause of death, just the recorded value.
Ian.
I only look at the Scottish data which shows the exact same hump April/May. there is no doubt in my mind that a virus was partly responsible for killing the aged with other severe diseases. However, nearly half of Scottish deaths were in Care Homes and started after ‘lockdown’. I have no way of knowing and neither does the government, if these were Covid or just general lack of care after lockdown. The horror stories of care homes throughout the world are very distressing.
As for a ‘second wave’. It is hardly surprising that death rates have gone up over October. There has been a huge increase in the number of people who have died at home and that may be a result of lockdowns.
Interesting that there is so much difference in excess deaths and covid-19 deaths, especially as lockdown was expected to cut road deaths. Seems like an awful lot of excess deaths caused by lockdown? Untreated cancer, heart attacks, suicides, etc.
https://fingertips.phe.org.uk/static-reports/mortality-surveillance/excess-mortality-in-england-latest.html#region
but the second national lockdown seems to have escaped that effect – at least initially.
“what leads to the situation in which we find ourselves regarding Covid-19 Deaths reporting”
You get the behaviour you reward. If you are paying me $13k for each “positive” well I’m cranking my PCR to 45 and KA CHING baby.
Except that’s another of the Covid myths. https://virologydownunder.com/the-false-positive-pcr-problem-is-not-a-problem/
Adam Gallon ==> Tricky, isn’t it. Your guy says “they are not false positives”. Another guy, writing reported in the otherwise “all-in-for-Covid-panic” NY Times, reports US doctors saying exactly the opposite — testing is way to sensitive for reporting positives worth acting upon.
I wrote about this issue earlier: https://wattsupwiththat.com/2020/09/07/covid-19-testing-1000-times-too-sensitive/
Kip, an outstanding guest post. I was contemplating something similar, but had not yet completed the requisite research thanks to Thanksgiving disruptions. Could not have risen to your level of excellence in any event. I’m just a JD/MBA who happened to helm a topical antimicrobial company licensed from P&G. No medical aptitude whatsoever.
To boil down my two cents worth of ‘findings’ on this topic:
1. The ‘died with’ or ‘died of’ COVID-19 is a very real ongoing controversy, with strong provable federal financial incentives for reporting ‘of’ instead of ‘with’.
2. Subproof. The average US age of death is 84. So is that for COVID-19–‘with’.
3. This core issue gets more material as we (US) have demonstrably (CDC data) reduced excess deaths by about 85% despite the recent surge in cases. We know more how to treat this disease than we did in March—dexamethasone steroid to halt cytokine storm, monoclonal antibodies like Regeneron or Lilly, anticoagulants to stop the microthromboses evident upon autopsy,…
4. The lockdown and mask stuff just do NOT work well. Dunno exactly why, only that causes enormous economic damage and does not prevent COVID-19 much. Many comparison US jurisdictions now for statistical validity. My two cents on those issues:
Lockdowns don’t work because people won’t fully ‘obey’, and the virus likes ‘cheaters’.
Masks don’t work well for the reasons explained in the newish Danish study.
The new SCOTUS ruling prohibiting edicted NY religious lockdowns and Gov. Cuomo’s arrogant ‘nonscience’ response typify the whole mess.
Rud ==> Thanks for the compliment. You are right on your points…..the Real World® problem is that the SARS-CoV-2 virus doesn’t recognize the lockdown and doesn’t stay sheltered-in-place — it does what every other virus does — it runs rampant through human populations until it is slowed/stopped by vaccinations or herd immunity. Then it pops up each and every cold/flu (and now /Covid) season.
Thank you Kip and Rud – good comments.
In Alberta we have a population of ~4 million, and ~500 have died from the Covid-19 flu according to provincial government stats. Average age of Covid-attributed deaths was ~82, and only about 3% of those had no co-morbidities – not to be cruel, but these old folks were running out of road – and the lockdown ensured that they died alone- – horrible!
In Alberta, total deaths from opioid overdoses doubled from ~500 to ~1000 during the lockdown, equal to about twice Covid-19 total deaths – I say ~500 of those opioid deaths were CAUSED by the lockdown – average age of opioid-od deaths was ~32
Opioid deaths also doubled in the Province of BC during the lockdown – and probably many other places too.
So just examining these two causes of death (Covid-19 and opioid od’s), the lockdown caused [~50years*500lives =} 25,000 years-of-life-lost here in Alberta. That does not count other lock-down-caused deaths including other suicides (reportedly way up) the destruction of our economy and small businesses and the huge unemployment of typically-young service-sector employees.
The Covid-19 lockdown can be characterized as a misguided war on the young and the poor – in a failed attempt to save the very elderly and infirm, our government impoverished and killed the young.
This is such a damned annoying and depressing fiasco. Eight months ago I published here in wattsup on 21March that this Covid-19 lockdown was a huge error. I hate being right about these things – it’s a no-win.
The more probable reality is that the full-Gulag lockdown for Covid-19 was not just an error, it was a WHO-led scam, sponsored by the Chinese Communist Party, the leftist press and the Marxist-Dems, to defeat Trump in the November 2020 election.
