Posted by Jeff Id on July 3, 2020
Treatment with Hydroxychloroquine, Azithromycin, and Combination in Patients Hospitalized with COVID-19
A new study of over 2000 hospitalized patients reveals that Hydroxychloroquine works very well in treatment of COVID. The reason I’m so excited about this one is because unlike the poor studies that I’ve written about already, this study controlled the dosages, use the correct levels of HCQ and Azythromycin per other studies, and matched patients to each other by their own health situations. This matching of health condition is the proper method to control the confounding factors in a situation where testing cannot be double-blind. The health of the patient is what the frustratingly fake studies didn’t correct for, but certain political pressures made them popular.
This is absolutely the most conclusive research produced to date by anyone, due mostly to the quality of the approach. No one has published this quality level of work on HCQ on humans prior to this.
HCQ reduced deaths by half from the untreated patients.
Of note, this was a very large study:
The results of this study demonstrate that in a strictly monitored protocol-driven in-hospital setting, treatment with hydroxychloroquine alone and hydroxychloroquine + azithromycin was associated with a significant reduction in mortality among patients hospitalized with COVID-19. In this study, among one of the largest COVID-19 hospital patient cohorts (n = 2,541) assembled in a single institution, overall in-hospital COVID-19 associated mortality was 18.1% reflecting a high prevalence of co-morbid conditions in COVID-19 patients admitted to our institution.
And Safe:
To mitigate potential limitations associated with missing or inaccurate documentation in electronic medical records, we manually reviewed all deaths to confirm the primary mortality outcome and ascertain the cause of death. A review of our COVID-19 mortality data demonstrated no major cardiac arrhythmias; specifically, no torsades de pointes that has been observed with hydroxychloroquine treatment.
My bold of course. That means that HCQ is still not dangerous folks!!
Look at this powerful result:
The Cox regression result for the two propensity matched groups (Table 4) indicates that treatment with hydroxychloroquine resulted in a mortality hazard ratio decrease of 51% (p = 0.009). The resulting Kaplan-Meier survival curves within the propensity matched setting displayed significantly better survival in the hydroxychloroquine treated group, with the enhanced survival persisting all the way out to 28 days from admission (Fig. 2).
Also:

I found it very interesting that the Azythromycin didn’t work as well in combination with HCQ but it did better by itself than no treatment. I also found it a little overly deferential in its recognition of the bad papers which others have produced, but those who know me probably aren’t surprised by that.
I want to thank all of these researchers who did their job so well. Saving lives the right way.
Samia Arshad, Paul Kilgore, Zohra S. Chaudhry, Gordon Jacobsen, Dee Dee Wang, Kylie Huitsing, Indira Brar, George J. Alangaden, Mayur S. Ramesh, John E. McKinnon, William O’Neill, Marcus Zervos, Henry Ford COVID-19 Task Force<ce:author-group id=”aug0010″>, Varidhi Nauriyal, Asif Abdul Hamed, Owais Nadeem, Jennifer Swiderek, Amanda Godfrey, Jeffrey Jennings, Jayna Gardner-Gray, Adam M Ackerman, Jonathan Lezotte, Joseph Ruhala, Raef Fadel, Amit Vahia, Smitha Gudipati, Tommy Parraga, Anita Shallal, Gina Maki, Zain Tariq, Geehan Suleyman, Nicholas Yared, Erica Herc, Johnathan Williams, Odaliz Abreu Lanfranco, Pallavi Bhargava, Katherine Reyes, Anne Chen
Well done!
Are “Tips and Notes” no longer monitored?
Doesn’t seem like it. I stopped putting things there quite some time ago.
SMC,
Sorry it seems that way. I’ll lean more on T and N as a source.
Hey, a quick question. What is that website, like Twitter, where multiple msgs can be sent and received? Sounds like “parlay” or “parier”.
Here:
https://home.parler.com/
Check your email.
Thanks for getting in touch!
Why do you ask?
I also believe that in this study the HC and associated drugs were administered *before* the patients were at death’s door unlike most of the other studies. If the drugs are applied when the symptoms *begin* to become severe then they have a chance to prevent them from becoming deadly.
I am also curious if the HC and combinations shortened the time till the patient became covid free? Or if it didn’t affect the timeline very much.
“I am also curious if the HC and combinations shortened the time till the patient became covid free? Or if it didn’t affect the timeline very much.”
I’m interested in this, too. The French study done a few months ago with HCQ claimed HCQ cleared the body of the Wuhan virus in from six to nine days.
I would like to know if this treatment reduced the time in the hospital for these patients. Wuhan virus patients spend something like 30 days or more in the hospital. I assume this is without HCQ treatement, so I would like to know if the HCQ treatment reduces this hospital time
It seems the quicker one can get this virus out of the body, the better off you will be, since Wuhan virus continues to do damage as long as it is active.
The length of hospital stays is one thing that is different for the Wuhan virus as compared to the regular seasonal flu. Reducing the length of hospitalization would be a huge benefit to all.
…well what did the market say – did Remdesvir lose share value?
Follow the money
There is much confusion over the role of HCQ regarding the stages of the disease. This diagram is helpful:
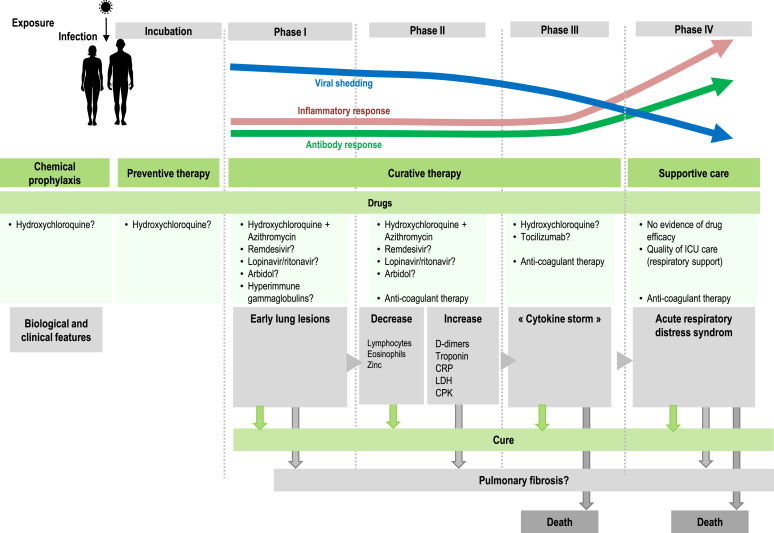
The Michigan study concerns sick, hospitalized patients and reports results in stages I and II.
“As doctors and scientists, we look to the data for insight,” said Steven Kalkanis, CEO of the Henry Ford Medical Group. “And the data here is clear that there was a benefit to using the drug as a treatment for sick, hospitalized patients.”