Post Script:
USA Covid-19 death stats are hugely overstated. Take Alberta Covid-19 deaths for our 4 million people and scale up to the total USA population – and only about 30,000 USA deaths can be attributed to Covid-19 – far less than the 244,000 Covid-deaths quoted in bogus USA stats. But then, USA deaths attributed to Covid-19 include motorcycle crashes, heart attacks, cancers, drive-by-shootings, parachuting “bounces”, etc.
THE GOOD NEWS – NOBODY HAS DIED FROM “OLD AGE” SINCE MARCH 2020.
The claim that a large percentage of the reported Covid-19 deaths are misattributed is provably false.
Here’s a CDC page with U.S. death statistics between Feb. 1 and Nov. 21. (I also loaded the data into this spreadsheet.)
Look at these numbers:
C = COVID-19 Deaths: 240,213
P = Pneumonia Deaths: 242,296
F = Influenza Deaths: 6,829
P ∩ C = Pneumonia + COVID-19 Deaths: 109,504
P ∪ C ∪ F = Pneumonia, Influenza, or COVID-19 Deaths: 378,800
where:
∩ means set intersection (“and”)
∪ means set union (“or”)
Pneumonia is a common way for Covid-19 patients to die, but there were 242,296 – 109,504 = 132,792 pneumonia deaths not attributed to Covid-19. In fact, only about 45% of pneumonia deaths were attributed to Covid-19.
So don’t let anyone tell you that deaths due to respiratory problems like pneumonia are being widely misattributed to Covid-19. That’s obviously untrue.
Hospitals are routinely testing patients for Covid, and if they test negative then their death is not attributed to Covid, even when they had symptoms like pneumonia, which are often caused by Covid.
The reported of known Covid-19 deaths is clearly an undercount, because of deaths outside of hospitals in people who were never tested for Covid, and are not attributed to it. That’s probably a small percentage of Covid-19 deaths, now, but it is clear that in the early days of the pandemic the undercount was large.
“3. This core issue gets more material as we (US) have demonstrably (CDC data) reduced excess deaths by about 85% despite the recent surge in cases. ”
We’re no longer telling people to avoid the hospital unless you have Covid. People are actually going in when they might have had a heart attack, etc. That was probably the biggest “non-covid” factor in excess deaths.
Dear Kip
Excellent dissection of a very muddy patient.
I have been following John E Cullen on Jason Goodman’s Crowd Source the Truth and enjoyed the work of Jamie on the Climatism Blog. You have brought their work together.
Cullen is claiming a Nobel Prize for his work on drawing attention to the eradication of the Flu in week 11 of the CDC Data. You may be able to join him in claiming this prize.
Yours in Cognitive Dissonance
Broadie
Broadie ==> Dissection is almost always messy — not like on TV….
Very good explanation of how the death count is calculated. Shows the bad math that is used to keep the lockdowns active. I remember the number that the CDC said was caused by C-19 ~ 9200? No way near the 200000 + the MSM pushes. Never mind the PCR testing fraud. Just ask Portugal. Wonder how many cases caused by the cold virus show up in the PCR running over 35-40 passes.
RT ==> RT-PCR testing would reveal almost all currently-being-circulated viruses at those levels. But they have to be individually tested for.
It would be interesting to know exactly how a positive PCR test evolved into being a case.
I first noticed it about 30 years ago when they equated testing positive for HIV as having AIDS. They used to call it HIV disease. Lots of people tested positive for HIV who never got sick. But that started the virus = disease paradigm.
“Just ask Portugal”?
Excellent post as usual, Kip. The pandemic is at least as much a media and political phenomenon as it is a medical one. All I want right now from our media in Canada is a simple affirmation that it is very rare for an otherwise healthy Canadian to die of COVID-19. I despise the technically accurate but deliberately vague way they say that “younger people are at greater risk of serious harms than older people.” And of course, the second you mention that almost all of the dead are elderly, on the way to making the point that the measures to limit its spread are disproportionate to the harms of disease, they accuse you of dismissing the value of the lives of the elderly.
I once read that medical students say (as a joke) that the cause of death for many people is TMB. Which means, Too Many Birthdays. They also call the geriatric ward the Departure Lounge. So young doctors-in-training quickly come to terms with the fact that human beings are mortal, and the condition of mortality is exacerbated by time and age. So much of the pandemic reporting just ignores this fact, and actively demonizes anyone who might point it out.
Ian ==> Quite so….
Ian
TMB is a good one, had not heard that one
I came up with my own a few years ago when I turned 50
I tell people the doctor told me I have O L D, that it’s terminal and is no cure
Some burst out laughing immediately, others show instant concern and ask if I want to sit, is there any cure, what can they do to help, I stare at them until they get it
Some never get it
Oops. I screwed up in my post above. I meant to say that media gets around the stark age-specificity of the mortality of COVID-19 by saying that “younger people are at less risk of serious harms than older people.” It’s the quick, stealthy admission that is also a dismissal that is so offensive. It would be as if they said, “younger people are at less risk of heart disease than older people.”
Now our national broadcaster in Canada is reporting that a ten year-old has died of COVID-19. No details. That’s the story. That there are no additional details seems awfully suspicious, because you just know that a healthy ten year-old didn’t just catch the virus and die. It would have had to have been more complicated than that. Of course the point of the story is to frighten into silence anybody who dares to say that healthy young people have little to fear from COVID.