Previous studies, such as the French ones, were successful giving doses soon after testing positive for the virus, and before requiring inpatient care
https://rclutz.wordpress.com/2020/07/03/michigan-gets-results-with-hcq/
The Chinese are claiming that patients that were taking HCQ daily for autoimmune diseases are not even contracting SARS2, suggesting that it is an effective prophylactic. The earlier the better, obviously.
Roy Spencer had an article on his blog in Mid-March showing that nations with the highest malaria rates, where HCQ usage was high, had extremely few COVID deaths.
I sure would like to see an update of that article.
Some of those countries now have the highest number of infections and deaths in the world.
Which ones? Not India, that has a very low rate compared to population. No countries in Africa are showing large signs, how about Indonesia, nope. Not sure what countries you are talking about.
The observation was, IIRC, that places with malaria seemed to have little or no cases of COVID.
Since then the disease has spread into many countries that have malaria.
Brazil has malaria, and one of the worst infection rate.
There are plenty of other countries with malaria and COVID.
The thing is, places with malaria tend to have a greater chance of being poor countries where not as many people travel, places where health info is probably not reported as well, places with less extensive networks of roads, less likely to have large gatherings of people for sports and concerts and movies and restaurants, etc.
Tend to be.
Besides, the older drugs are not as effective and may be useless, and CQ and HCQ is not very widely used as one might suppose based merely on rates of malaria.
One might look at the malaria incidence map of the world and the places where viral disease rates are high, to see if there is some antiviral effect from malaria treatments.
In fact, places where there is malaria also have some of the worst rates of many viral illnesses.
One other thing occurs to me, which is that places with malaria endemic and widespread may have fewer old people with lots of health conditions, who are the ones mostly dying.
It looks to me that COVID correlates fairly closely with the inverse of poverty rates. Lot’s of wealthy people who travel extensively seems to be the places where it went to first.
It should also be noted that whatever can be said at the present time is only true “so far”.
Maps of malaria and COVID:
http://3.bp.blogspot.com/-GiDfJ2htZDk/TZo0CpX9byI/AAAAAAAAHlI/8D40OpJSUrA/s1600/malaria+map+1.jpg
https://www.cnn.com/interactive/2020/health/coronavirus-maps-and-cases/
I am not vouching for the accuracy of any maps, and I would not take it for granted that everyone is reporting accurately and in a timely manner on COVID.
That was months ago, RBT.
More extensive worldwide data thoroughly refuted any such contention.
It was never more than internet rumor anyway.
Lots of people with lupus on HCQ have gotten sick, many have died.
It does not prevent corona virus, or any other virus, from infecting human beings.
If only people were actually monkey cells in a dish.
To mimic a commercial from the 1980’s “Where’s the Zinc”? Should I get infected, I want the 3 part cocktail. One of the hero’s in all of this to me has been Dr. Didier Raoult. Fauci, he’s in the same neighborhood as Mann.
Just think how well the outcome would have been with zinc’s inclusion. It’s like lessons learned go out the window.
Oh well, send some more COVID-19 patients to nursing homes.
And also if the patients had been given HCQ at the onset of symptoms.
Lots of Dementocrat states have egg on their face now, banning the treatment because Trump touted it.
“Lots of Dementocrat states have egg on their face now, banning the treatment because Trump touted it.”
It would be interesting to see how many people did *not* use HCQ because of the political games being played around it. It would also be interesting to see how many people took HCQ despite the politics.
Of the 47k-plus deaths in NY & NJ, how many could have been prevented? Moralities in about half the states are less than 1/10th that of NY & NJ (deaths/1M pop). Lets hope they can keep the numbers down. Lot of factors at play of which HCQ is one.
Mortalities do not necessarily track moralities;<)
Certainly a lot of the deaths in NY nursing homes could have been prevented simply by not sending chicom-19 patients there.
Scissor. Red meat and chocolate are the high natural sources of zinc that is readily available.
https://www.healthline.com/nutrition/best-foods-high-in-zinc#section9
“…a 100-gram (3.5-ounce) serving of raw ground beef contains 4.8 mg of zinc, which is 44% of the Daily Value (DV) (4). (measured before cooking)”
6 Oysters, 291% of DV!!, crab 100g 69%, 100g dark chocolate 33%
There is always some Zinc available in the body, but the ionophore function of the HCC is enhanced by adding more to push the reaction. Once it is in the cells, it is, after all, the Zinc that eliminates the virus by interfering with the cell’s RNA transcriptase (and two other enzymes) that the virus hijacks to replicate itself.
The HCC + Zinc has been found to be most effective as early upon onset as possible. Makes sense… The Azithromycin is to prevent adventitious infections in the lungs (and elsewhere), after the virus starts its destructive work.
Why the primary role of Zinc is almost always neglected in these “studies” is beyond me. Don’t these “doctors” (of what, we might wonder) understand the biochemistry of this situation? Certainly Zinc is intentionally left out of the Pharma-funded “studies,” to assure their failure and maintain hope for fortunes to be made by selling patent-protected “drugs” from their intellectually- and morally-bankrupt mono-molecular paradigm and market (and political) dominance.
This whole Covid frenzy is so profoundly corrupt, based as much on politicized science as is the climate manipulation. Equally embarrassing is how the Trump Derangement Syndrome of the left immediately disqualifies anything the man says, without any critical or objective examination.
There are two issues with zinc that most people probably are not aware of.
The first is absorption, which decreases with age. Some zinc supplements are better absorbed than others (zinc oxide is probably the worst). Zinc taken with vitamin B6 and magnesium (ZMA is one form) increases absorption significantly.
The second is bio-availability. Selenium is required to release zinc from its transport protein (metallothionein) and make it bio-available. There can actually be an abundance of non-bioavailable zinc because of a selenium deficiency. So selenium supplementation with zinc is advisable.
You say “zinc absorption decreases with age.” Is it possible that zinc absorption explains the decreasing survival rate with age? Where do people normally get zinc (e.g. from the water supply?)
Good question. I looked it up:
https://www.myfooddata.com/articles/high-zinc-foods.php
One Centrum Silver supplement tablet for men has 100% the daily recommended amount. I’m taking zinc supplements too.
A well balanced diet should take care of a person’s need for zinc. I see that shellfish have high levels of zinc, and some nuts. Grains and milk also provide zinc along with other essentials for good health.
They get zinc from food.
The surprise I had was that the HCQ worked as well as it did, given they did not supplement with zinc. That is quite an oversight. Don’t they read?
There is also no mention of the level of vitamin D shortage, specifically they should test blood for the 1,25 form. It was me, I would take 400 mg HQ or quinine, 50 mg zinc and 5 times the daily recommended dose of vitamin D. Oh wait, that’s what I took. After starting I felt progressively better within 18 hours.