And then of course there is undefined term “case.” No explanation of what constitutes a case is ever given. Just big scary numbers designed to frighten rather than inform.
Why didn’t Donald Trump die? What has become of Melania Trump? Is she fighting for her life on a ventilator? Why aren’t recoveries from COVID-19 discussed? This is manipulation, pure and simple, and I’m fed up with it.
CTV tonight said the boy under 10 had underlying medical problems. Seems that CBC neglected to mention that
Hello, Ed. Yeah, they neglected to mention it. That’s how activist media types lie: they report facts that are technically accurate, and then leave out other facts that undermine the effect they want to create. It was at least a month into the pandemic in Canada before the CBC admitted that the median age of the COVID dead was 84. Even now, American news media reporting on the death tolls of COVID just don’t bother discussing the ages of the dead, as if this were a trivial point that no serious person need consider.
CDC tracks national health & death statistics and their C-19 web site has a plethora of tables displaying age, gender, location of death, comorbidities, by states and counties, etc.
One such table tallies “C-19 deaths” and “deaths from ALL causes” side by side.
There are around 2.8 million US deaths from ALL causes every year. On average that’s 7,670 per day or 53,800 per week. This is the “normal” load for the medical system.
To gauge the impact that C-19 deaths had compared to the normal national deaths they are plotted together on a common graphic along with the percentage of C-19/ALL deaths.
The first wave peaked the week of 4/18/20 with 17,088 deaths or 22.3% of ALL deaths.
The second ripple peaked the week of 8/1/20 with 8,227 deaths or 12.9% of ALL deaths.
The third ripple peaked the week of 11/7/20 with 6,175 deaths or 11.6% of ALL deaths.
Cases don’t count, they are a function of testing which has become a total can of worms.
Deaths count.
From other tables:
Globally the US, India, Brazil and France together have more C-19 deaths than the ENTIRE rest of the world. (WHO)
Nationally NYC, TX, CA, FL, NJ, NY, IL, and PA together have more C-19 deaths than the ENTIRE rest of the country.
In Colorado, Denver, Adams, Arapahoe and El Paso counties together have more C-19 deaths than the ENTIRE rest of the state.
85% of US C-19 cases are among those under 65.
80% of US C-19 deaths are among those over 65.
24% of US C-19 deaths occurred in elder care, nursing, hospice.
Half of the 250,000 deaths occurred before 6/30, 20% of them in NYC alone.
Hard to comprehend how Covid-19 qualifies as a wide-spread, highly contagious, lethal pandemic.
More like a scam-demic big lie foisted on the public by opportunistic liberals and the fake news MSM.
Graphic located here:
https://www.linkedin.com/posts/nicholas-schroeder-55934820_publichealth-covid19-lyingmedia-activity-6738099757417422848-vtUb
Nick Schroeder ==> The SARS-CoV-2 virus and the disease it causes are serious, widespread, and are killing and/or accelerating the deaths of a lot of old people, both in the U.S. and around the world. No way around that.
The other issues are contentious — including the exact numbers, the magnitude, and the details….not to mention the many idiotic mandates claimed to be “for our own good”.
“Hard to comprehend how Covid-19 qualifies as a wide-spread, highly contagious, lethal pandemic.”
Easy Nick, you change the definition of “pandemic” in 2008 to remove the requirement for excess mortality. After that they can call almost anything a “pandemic”. How convenient is that?
Another aspect to this is the fact that the age group of people that die from COVID almost all get flu vaccines. So in previous years, they were at least partially protected and most of them did not die from the flu. The other health issues took their lives.
If there were no flu vaccines, the incidence of elderly people dying from the flu in the past would have been up astronomically.
Of course the COVID vaccine will cause the death rate to plummet by the greatest amount in the elderly, just like they are now protected from the flu.
Mike Maguire ==> As you already know, flu vaccines are not very effective compared to, say, measles vaccine or polio vaccine. A specific Covid-19 vaccine will be a life saver for sure, as long as the SARS-CoV-2 virus doesn’t mutate to the SARS-CoV-3 virus…..
“A specific Covid-19 vaccine will be a life saver for sure, as long as the SARS-CoV-2 virus doesn’t mutate to the SARS-CoV-3 virus…..”
Then, I suppose we develop another vaccine and have 2 COVID vaccines.
Here are the latest US COVID numbers with an interpretation. Scroll down to the last page at the link for the latest data/comments:
https://www.marketforum.com/forum/topic/61206/
Fauci got the flu according to him late last year. He said the flu coupled with all the speaking engagements led to a growth on his throat that needed to be removed. This is why you don’t hear much from him until lately.
Does it seem odd that the preeminent infectious disease doctor who has access to the latest flu data and flu vaccines got the flu? What hope do the rest of us plebes have if he can’t even avoid the flu?
Like many things today Covid-19 has been politicized. Once that happens truth becomes subjective.
Especially when politicized by antifa democrats, barbarism under the guise of moral superiority.