Chronic vitamin D deficiency is major problem. The total cost of that treatment package is less than $50. If you get into serous trouble, add molecular hydrogen (from an electrolysis unit). Split the water (takes about 13 amps) to make a litre of combined gas per minute. Breathe that plus anything else you need – typically 10 l/min. You want ~5% H2. That takes care of the cytokine storm.
All molecular details at the Molecular hydrogen institute, or MedCram. Free.
@Crispin – when admitted, a patient gets a full blood panel as a matter of course. Any deficiencies (of whatever, not just D and zinc) would place the patient into the appropriate propensity grouping.
Alternatively, these are early progression patients, presumably still able to eat. Hospital dieticians are worse than the strictest of parents; they will make SURE that what you are offered is “healthy” for whatever your medical profile is, thus correcting deficiencies. (They also have you captive – if you manage to not eat the disgusting glop on one tray, they will make the next one even more revolting to anyone with taste buds. Effective conditioning technique, there…)
hmm interesting because until the last 20yrs almost ALL Aussie tanks were galvanised steel
ie zinc coated, and most homes had copper piping
now the tanks and pipes are PVC
so weve lost 2 reliable lowdose sourcs of vital minerals
and Aus soils are very low in iodine zinc selenium molybdenum and more
my area here is so iron heavy calcium poor its beyond annoying for gardens and supplements of calc/magnesium are really vital for stock health
I understand alcohol consumption can also significantly increases the body’s zinc requirements. This seems believable because alcohol dehydrogenase is a zinc dependent enzyme.
All foods have zinc in them.
Many have a lot of zinc.
Food has zinc because every living cell has zinc in it.
Dead ones too.
In fact human beings that are deficient in any of the dozens of essential nutrients are by drug option not healthy.
Taking a bunch of one of two nutrients will not compensate for a deficiency in any of the many others.
Friggin autocorrect!
Drug option = definition
Best sources of zinc are oysters and liver (beef and buffalo -if you can find it); best meal is liver and onions. The beef liver contains the zinc and onions contain quercetin which is also a zinc ionophore. There are other natural zinc ionophores as well. Wikipedia has a list of ionophores if you google “ionophore”. Perhaps the best Zn-ionophore is honokitiol, an extract of Taiwan cypress heartwood or Western Red Cedar heartwood. It was shown to help treat SARS Covid 1 when used with zinc according to Wikipedia and Wikipedia is well-known for discounting natural and herbal treatments and supplements. Honokitiol is also an iron ironophore which (total speculation here) could help with the Wuhan Covid-19 attack on red blood cells which kicks iron out of the heme molecule. Without iron, heme can not transport either O2 or CO2 which is probaly why patients die gasping for air and why ventilators do nothing to help.
Hi icisil, Interesting comment about selenium.
This is what I could find concerning the ‘science’ of zinc absorption and the body’s regulation of zinc in the bloodstream.
Serum Zinc blood levels only increase around 6% for those taking Zinc supplements which is interesting. Zinc supplements of more than 30 mg/day interferes with the absorption of copper. I take 17 mg/day of zinc citrate as I am mostly a vegetarian/vegan, and the highest source of zinc is in low fat beef.
The body can maintain Zinc in the blood, up to the point when there is stunting.
Zinc deficiency results in stunting. People grow less and are shorter who are zinc deficient, hence the term ‘STUNTING’.
Roughly 2 billion people are based on observed Stunting, Zinc deficient.
The blood serum level changes during time of day. The highest level of zinc in the blood is the issue. The highest level of zinc occurs during the normal, regular, daily fast period. The longer the daily normal fast the higher the level, of Zinc ions at peak.
https://academic.oup.com/jn/article/148/9/1399/5079797
Yet Again, Serum Zinc Concentrations Are Unrelated to Zinc Intakes
Data from NHANES 2011–14 surveys, reported in the August 2018 issue of the Journal, showed that the serum zinc concentrations of the 4347 children, men, and women surveyed were unrelated to their zinc intake from either diet or supplements (1). This is not the first report that serum zinc concentrations are unrelated to zinc intakes. Three recent metaanalyses came to the same conclusion (2–4).
Data from 10 randomized controlled trials and 3 observational studies in adults showed that doubling zinc intake changed the serum or plasma zinc concentrations by 6%. Thus, an adult consuming 14 mg Zn/d has a serum concentration that is only 6% higher than that of an individual consuming 7 mg/d. (The differences between serum and plasma zinc concentrations are very small and these 2 sources of circulating zinc are used interchangeably.
The term serum zinc concentrations will be used throughout this paper when the source may be serum or plasma.) A 6% difference falls within the margin of error in measuring serum zinc.
In fact, it represents only about one-fourth of the usual 22% drop in serum zinc concentrations from the peak fasting morning value to the lowest evening value about 3–4 h after the last meal (5). Meta-analyses done in children and pregnant or lactating women also found small changes in serum zinc when dietary zinc was doubled (3, 4).
Doubling dietary zinc predicted a 9% increase in serum zinc concentrations in children, a 3% increase in pregnant women, and only a 1% increase in lactating women. These results along with the NHANES data in the August 2018 issue (1) suggest that strong homeostatic mechanisms are in place to prevent deviations in serum zinc when dietary intakes fluctuate.
Late to seeing this posted here. Been trying parler….
Henry Ford also is doing their WHIP prevent study, also no zinc.
Do not for get AASP FDA plus suit.
Follow here: https://www.courtlistener.com/docket/17221869/association-of-american-physicians-surgeons-v-food-drug-administration/
DRAGS on..
high zinc intake also correlates with higher risk for cancer.
One Dutch doctor using it against Covid-19 recently called HCQ the gun and zinc the bullet…
Why shoot blanks?
Please cite evidence of HCQ as zinc ionophore.
Assertions are not evidence, and CQ is not HCQ
Please stockpile to veritable facts when making unqualified assertions.
By the standards used here, snake oil is a miracle wonder drug.
Nicholas McGinley July 5, 2020 at 5:36 am:
Calling something “snake oil” shows just how misinformed your are. Snake oil refers to something charlatans try to sell to seek profit. In this case, you are the Snake Oil salesman. You see, no one who claims HCQ and Zn helps people stands to profit from that information… You, on the other hand, parrot from the people who stand to profit from the death caused by ignorance you peddle.
HCQ is a derivative of Chloroquine. Both are Zn ionophores. You need to prove that it is not a Zn ionophore.
Watch a MedCram video or go to a medical site, and prove them wrong. Meanwhile, the world will move on and survive from the drivel of your ilk.
I do not need to do anything.
I do not need to prove anything.
As to your contention that something is taken to be true until proven false, is as contrary to how the scientific method works as anything that anyone could say or think.
IOW…your contention that I need to prove it demonstrates a profound ignorance.
Ironic that you do so in public while thinking you are being smart, and do it on a site which has, arguably, mostly been focused over many years on proper application and understanding of how science actually works, as opposed to how warrantless supposition and unfounded ideas pollute so many minds.
Nicholas: I do not need to do any such thing, and you can call it whatever you like. You’re the guy who’s been on a diatribe asking people to jump through hoops. We the science is already out, and the mechanisms behind HCQ and Zn are already known. So keep on chasing windmills with your dull sword
When I make an assertion I back it up.
If you do not understand the distinction I am not surprised in the least.
The null case is the default position of any proposition.
Some are asserting all quinine derivatives are zinc ionophores.
If true it should be easy to find some research to back that up.
Unless you have a terrible memory, you know that I only brought up this point regarding HCQ not being shown ZI, after I looked for and could not find any research to back it up.
Lots of people have made the assertion, and if you follow the references they offered, it all leads back to the research on CQ.
Knowing something for which no proof or even evidence exists is a well described phenomenon…it is called faith.
So we might presume that since you refuse to offer any evidence, your believe is based on faith.
Kind of an odd religion, but you can believe whatever you want.
Getting back to the specific case, please do tell which viral illnesses can be cured by which antimalarials.
Is it specific or general?
Do you think all quinolones or quinine derivatives are zinc ionophores?
Do you think zinc is an antiviral with broad efficacy against a range of virus types?
Or is it effective against all coronaviruses and not other viruses?
If so, why?
The logical conclusion of the assertions made re zinc ionophores and zinc and viruses is that all quinine derivatives ought to cure all diseases caused by viruses.
Explain why this is not the case.
You can’t.
No matter what you say, unless you point to some evidence, you are simply talking, and are professing a religion, not anything to do with science.
Nicholas:
You are a confused man. Just because you said something before, does not make it true –yet you claim yourself as a source without even a quote.
In vitro has shown HCQ to increase Zn concentration in cells. That is why it works to save lives. It also increases pH of the cytoplasm, another indication of crossing the boundary into the alveolar cells. Only you can heal thyself but admission of failure or continue your blather.
To help out your further confusion.
Quinine is not HCQ, or CQ. Do I need to prove that too?
Mario,
No one in the world has ever posted a shred of evidence that HCQ has the effect on zinc you are asserting here.
HCQ is not listed on any compilation of known ionophores.
You can say it, and it will not make it true.
Despite what you think, I am a researcher, and I am a trained chemist, and I know that of which I speak.
Condescension does not wear well when you are forgetting that I am the most vocal person on this blog about keeping clear the distinction between these molecules.
You forget, but I recall vividly, when I was posting about these molecules at length.
You did not enter the conversation then, because back then you did not pretend to be an expert on material you have no expertise in.
Here is a comment from April I made in which I gave a long talk on the physical properties of the CQ and HCQ molecules.
Interesting thread.
Krishna congratulated me for being the first person on this site talking about things like infective dose:
https://wattsupwiththat.com/2020/04/24/coronavirus-covid-19-and-rumination-6/#comment-2976711
In fact I have ben a though leader on many aspects of this virus pandemic from the earliest days.
Regulars here know me to be informed, knowledgeable, and someone who takes the time to explain complicated things so that the laypeople here can understand.
right on post..have used HCQ since Nov 19 when symptoms were apparent.. 1 week later recovery was in sight.. D Trump should receive a credit for the HcQ find.. the media and big pharma are criminals ,and may be responsible for so many fatalities.. why not bring this to bear on false narratives and biased reporting.. hang ’em all
I agree with you. It is criminal, the level of attacks on a proven safe and highly effective cure that stops replication of the virus when there is enough Zn present. The mechanism is clear and factual.
The evidence is clear.
Nicholas McGinley pops up like a whack-a-mole, a shill, still continuing to put forth baseless attacks on people with opposite views. When will he learn that no level of hubris can make up for clear evidence. He gets confused by words, and sets up strawman arguments. He is on the wrong side of history.
Very amusing Mario.
Your remarks are a case study in psychological projection.
You are the shill.
You are attacking me.
Your attack is baseless, ands you make it because I do not share your faith.
I am not stupid enough to think anything one can say one any topic in medicine or science is purely binary, so I have no idea what an “opposite” belief or view is.
Your evolution into a rabid foaming at the mouth advocate for something for which no clear proof and very little evidence exists, has been eyepopping.
I recall when you where certain that vitamin A was the important ingredient in fighting COVID and disease in general.
As for those last remarks, you are a largely uneducated dolt, steeped in internet lore and little else, as far as I can tell.
It is impossible for me to be on the “wrong side of history”, because I go with the evidence.
If the evidence changes, so will I.
You do not even know of any evidence except that which confirms your faith, whereas I have very comprehensive knowledge and recall of the whole story, including your evolution to your present state of mind.
You have changed your mind so many times, and said so many things were known to be true which have been refuted…well…it seems literally every word you said about me is demonstrable true of yourself.
Nicholas: You started the drive by assaults (on other people’s posts) on my character several weeks ago. You lied about me in generalities saying that I was also on all sides of this issue. You simply maligned me making stuff up and would not respond by using quotes to back up your false assertions.
That you are trying to hide, literally the best treatment for RNA viruses, with your dull obfuscation using the MSM to support your drivel, would be considered evil if you actually knew what you were doing.
I am not convinced you know better, and I never called you evil, but you are a useful shill for the cause.
Here’s an example of how confused you are:
Quote from the McGinley:
“As for those last remarks, you are a largely uneducated dolt, steeped in internet lore and little else, as far as I can tell.
It is impossible for me to be on the “wrong side of history”, because I go with the evidence.
If the evidence changes, so will I.”
So, you deny there is evidence?
You accuse me of an Internet lore, after you site opinion pieces from MSN.com?
Projection is when someone does what they claim others are doing. You just showed your cards. Look in the mirror and read this post, trying not to laugh.
Do you understand the term evidence? Evidently you do not.
So you can’t get your stories straight, writing that evidence is not evidence unless the McGinley says so.
You make claims about my education. Nice try… you are batting zero.
It’s disappointing that the mainstream scientific community is so corrupt. This is useful as confirmation. No one should listen to these people again.
“No one should listen to these people again.”
huh, these people doing this study ARE THE MAINSTREAM SCIENTIFIC COMMUNITY
look it is not uncommon for medical studies to come to contradicting answers
Look what we were told by believers.
1. you have to start early Before hospitalization: this trial did not
2. you need zinc: this trial did not.
Of course there are “answers” to both of these, but More science is needed, not less.
would I take HCQ? well, I would talk to MY doctor and we would come to an agreement.
that would be my choice. Probably yes, pre cautionary principle.
can I recommend it for you?
no
why?
because YOU have to decide with YOUR doctor and because the science is not settled.
I would not tell you medical advice, only a process for deciding. Talk to your doctor.
get a 2nd opinon.
can I declare it a cure? nope. no RCT.
evidence based medical science relies on RCT. that’s the standard of proof. anything less than that
is an opinion. it can be an opinion backed up by strong evidence, but the gold standard is RCT.