WHO has a question and answer web page on the differences between COVID and influenza. In spite of all the focus on COVID the web page was last updated. Here is the link https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/coronavirus-disease-covid-19-similarities-and-differences-with-influenza as seen today Nov. 28,2020. It is a long discussion and as far as mortality comparison, I am pasting the discussion from that web page verbatim:
“Mortality for COVID-19 appears higher than for influenza, especially seasonal influenza. While the true mortality of COVID-19 will take some time to fully understand, the data we have so far indicate that the crude mortality ratio (the number of reported deaths divided by the reported cases) is between 3-4%, the infection mortality rate (the number of reported deaths divided by the number of infections) will be lower. For seasonal influenza, mortality is usually well below 0.1%. However, mortality is to a large extent determined by access to and quality of health care. ”
On the other hand, worldometers reports that there are currently some 17.9 million active cases of which 105,000 are active or around .55 per cent but they report this as 0.6 per cent. With survival rate of more than 60 per cent of the critical cases, this will bring the deaths to around 0.2 per cent or very close to those of common influenza.
The biggest problem with COVID 19 decision making is the strong focus on the infection rates. When COVID first showed up, there were lots of mistakes such as exposing the elderly and those with chronic diseases. Yet, the focus is still on the infection rates rather than on reducing the death rate further. On the other hand , people are scared — really scared they willing to surrender basic freedom such as freedom to associates and move around. Unpopular politicians are getting stratospheric approval ratings for instituting draconian measures curtailing basic freedom especially in developing countries were levels basic personal health is very low.
Kip, great post! As a resident many years ago I did a number of autopsies. The causes of death could be interpreted many ways. I did several on smokers who died of lung cancer, one I remember who gave up smoking ~5 years before dying of a metastases to his brain. Is that a cancer death or a smoking death or both. I remember a young auto accident victim who was on the ward for several weeks. She died of overwhelming infection in fact I found Candida growing on her heart valves.
So in my reports re gross findings and histopathologic I noted everything. As a resident however I did not fill out death certificates. So it is complicated as you noted.
Mad Mac ==> Thanks — good to hear from a medical professional. Good heavens, YES, it is complicated!
Rather than a covid death, they should refer to it as an “impaired immune system” death.
Here is a very good explanation.
https://www.jhunewsletter.com/article/2020/11/a-closer-look-at-u-s-deaths-due-to-covid-19
brain ==> Yes, see the Addendum at the end of the essay.
Excess deaths in the US between February and early October were about 300 000 higher than usual. So if COVID isn’t killing people then something else is which is a much scarier idea.
Izaak Walton ==> I think you are missing the correct data — people are dying, lots of them, the point of this essay is the question of what is being provided by the press and CDC etc about that.
I intentionally gave links to the recent work of Genevieve Briand at the end of the essay, just before the Author’s Comment.
And did you read the retraction that you also linked to? It clearly states that Dr. Briand’s claim
“is incorrect and does not take into account the spike in raw death count from all causes compared to previous years. According to the CDC, there have been almost 300,000 excess deaths due to COVID-19.” The CDC’s webpage stating that is at:
https://www.cdc.gov/mmwr/volumes/69/wr/mm6942e2.htm
Causes of death are misleading as you mentioned but excess deaths are harder to argue with.
Approximately 2.8 million die in the US each year. The number actually varies depending on the source (the UN has different numbers, not sure how that works). Regardless of the cause is the extra 200k deaths significant enough rationale for the measures taken as there is no telling how much different the number of deaths would have been with no lock down? My answer is no. People die every day, they will continue to die every day. It’s my job to provide care to ill people, I value life, but we have to be realistic about what we can do to mitigate the effects of the disease vs the economic/societal drubbing we are inflicting upon ourselves.
You state that you value life but by how much? The standard value of a life for insurance purposes in the US is around $10 million dollars and without lockdowns you would expect more than a million deaths in the USA giving a cost of COVID-19 of over 10 trillion dollars. Lockdowns are cheap in comparison.
I’m looking at a a CDC page that gives deaths by month in 2017. At the end of November there were 2,599,000 deaths. This year at the end of November the CDC shows 2,579,548 deaths from all causes.
Where are those extra 300,000 deaths?
LINKS please to the data you’re referencing.
posa ==> CDC Data on All Cause Deaths is scattered and somewhat difficult. One source is the ongoing weekly report at this link :
https://www.cdc.gov/flu/weekly/index.htm#S2 — under the chart of P I and C deaths is a link to View Chart Data — this downloads a csv file which you can open in Excel or an Excel clone. Once open, Column G is “All Deaths” by month. It is trivial to add up the weeks to get the year-end total . For instance =SUM(G15:G67) give the total for 2014 of 2,664,285.
That’s the same number as ‘all deaths involving covid.’ They are counting every death ‘involving covid’ as an excess death, even though there is no similar spike in numbers of deaths from all causes, compared to previous years.
In other words, they are lying through double-speak.
That’s true as far as it goes. Right now it looks like excess deaths are running about 10% above normal. link
Recently, we’ve had 200,000 cases per day in America but we haven’t had a concomitant increase in excess deaths. So, it’s not like the Wuflu is like the plague or anything like that.