You can decide for yourself. You can’t decide for others.
+07042020!!
Well Steven, you should have said that to CNN and the rest of the lame stream media that always “decide for others”.
It’s a study how HCQ works and they find: yes, to some degree. It’s not a study about “class-fighting” and in the view of a German from the other side of the Atlantic it makes me breathless how every result any study is politcised in the USA. It won’t help against the virus! There is research needed in medizine and mathemetics but not research if CNN or Fox is right.
The problem with HCQ in the USA is that politics took the place of medicine as soon as Trump said something good about HCQ.
Well Dr Fauci is pushing rehmdeviri as a game breaker, but the results are not as good as these. Funny that the drug is a high priced drug that he personally Is connected to. There has been hundreds of doctors saying the HQ works but the scientific community has been pushing the story that it doesn’t work and that it’s dangerous. That fact that you can’t see the unending establishment bias,Steven, is ridiculous.
Did I see it stated somewhere that the cost of rehmdeviri was going to be $3,000 per patient?
Yes, I’ve seen that price tag mentioned in several places!
This whole escapade can be explained by “Follow tbe money!”
It also parallels what “established science” says about climate change and so extreme caution should be applied!
There is undoubtedly a hidden political agenda involved in both cases!
Would you change your life based on atmospheric CO2 levels?
Would you recommend others change their lives to accommodate your belief in what the changing CO2 levels might mean to you?
Would you support mandates that others change their lives?
If everyone was mandated to change their lives, in the manner prescribed by mainstream believers that increasing atmospheric CO2 level is dangerous, would you call it a cure?
If you knew of lies and misinformation peddled on behalf of the cure would you keep it to yourself, or would you play along because of your individual belief?
no
why?
because YOU have to decide with YOUR doctor and because the science is not settled.
I would not tell you medical advice, only a process for deciding. Talk to your doctor.
get a 2nd opinon.
can I declare it a cure? nope. no RCT.
Pharmaceutical outlets weren’t as liberal as they should have been–they were actually questioning doctors regarding the use of NHCQ!
Some doctors told the pharmacists to go pound sand–it was none of their damned business what they were using it for, or the how or the when!
I saw where a lawsuit was brought by the Association of Surgeons and Physicians against the pharmaceutical industry demanding that they refrain from interfering in the practice of medicine; that’s the doctor’s job, not the pill supplier!
Mosher: Why do you think an RCT has not been done yet?
HCQ has been the most important finding for humanity to treat for RNA virus –it works and is cheap. That is why RCT studies are taking so long. Politics.
So we are forced to go by old fashioned science using observation and best practices. Doctors can be afraid to use best practices because the MSM and Dem’s are trying to falsely claim HCQ is dangerous and there is no proof it works.
I am sick and tire of the intellectually dishonest arguments.
Cut the BS Mario.
Saying such things will never make them true.
https://www.msn.com/en-us/health/medical/hydroxychloroquine-is-the-most-disappointing-disavowed-drug-that-researchers-keep-studying-for-covid-19/ar-BB16glaE
Well said Mario
https://aapsonline.org/aaps-news-june-2020-aaps-sues-fda/
@Nicholas McGinley July 5, 2020 at 5:43 am
You wrote:
“Cut the BS Mario. Saying such things will never make them true.”
_______________
You’re a tired and confused being who does not understand the subject matter. You have been on the wrong side of arguments, and are acting like a cornered rat. Nice going.
rick July 5, 2020 at 9:41 am
“Well said Mario”
____
Rick Thank you. Nicholas pops his head up once in a while and rants, not seeming to understand the written language.
Nicholas McGinley July 5, 2020 at 5:43 am:
The link you sent is from MSN and shows how illiterate you are. No one cares about opinion articles. Maybe you had forgotten that people here are interested in the science. You are not an honest broker here. But I do love hearing how the other side thinks. The other side in this case is against humanity.
Nicholas McGinnley: You said HCQ is not a Zn ionophore. It’s not hard to find medical references that prove otherwise. Evidently, you just are not smart enough to know. It’s not my job to make you smart enough to engage. However, here’s some help. Waiting for you to make up some more stuff.
Excerpt from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7202847/
“From in vitro and some clinical studies, it is well known that zinc elicits activity against several viruses [14]. Indeed, it was demonstrated that zinc inhibits the activity of RNA dependent RNA polymerase (RdRp) of Hepatitis E virus [15]. It was further shown in vitro that zinc inhibited coronavirus RdRp activity and that zinc ionophores blocked coronavirus replication [16]. Despite the well-known antiviral effects of zinc and possible properties of CQ/HCQ as zinc ionophore, the combination of zinc with one of these established drugs to achieve additive or even synergistic antiviral effects ought to be still confirmed.
The Thomas Sowell quote from another WUWT post applies directly to Nicholas McGinley :
“The problem isn’t that Nicholas can’t read. The problem isn’t even that Nicholas can’t think. The problem is that Nicholas doesn’t know what thinking is; he confuses it with feeling.” ―
That is the best advice Quick Nick McGinley could have taken. That is priceless.
It is obvious you never opened the link.
It is a article from the Philadelphia Inquirer.
It does not matter who says something, but whether it is true.
You can puff up your chest and pretend to be a scientist, but you are not.
And I am.
No one should listen to these people again.
No one should listen to the media again.
President Trump touted HC back in March and the media pooh poohed it the next day.
I believe that was based on an article in the Lancet and since then, that Lancet article has been withdrawn!
But was that retraction widely broadcast?
It appears that fact was seldom if ever mentioned!
Follow the money; follow the politics!
Is Raoult using zinc in his studies? I couldn’t believe it when I saw no zinc in the Lancet study, which turned out to be bogus anyway – perfect Guardian material. Probably excellent class-action lawsuit material for the ambulance-, ooops hearse-chasers.
Here is a detailed account of a retrospective study with data collected from 1061 patients between March 3rd to March 31st at the IHU – Méditerranée Infection, Marseille.
A new study of 3737 patients will be published soon I believe.
https://www.sciencedirect.com/science/article/pii/S1477893920302179?via%3Dihub
Thanks. No zinc to be found in that study either according to a simple word search. Strange. I’ll try to get to the bottom of this later, but looking forward to the new study results.
I heard Raoult talk briefly about zinc supplements in an interview (can’t find it yet). My guess is that it might be included in the standard vitamin package at the IHU Marseille considering it”s a big structure capable of extensively testing patients.
Here’s the 3,737 patient study. I haven’t had chance to read in detail yet, but they did measure zinc levels:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7315163/
One of my children’s family in London contracted Covid in April. I got them to get tonic water, zinc and vita D and sent info on results of Drs Didier, Zelenko, etc on HCQ/Q +. The rest of my family also came to be fond of gin and tonics! At the time, I was the best doctor they had in lefty lands Canada, UK and South America.