On the other hand, I’m not taking chances. I also take a dim view of the folks who think it’s reasonable to have their big ethnic weddings and the particular religious community near me who think it’s their God given right to do whatever, get infected in large numbers, and cause the rest of us to risk a lockdown.
Grrr. I think I’ll go spend some quality time with the heavy bag.
CommieBlob
That so-called CDC study is computer modeling nonsense.
The number of “COVID 19 deaths” is a CDC wild guess
The number of “non-COVID 19 flu deaths” is a CDC wild guess
The extremely CDC low wild guess for “non-COVID flu deaths”
strongly suggests CDC’s “COVID 19 deaths” are over stated.
There is no such thing as “normal” excess deaths.
With US deaths of about 2.8 million per year, just random variations from year to year could make that number go up one percent, or down one percent, in the next year.
One percent of 2.8 million is 280,000 deaths.
There may be 280,000 COVID 19 deaths in 2020.
If the total US deaths are up +280,000 in 2020 versus 2019, we can’t be sure that +280,000 was from the 280,000 COVID 19 deaths — +280,000 could just be a random variation from 2019 unrelated to COVID 19.
So we learn almost nothing from an excess death “study” when the COVID 19 deaths are only about one percent of total annual deaths. There may have been excess deaths in April 2020 and May 2020, but for the whole year of 2020 I doubt if any excess deaths study will be meaningful.
Richard Greene
perfesser of everything
I am not a real doctor but do
wear a stethoscope in singles bars
280,000 is 10% of 2.8M, not 1%. 10% excess mortality is significant. It is not the apocalypse but something to take seriously.
JoeRickShaw
My argument does not change even if the 1% percentage I wrote was wrong.
I’m glad someone here knows math !
The number of COVID deaths, which I guessed as 280,000 for 2020, is too small for use of an excess deaths analysis for the year 2020.
That type of analysis might work for a specific month, such as April 2020.
Total deaths vary from year to year. There is a rising trend from the growing population and the aging US population.
A change of up to +/- ten percent from year to year is possible.
With or without COVID deaths.
(Sorry I wrote +/- one percent in my prior comment).
10 percent would be an unusually large year to year random variation, but is possible.
Let’s say we have a “CDC claimed” 280.000 COVID deaths in 2020.
COVID has to be assumed as a cause of death, of course.
That’s based on guessing, since COVID alone is not killing people.
The 280,000 is probably overstated because the CDC guessed non-COVID flu deaths
seem ridiculously low for 2020.
280,000 “COVID deaths” is too small to be sure you will see +280,000 “excess deaths” in 2020 versus 2019.
+280,000 could be a large, but random, year to year variation.
Other causes of death in 2020 may have gone up, such as suicides and homicides — both related to COVID, but not officially COVID deaths..
2020 and future year deaths may rise from COVID-fearing people avoiding doctors and hospitals in 2020, and probably 2020 too.
So there are indirect effects on the death rate from COVID too.
But the original question is whether or not to believe the CDC wild guessed number of people who “died” from COVID in 2020.
I say the excess deaths estimates are NOT going to answer that question for 2020.
Especially if you combine ALL CDC wild guessed flu-related deaths in 2020 rather than just to focus on those (probably overstated) 2020 deaths the CDC attributed to COVID.
Read more carefully.
I am a senior now and my main concern along with a number of my friends is not the cause of death. If I go it really does not matter how any more. Our MAIN concern is PREVENTING needless deaths of seniors and those who may have other ailments. There are two things we can do to prevent deaths; 1) Proper diagnosis and good medical treatment and 2) Ensure we are as healthy as possible which would include supplements that we may be deficient in (more later).
I at this time do not have any significant ailments and I still play ball in the summer. With respect to prevention and improving our health the “medical experts” in Canada (I did not check other countries so will leave them out) appear on TV and in other media DAILY to report the number of cases and deaths and then go on with social distancing, washing and masks and say NOTHING about health and prevention. So I have essentially TUNED OUT to the broadcasts.
A friend whose son is a doctor in this field and I have been following Covid since it first appeared. I have read all the posts about it on WUWT and they are miles ahead of what I have seen on our local media. So I can say that we have likely read more than many GP’s about the subject. One of the items that has come up is Vitamin D deficiency and there were posts about this. Many seniors that died are confined indoors and do not get Vitamin D from the sun and colored people absorb up to about 35 % less. Some surveys showed a SIGNIFICANT Vitamin D deficiency in the deceased.
Now it just gets worse with respect to medical treatment.
All you hear in the inept media like CNN and CBC in Canada is that over 250,000 have died and it is Trump’s fault.
Readers may recall when President Trump noted the doctors that had success with Hydroxychloroquine and a combination with Azithromycin and Zinc. Readers may also recall the noise from CNN, Democrats and certain doctors in the USA which I believe included Fauci. So instead of saying, let’s check this out and working together, they continued denigrating Trump. So we hear CNN accusing Trump of lying, but has anyone counted the lies told by CNN?
So the result of this has been that the medical authorities in the USA limited the use of HCQ in the treatment of Covid. We must note that HCQ has been used safely for malaria and other illnesses for 80 years. Then with limited trials they approved Remdesivir which the WMO has recently said has no value. Of course the drug companies like it because it costs 100 times more than HCQ.