I think class action suits would straighten out the barbaric political behavior resulting in so many deaths in states where this “no regrets” treatment was banned and the egregious massive overdose tests set up to fail should be criminal trials. One can argue that they didn’t have double blind, controled trials, but they went beyond that and vilified HCQ as a dangerous drug despite the hundreds of millions of people who have taken it for over 70 years and quinine since the 1500s! These ugly people deliberately executed patients with massive overdoses for politivmcal reasons. How can these people live with themselves!
Couldn’t agree with you more.
It is dangerous for the same reason snake oil is dangerous.
It does not work.
Raoult no longer used it.
In fact France has made it illegal to prescribe or use it for covid.
Clinical trials using it are banned and halted…over a month ago in France.
At this point the rationale for taking it seems to be it kills few people and does not cost much.
There was never any valid evidence for widespread usage.
If a few well controlled studies were done months ago, by now we could be focusing on treatments that might actually work.
If course efficacy may come with a price tag, so I am sure many will prefer “cheap” to “effectuve”.
But fauci said its No good, and trump taking it means its a big no no, I believe it as the news media told me so…
Also protesting AKA smashing up cars and looting businesses, beating up people for BLM is ok and the corona virus can’t touch me, but if I go to a trump rally or walk on the beach or see my grandparents, I am a killer…..
Remember the news doesn’t lie 😀
No truth in the news because there is no news in the truth.
I wonder how many people died because of the anti-Trump media and the swamp dwellers.
It’s pitiful that the progressives and anti-Trumpers are willing to let people die because of their absolute hate of Trump. If Trump would have been against HCC, the media and the swamp dwellers would have declared it the miracle drug. Sad times in the world.
Mr. Lowe: You’re on to something there. Obviously, Trump should have come out against it, knowing that american press (predictably) would promote it and save lives. So, once again we see how Trump is evil and killed people. I think the press will know how to play this. /sarc.
Anyone who is trying to arrive at an assessment of efficacy based on who loves it and who hates it, will have a very hard time ever getting around to simply and objectively determining what the actual scientifically valid data is telling us.
How many will die because they think politics and choosing sides can inform us regarding therapeutic efficacy of drugs?
I for one may die of severe mental anguish over the scientific illiteracy and biased opinionating of presumably rationale people.
I guess CQ and HCQ are sooooo dissimilar that it’s not even worth testing a hypothesis…
————————————————————–
Chloroquine is a potent inhibitor of SARS coronavirus infection and spread
Martin J Vincent, Eric Bergeron, Suzanne Benjannet, Bobbie R Erickson, Pierre E Rollin, Thomas G Ksiazek, Nabil G Seidah & Stuart T Nichol
Virology Journal volume 2, Article number: 69 (2005) Cite this article
The Centers for Disease Control and Prevention can not recommend a treatment, previously recommended by President Trump.
I have to ask, what were the other patients treated with: harmless placebos, nothing, or the usual toxic experimental drugs? Is this a case of HCQ actually benefiting patients, or of simply harming them less? I’m agnostic towards HCQ; it seems to help, but does this study actually show that?
HCQ in combination with azithromycin reduced the covid death rate by 71%. 71% REDUCTION IN DEATH RATE. Wow… Wow….
CNN and BBC have not reported this amazing discovery. It looks as if the Lancet study, which concluded that HCQ had no clinical benefit and HCQ caused heart damage…. Blah, blah, blah,…
Has a fake scientific study done for political reasons.
…at time of a pandemic, a fake scientific study, hiding the only known treatment for Covid (71% Reduction in death rate, 500,000 deaths to date) is
…. Treason and mass murder.
People are dying of Covid because of CNN and BBC fake news. How long is going to take before the Left wing discusses the HCQ and azithromycin game changer.
It is know that HCQ is a zinc ionophore (it gets a tiny amount of zinc Z+2 into our negative charged cells) and it has been proven the Z+2 ion if it gets into our cells, stops the covid virus from replicating.
The standard treatment for all patients showing Covid symptoms should be and will be, HCQ & Azithromycin & (Zinc Sulfate?)
P.S. I have found out some interesting things about Zinc. Zinc citrate supplements have very little effect on available zinc in the body stream. That is why Zinc Sulfate is in parentheses with a question mark.
How long will it take and how many people will have to die before HCQ and Azithromycin is used as the standard Covid treatment?
Hydroxychloroquine provided a 66% hazard ratio reduction, and hydroxychloroquine + azithromycin 71% compared to neither treatment (p < 0.001).
https://www.ijidonline.com/article/S1201-9712(20)30534-8/fulltext
Treatment with Hydroxychloroquine, Azithromycin, and Combination in Patients Hospitalized with COVID-19
It looks as if the Lancet study..
The Lancet study was retracted….they refused to give any of their data
…now why would you make up some excuse to not give any of your data
retracted > https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31180-6/fulltext
…when this study uses the exact same data….and they had no problem at all releasing every bit of it
“How long will it take and how many people will have to die before HCQ and Azithromycin is used as the standard Covid treatment?”
I think refusing to prescribe HCQ is against the law.
President Trump signed a bill into law a few months ago called “The Right to Try” law, giving people the right to try any drug available, even experimental drugs not approved by the FDA, if they thought the drug might save their life.
It looks to me like HCQ is right in that category.
What needs to happen is publicizing the results of this study giving people notice that HCQ is an effective treatment. Then the people can take advantage of the “Right to Try” law.
Unfortunately, it looks like this study has been blacked out on the Leftwing News Media. First, they actively discourage people from taking HCQ, and now that it shows effectiveness, they bury the information and end up destroying more people’s lives. And all of it is for political gain. Sick people are just collateral damage to the lying Leftwing News Media when it comes to gaining political power for the Left.
Unfortunately, the right to try law only kicks in when there are no other accepted options, and you are going to die.
With COVID-19 that means that it’s too late for anything to be effective. Treatment needs to happen as early as possible to work.
William,
“From the limited published data on the absorption of zinc from supplements fed to humans, it would appear that zinc gluconate, zinc citrate, and zinc sulfate are absorbed to a similar extent and that zinc oxide is slightly less well absorbed (7, 8).”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3901420/
icisil
July 3, 2020 at 4:43 pm
It seems this study clearly shows the HCQ being beneficial and helping.
Yes, it could be that it does both, helping directly with the condition as a positive treatment, and also indirectly, by blocking the wrong and very risky-dangerous treatments from being applied.
Even Mosh sees it that way. 🙂
cheers
That is problematic as there are ample examples where a retrospective finding didn’t translate at all into efficacy in a randomised double-blind placebo controlled trial and had even problematic side effects. One of the most famous is hormone therapy treatment in women as prevention for Alzheimer’s disease. Was a big fail though the retrospective studies were very promising.
That is one of the reasons the randomised double-blind placebo controlled trials are necessary to prove benefits and efficacy. Otherwise nobody would waste time and money to do them.
Ron, What you say is not correct. There is no hidden mysterious about whether people die or do not die from a illness.
It is weird that the Medical Industry was allowed to develop the Double ‘Blind’ Test format.
Logically a treatment, for an ‘illness’, would ‘work’ or it would not. Long term follow up, sure, that makes sense. Follow checks of blood work, sure.
The Double ‘Blind’ Study format was developed for the Psychiatric Industry. It is not appropriate when treating people how are dying….
When it has been proven that there is a 71% less chance of dying when the patient is treated with HCQ in combination with Azithromycin, than not treating the patient….
There is, therefore, no need for a Double Blind Study. The patient is not going to fake not dying. The doctor did not make the patient better with his bedside manner.
In the case of the psychiatric industry, the cause of the mental illnesses, is unknown… And success is measured by what the patient tells you.
So, the pills are compared to a placebo.
Unfortunately the current psychiatric ‘medicines’ all cause long term brain damage (and the tests were only short term tests, and many of the side effects where not reported, hence the law suits), so in almost all but the most severe mental illness cases, the patient’s long term outcome is much better with no drugs than drugs. The drugs shutdown the brain which cause long term damage. The patients start to move uncontrollably which make life very difficult. They also have very early onset dementia.
https://www.amazon.com/Anatomy-Epidemic-Bullets-Psychiatric-Astonishing/dp/1491513217
Anatomy of an Epidemic: Magic Bullets, Psychiatric Drugs, and the Astonishing Rise of Mental Illness in America
You completely missed the point what the problem of retrospective studies is.
And no,
is not true. There are, as I said, ample examples that proved retrospective studies wrong when testing the hypothesis of the retrospective study as a randomised double-blind placebo controlled trial. The most famous, that raised ethical concerns bc patients were basically denied of a so-thought life-saving drug, was this study:
https://en.wikipedia.org/wiki/Cardiac_Arrhythmia_Suppression_Trial
No psychiatric drug at all. Placebos work on nearly everything to some extent. Even on the opinion of doctors that prescribe them. That is why the study has to be double-blind.
Ron.
Your comment is Mumbo Jumbo maximum. Mumbo Jumbo looks Sciency… To hide an agenda.
Ron said: “You completely missed the point… (William; OK. I am waiting for Ron’s point)
… what the problem … (William: here comes a new invented Mumbo Jumbo term) of retrospective studies is”
Ron What is a’ RETROSPECTIVE’ study…
The word ‘RETROSPECTIVE’ is mumbo jumbo….
So is your link…. to a Wiki fake article.
It is peer reviewed fact (six hospitals 2000 patients) that there is a 71% less chance of dying from Covid…
… for patients who were treated with HCQ in combination with Azithromycin…
as compared to letting the patient die.
What is RETROSPECTIVE about the HCQ tests?
A drug works or it does not.
The Double Blind Test format was developed to push chemicals to treat mental illness. There is no evidence that mental illness is due to a chemical imbalance.
The Psychiatric drugs are known to cause severe long term brain damage and horrific side effects… and statistically those taking the placebo.. had a 80% chance of complete recovery with no recurrence of the illness, while those taking the brain damaging psychiatric drugs become permanently disabled. Odd the Double Bind Study missed that fact.
The Tests were blind as they did not look at the long term outcome of the patients.
80% of the the severe depressed patients completely recovered and never had a recurring depression.
There is now four times as many ‘depressed’ people and they are chronically depressed and now have long term health effects do to the drugs. There are now 35 times as many children with mental illness and all are being ‘treated’ with the brain damaging chemicals.
That kind of menticide must lead to a mumbo-jumbo epidemic.
I wonder how much of the current mass rioting and “lazy reason” is in fact pharma drug damage, never mind the illegal stuff?
Imagine youth, “students”, holding COVID 19 parties to deliberately spread the plague?
Retrospectively, that will compete with Boccaccio’s Decameron.
You have a fundamental misconception how to prove that in a clinical trial.
Using all-caps doesn’t solve your lack of inside.
Ron,
You happened to expose the crux of the issue with your Freudian slip of “inside”, for it is exactly the political insiders that fought a resolution to a deadly serious problem!
Would you use a clinical trial to prove the efficacy of flight? The airplane either flew or it didn’t and in the applications of NHCQ, it flew a lot farther than anything else used so far!
Then you have the real specter of one side in this political battle actually using misinformation and violations of stated public health policy to boost death counts!
Why?
Because their political agenda would willingly sacrifice humans to win the argument!
Think about that!
This goes way beyond “fundamental misconceptions regarding clinical trials”!!
Way beyond!!!
@RockyRoad
You can’t convince an airplane to fly but you can to some degree convince people that stuff works although all is working is the placebo effect. Your allegory is therefore completely unfitting.
The Double Blind trial system was developed by Statisticians, not by the Medical people. In fact Medicine resisted the concept for decades but finally had to give in as the evidence that the stats in most Medical papers were frankly rubbish. That famous carcinogen Saccharin anyone? Yet the paper is still quoted today as an authority.
The reason that Double Blind trials are necessary is blank off all bias in the trial. For example we all suffer from bias confirmation and a Double Blind trial is the only mechanism that blocks this out. It is a very subtle and invasion phenomenon that is extremely hard to exclude.
Someone has been reading their Feynman…
That is a too simplistic view on history. There have been reasonable ethical concerns about placebo controlled trials in patients at risk of dying. Nobody knew beforehand that it was worth in the end. Judging from hindsight is way too easy.
William, you have now become this sites premier crackpot.
Nicholas,
If you tested positive for the coronavirus, would you take NHCQ + Zn in the off chance that it would help, or would you continue in your treck through the weeds arguing the merits of double-blind clinical studies and calling people you disagree with crackpots?
I take nutritional supplements as I have since I was a small child.
But they do not sure infectious diseases.
I would not take HCQ because numerous controlled trials have shown it to be worthless.
Would you take snake oil?
It might work too.
If you had cabcer, would you go to Mexico and take laetrile.
Tell me, by what rationale does one take a drug while I’ll because of “off chances”?
HCQ is shown to interfere with remdesivir.
Remdesivir has shown efficacy in clinical trials.
As have steroids and a few other things like blood plasma.
I would seek out quality medical care, not off chances and disproven noncures.
But that is just me.
I have survived a lot of things most people would not survive, and not by being irrational, but by being knowlagable, logical, and thorough.
Very few are dying these days Rocky.
In my demographic, the odds are very low of a fatal result.
I am not the sickly type.
Nor given to wild guesses/wishful thinking in life and death health issues.
Mr. McGinley: I think you are being rash about Mr. Astley and this site’s crackpot competition. I’m still here!