So this anit-Trump syndrome has spread to Canada. There are some trials going on but they may be designed to fail if they are with stand alone HCQ. The successful procedures generally involved HCQ in combination AND it must be given early in the sickness.
I have also been told that doctors in Canada have been told NOT to prescribe HCQ, a safe drug in use for 80 years.
We have written to health departments and to media about this and essentially get no replies or some negative ones from anti-Trump journalists.
Now there are two websites and in each of them there are studies and peer-reviewed studies approaching 200 that show the efficacy of HCQ and Vitamin D.
So below is part of a letter that I have sent to media and medical personnel:
I note that there are a number of Covid related articles in the Sun papers today, Sunday, Nov 22, 2020.
However, as I will relate, they are all missing the boat with respect to treatment. I am a senior and a friend and I have been following this situation since January, when it was considered racist to cut flights from China.
As my mother is older than I am, her health is also of concern. You may recall that in April, the MB government announced some cuts to senior care and we had to fight to have those reinstated.
A few doctors interviewed in Canada about Hydroxychloroquine have generally avoided the topic and the only comments have been that it has not shown to be good. Some of the “studies” in Canada are the main problem. They are essentially designed to fail. A friend and I have been doing a lot of reading and researching on this since last winter.
As we see it the whole problem started when President Trump quoted a top doctor in France who had success in treating patients with a combination of HCQ and Azithromycin and Zinc. In order to be effective this must be given early. After the Trump Tweet the media, Democrats and Fauci denigrated Trump and the health bureaucracy in the USA limited the use of HCQ.
If they would have worked together instead, the problem would have been significantly less. But they politicized it. Instead the Corrupt CNN and others chose to try and make Trump look bad and have killed over half the 250,000 people with their actions.
This syndrome has spilled over into Canada in my view as at least one doctor said (he,she) could be fired if they prescribe HCQ.
I have written to doctors and health departments about this and got no response. The other item I have written about is Vitamin D. Sadly, the response here was to tell me that too much Vitamin D can be bad for you. So are the 10 people who re dying daily in Manitoba dying from excess Vitamin D. It has been shown in some locations that most of the elderly who have died are Vitamin D deficient. This is also shown in the two sites I am going to quote.
Donna Laframboise (Toronto) is about the only journalist who has written about HCQ. She quotes an essay which describes the situation:
https://nofrakkingconsensus.com/2020/08/24/hydroxychloroquine-the-judgment-of-history/
Hydroxychloroquine & the Judgment of History
How a safe, well-understood malaria drug was demonized as a COVID-19 treatment. Because a politician said good things about it.
Norman Doidge persuasively argues that history will judge many people in Hydroxychloroquine: A Morality Tale,
Here are the two web sites which now have over 100 studies which show the efficacy of HCQ as well as Vitamin D:
https://c19study.com/
https://hcqmeta.com/
I would like these to be quoted for the public to see what they are being deprived of. In one of those sites there is a chart that shows that the countries which are using HCQ properly have lower death rates.
Will you as journalists quote these sites and ask doctors about them?
In an interview on TV, Dr. Bogoch (Toronto) said there are no studies which show benefit of Vitamin D.
Then we have the hypocrite, Dr. Sanjay Gupta on CNN who will say nothing about HCQ. I suppose if he told the truth they would release him.
Gerald Machnee ==> I will eventually write about the HCQ debacle. But not until the pandemic is past.
Thanks.
However, some of us in Canada are upset because seniors in care homes are dying and as far as we know they are not getting much for treatment. They are actually using Remdesivir because the CDC Okayed it even though WHO says it doe not do much good.
Gerald MacKnee sez:
“I am a senior now and my main concern along with a number of my friends is not the cause of death. If I go it really does not matter how any more.”
Your mind is good
Your comment is great
You’re not going anywhere !
I added 5000 IU Vitamin D to my diet in March 2020 on top of the 2000 to 3000IU already in my multiple vitamin and Calcium supplements that I have been taking for over 50 years. So far I have not had COVID. Although I now have six toes on each foot and need new shoes.
The controversy over HCQ is from the same ridiculous people who gave us the 2 million dead in the US wild guess computer game estimates and those dreaded lock downs.
You seem to have more than enough wisdom to agree with my favorite quote:
“Politics is the art
of looking for trouble,
finding it everywhere,
diagnosing it incorrectly,
and applying the
wrong remedies.”
Groucho Marx
This is funny. Climate scientist states in their typical, presumptuous manner that virtually all doctors and scientists agree that we need another lockdown; runs silly poll, gets owned.
https://twitter.com/GeoRebekah/status/1329909018152808453
“As you already know, flu vaccines are not very effective compared to, say, measles vaccine or polio vaccine.”
Yes, they need to be administered every year………..which is what we do and don’t protect us from all strains of the flu.
At 65 years old, I got my first flu shot. I’ve had the flu 1 time the past 25 years and consider myself low risk.
However, after looking at the stats and seeing how vulnerable the elderly are, decided to take advantage of science that makes it an even LOWER risk.
Great article…….thanks for contributing.
I. Am 81 years old I have never had a cold or flu but a year ago I suffered from bronchitis, (ok now) at 81 I think that the world has gone crazy Did they ban sex with HIV,/AIDS?
Overall comment.
The pandemic is still in progress so no “conclusions” are possible yet.
Perhaps one in 1,000 COVID infections leads to death.
Why focus on 1 of 1,000 ?
What about the other 999 of 1,000 ?
And what about the health problems resulting from unemployment and being isolated from others ?
Avoiding doctors and hospitals, alcohol abuse, drug abuse, depression, wife beating, child beating, mother-in-law beating, suicides, and even worse !
It seems like the deaths of mainly elderly people, probably all with other medical problems, is only the tip of the COVID iceberg.and
Are there any perfectly healthy people dying from COVID, or does it only contribute to the death of a person who has other medical problems?
I say COVID only contributes.
The other medical problems may not be known, but they exist. Perfectly healthy people are not among the 1 of 1,000 who get COVID infected and die. ” Flu deaths” is a CDC guessing game. The fact that guessed deaths from other flu strains are so low in 2020 suggests the guessed deaths from COVID are over stated.
If you consider EVERYONE who gets infected, why focus on the 1 of 1,000 who die, mainly elderly, and ignore the 600 of 1,000 with normal flu symptoms or severe flu symptoms, that survive. They add up to more pain and suffering in my opinion.
I was originally thinking the 400 of 1,000 COVID infected with mild or no symptoms were good news … consider a friends daughter, who only lost her senses of smell and taste … many months later she still has not recovered her sense of smell, which affects the sense of taste. There may be long term symptoms even for those COVID victims who were never sick enough to check into a hospital.
Some interesting COVID charts with data split by country on my climate science blog:
http://elonionbloggle.blogspot.com/2020/11/covid-19-data-charts-if-youre-not-tired.html
Richard ==> Like in many things, time will tell.
Richard wrote, “Perhaps one in 1,000 COVID infections leads to death.”
Who told you that? It’s not true.
That’s about right for seasonal influenza. But Covid is much more deadly.
So far, the USA has had 272,254 known Covid deaths, and 8,041,239 known Covid recoveries.
So, of known, resolved Covid cases, (272,254 / (8,041,239 + 272,254)) = 3.3% ended in death.
The number of deaths is an undercount, but the number of recovered cases is a much worse undercount. The true number of recovered cases could easily be twice that. So the average death rate, to date, might be as little as half that: 1.6%.
What’s more, that’s an average, over the full duration of the epidemic. The death rate has been declining, as the medical community gains experience with the disease, and as better treatments become available. So you should expect the death rate for recent cases to be lower.
Another way to estimate the death rate, just for recent cases, is by comparing the average daily death rate (an average of 1659/day, calculated over one week, Nov 17-24) to the average daily number of new known cases (161,014/day calculated over the previous week, Nov 10-17). 1659/161014 = 1.03%.
So the fatality rate is definitely falling, but it’s still about 1% of detected cases, rather than the 0.1% you estimated.
Even if half of all cases are undetected (doubling the denominator), that still makes the fatality rate over 0.5%.
Less than 70 y/o with no underlying health conditions, survival rate is 99.9% or greater.
icisil wrote, “Less than 70 y/o with no underlying health conditions, survival rate is 99.9% or greater.”
Where did you hear that claim?
If you think about it, there are some clear problems with it.
First of all, how many 69 year-olds do you know who have “no underlying health conditions?” That’s unusual! Almost all 69 year-olds have some “underlying health conditions.” So claiming that 69 year-olds with no underlying health conditions are unlikely to die from Covid is pretty meaningless. You might as well say that very few unicorns die of Covid.
In fact, most Americans have one or more “underlying health condition” which puts them at increased risk from Covid-19. My guess is that roughly 3/4 of Americans have one or more known risk factors: overweight, age >60yrs, diabetes, COPD, asthma, or other pulmonary disease, kidney or heart disease, etc. (In fact, roughly 2/3 of Americans are said to be overweight.)
It is certainly true that the Covid-19 infection fatality rate is much lower than average for young, healthy people. However, most people are not young and healthy, and the fact that Covid-19 is most deadly to people with other health issues is completely unsurprising, because that is true of most other diseases, too.
With the “no underlying health conditions” caveat, the claim is nearly meaningless, because most Americans have underlying health conditions.
Without the “no underlying health conditions” caveat, the claim would be clearly false. To see that, let’s look at some numbers.
Let’s start out by examining the statistics for the 50-64 age cohort.
According to this CDC page, between Feb. 1 and Nov. 21 Covid-19 claimed the lives of 37,430 Americans aged 50-64. (That’s the first row of this spreadsheet.)
If the Covid-19 survival rate were ≥99.9% for that age cohort, it would mean that 999× that many Americans in that age range had survived Covid-19. That would mean ≥37,392,570 recoveries, from just that age cohort.
But, according to worldometers, there’ve only been 8,222,879 known Covid-19 recoveries, in total, from the entire U.S. population.
It is quite possible that there’ve been as many undiagnosed recoveries as known recoveries, but doubling that still gives us only 16.5 million recoveries.
Do you see the problem?
Plus, that 50-64 age cohort is only about 19% of the U.S. population. (According to this page, there are 62.92 million 50-64 year-olds in America, which is about 19% of the U.S. population.) So, assuming their Covid infection rate is not wildly different from other Americans’ infection rate, even if half of the Covid recoveries have been overlooked, there still must have been only about 3 million recoveries in that age cohort, not 37 million.
Obviously, for the 50-64 age cohort, the fatality rate must be more than ten times that claimed 0.1% (i.e., over 1%).
Let’s check a younger age cohort. For example, the 45-54 age cohort has recorded 12,371 Covid-19 deaths so far, from a population of 40.88 million (about 13.6% of the total U.S. population). If their IFR were really only 0.1%, that would mean there were 999 × 12,371 = 12,358,629 Covid-19 recoveries, from just that age cohort, which is still obviously impossible.
I’ll leave it as an exercise for the reader to keep trying younger age cohorts until you find the age at which a 99.9% survival rate is possible.
Dave Burpin
Complete nonsense.
The death rate never reached one percent even in April 2020 when the ventilators were killing ICU patients and no one without COVID symptoms could even get tested.
The death rate now has to be based on the percentage of people who test positive even though many people who are infected with no symptoms will still not be tested.
The death rate has to be based on two estimates:
How many people are guessed to be infected
How many people are guessed to have died “from COVID”
There’s no way 1 of 100 infected are dying from COVID now.
I would bet you the 25 percent portion of the Brooklyn Bridge that I own that you are wrong!
If we look at North Dakota, more than 1 out of 1000 North Dakotans have died, mostly since September (https://www.worldometers.info/coronavirus/usa/north-dakota/). Excess deaths (https://www.nytimes.com/interactive/2020/05/05/us/coronavirus-death-toll-us.html) run higher than counted coronavirus deaths. So call it 1.5/1000. Assuming that fewer than 1 out of 3 North Dakotans have caught COVID, and we’re at about 1/200 COVID infections lead to death. So not quite 1/100, but not far from that…
Farcus
First you have the issue of guessing who really died of COVID. I say no one. COVID is a contributing factor with other medical problems and/or genetic weaknesses involved too. Whether or not the other medical issues were known at the time of death.
Then you have the problem of under counting deaths related to ordinary influenza, resulting in over counting deaths attributed to COVID.
Then you have the trend of doctors finding ways to keep patients alive.
Then you have the trend of finding out, through testing, that the percentage of the population currently infected, or who had been infected, is higher than ever expected.
And many infected people with no symptoms will never be tested. The estimated percentage of people infected with no symptoms is rising too.
The percentage of all Americans infected, whether they know it or not, who die from COVID, has been declining rapidly since April 2020.
A1 % or 2% death rate of all infected people is old news biased by poor results last Spring — old numbers — not the current situation, which is much better for deaths as a percentage of TOTAL estimated infections, and not just those detected with tests .
Richard Greene wrote, “Dave Burpin…”
How did you know about my GI issues? Wow, that’s spooky.
As for the case and fatality counts, I gave you the links, you can check the figures for yourself. (Hover your mouse over the worldometers “Total Coronavirus Cases” and “Total Coronavirus Deaths” graphs to see the exact figures.)
The U.S. Covid-19 case fatality rate rate in April can be calculated very closely by dividing the number of deaths in weeks 2-4 (April 8-29) by the number of new cases in weeks 1 to 3 (April 1-22). The answer is 7.0%.
However, in April probably more than half of U.S. Covid-19 cases were going undiagnosed. It might have been as high as two-thirds. If two-thirds of the cases were never diagnosed (which is on the high end of plausibility), and if the number of deaths was only slightly underestimated (which is doubtful!) that would make the true fatality rate 1/3 of 7% = 2.3%.
It was probably higher. It could not plausibly have been much lower than that. I would bet you my entire stake in the Brooklyn Bridge, plus a silk pajama, that it was over 2%. (That’s a literary reference.)
You are correct that (inexcusably!!!) most people in the U.S. with asymptomatic Covid infections still are not being tested for it, even now, even if close family members have confirmed infections. Additionally, many people with only mild Covid symptoms, not requiring medical attention, are not being tested, either, even when they have been in close contact with confirmed cases.
That suggests that as many as half of U.S. Covid-19 infections still might be going undetected (though it’s probably not quite that high, anymore). If so, and if Covid-19 deaths are by now only slightly undercounted, that would mean the calculated recent fatality rate of 1.03% could be as much as twice the true IFR.
That would make the true IFR for recent cases only about 0.5%, which is a very dramatic improvement from the early days of the pandemic.
Dave writes:
I survived it. At 65 yrs of age. BUT then I am in fairly good shape and had started bicycle riding in a big way in March of this year. Had acute shortage of breath and could hear ‘bubbles’ popping upon complete lung exhausting (not unlike the sound I heard when I had pneumonia in 1995) in the late August-September timeframe. Also had nightmares and felt as if something ‘heavy’ was in my lungs when I laid down. Am back to normal now, ‘pulling’ up hills (on the bike) like before (could NOT quite do that when the Covid was impacting me.) I do think anyone significantly out-of-shape could have been QUITE adversely affected, and required hospitalization/intubation etc.
I wonder how many other ppl had this experience as I did?