Sorry Paul, you are well behind the pack in this race.
I have never seen you to be unable to distinguish your opinions from established facts, nor to represent the former as the latter.
Ron, Exactly.
all well and fine…until you look at the fine print
neither med, median age……..71
HCQ alone…………53
AZM alone……….64
HCQ + AZM………62
…they gave neither med to the oldest age group
and gave HCQ to the youngest age group
They controlled for demographics:
Multivariable Cox regression models and Kaplan-Meier survival curves were used to compare survival among treatment groups while controlling for demographics (e.g., age, gender), preexisting medical conditions (e.g. CVD, lung disease) and clinical disease severity (mSOFA, O2 saturation).
Table 3 in the paper shows the baseline characteristics along with the propensity matched characteristics in HCQ vs non-HCQ patients. The propensity matched Cox regression result for mortality prediction for HCQ patients had a P-value of 0.009 and a Hazard Ratio of 0.487.
Something still seems wrong there. The hazard ratio not allowing for other factors is 13.5/26.4=0.51. Allowing for the younger CHQ group slightly reduces the HR.
Maybe the HCQ group had a whole lot of compensating comorbidities, but it does look strange.
You’re right about the comorbidities. If you examine Table 3, which compares the experimental groups, you’ll find that the group given HCQ had much higher BMI and diabetes than the non-HCQ group; most other comorbidities and characteristics were about the same. But their propensity matched characteristics are about the same.
Then that relies hugely on quantifying the risk of the comorbidities. Especially as they seem to use just a yes/no criterion with something like obesity or chronic kidney disease, with no gradations.
The HCQ group had mean age 53 and yet 13.5% mortality. Either they were spectacularly comorbid, or HFHS hospitals are a place to avoid, or HCQ didn’t do them much good.
It is problematic how the propensity-matched groups were selected. No information about that. Multi vs one comorbidity patients?
But what is more troubling:
71% of HCQ treated patients received a steroid, only 36% of the untreated patients. Dexamethasone anybody?
And how did they manage to get “white” as a risk factor? There is no other study that has this results but a lot that show the opposite including the vitamin D ones.
Nick and Ron,
You are both in the right track here.
This type of confounding is exactly why double blinding and randomization prior to treatment is the only way to get an objective scientific result.
If we are going to take a retrospective approach, let’s consider every study result that has been published, plus all of the doctors and hospitals that have abandoned this regimen after months of trying it on tens of thousands of patients.
It was not a clinical trial, but a retrospective analysis.
Patients had widely varying treatments besides the drugs in question.
Specifically, many more of the HCQ group got steroids, which have been shown to be helpful.
Unless the drug(s) being evaluated is(are) the only variable, the outcome is meaningless from a scientific perspective.
The VA study was similar to this, and was rejected because it showed no benefit.
At this point, all favorable data is taken as proof, and contrary data is dismissed out of hand.
The overwhelming preponderance of evidence is that SAY is worthless, HCQ is worthless, steroids help a great deal, and remdesivir shortens time in hospital by several days.
Soon trials of inhaled remdesivir will begin, which will allow people not hospitalized to take it.
This is important, because antiviral usually work best when taken early.
A while back, a huge study showing no benefit fro m malaria drugs was dismissed by this same WUWT crown because no zinc.
Now, a putative positive result is hailed as proof positive, and zinc ain’t part of the result.
Double bling trials are the gold standard because only that type of study eliminates confounding variables.
It is very simple…if there is no randomization the result is not scientific.
And the data here bears that out. Age was not the same, and other drugs were used in the various groups analyzed.
There are now dozens of study results and tend of thousands of treated patients looked at, with few showing any benefit.
Singling out this nonscientific retrospective as having greater weight than other studies that were randomized and showed no benefit is wishful thinking at best, and idiotic at worst.
The majority of people commenting on this topic here have confirmation bias, tunnel vision, selective attention, and no idea what they are talking about.
yup
science still not settled
Looks like the results depend entirely upon the values the authors choose to assign to weight the effects of age and various co-morbidities in order to be able to make a comparison at all. Disappointingly, this would appear to make the conclusions worthless.
Tick
Where did you see that? I skimmed through the paper looking for it but found no such detail. They did break it down between over 65 and under 65, that’s it. Not saying it isn’t there, but a link or page number or other reference would be of assistance.
david…table 1 graph…….Patient Characteristics by Treatment Group
third group down…..age in years…mean..median….71…53……64…..62
Yes. I don’t have US mortality/age data handy, but in Italy the general mortality went
50-59 1%
60-69 3.5%
70-79 12.8%
On that basis, the 53yo (mean) HCQ group should have done far better than the 71 yo no treatment group. HCQ looks bad for them. Even if you use the other numbers quoted of 63 and 68 years, the difference is enough to account for the mortality drop, without HCQ.
Italy is a nice cherry-pick where the elderly death rates were abnormally high compared to other countries. Of course, general mortality and those making it to the hospital are quite different as well. Seems that a number of elderly Italians died in their homes.
Age was controlled for. It has been pointed-out to you repeatedly since you missed that part in the study. This was a study of over 2,500 patients admitted to a hospital in Michigan. We know how to do these medical studies.
So what we have here is someone in Australia that vehemently attacks and denies any study or suggestion that HCQ is a benefit to COVID-19 patients apparently just because the US President touted its potential. You should do some deep soul-searching.
Nick? Soul? LOL
“Italy is a nice cherry-pick”
OK, here is US data, different age ranges
50-64 2.9%
65-74 10.4%
75-84 20.8%
They point is, the age mortality is easily enough to account for the difference between a mean age 53 and mean 71 group. On the face of it, HCQ is harming the former.
“This was a study of over 2,500 patients admitted to a hospital in Michigan.”
When it comes to the propensity-matched subgroups, there were 380.
Skimming that study on a phone, it appears those are the rates for the US population as a whole. This study is only of people sick enough to require hospitalization. Not at all comparable.
And you can not compare to other hospitals unless you know that their admission criteria and demographics are similar.
For anyone getting their news on this topic mostly here in WUWT, it needs to be noted that this site has almost exclusively published positive results, and gone full CNNLOL when it comes to mentioning the large number of clinical trial results, as well as major medical groups and large hospitals that have announced data, showing no benefit and in some cases substantial harm from HCQ, CQ, and Z Pak.
Honestly, reading these comments brings to mind warmistas and various gullible laypeople talking about global warming, who insist there are no serious people or scientists who dispute “The Science”, apparently oblivious to any and all climate skeptics and their arguments and findings.
Objectively speaking, HOW has been proven to have no value.
But you have to be aware of all the results to know this.
And be willing and emotionally capable of performing objective analysis.
The MSM could do a far better job of keeping a running scorecard of results.
But they have been conditioned by decades of climate reporting, to report the latest findings to be announced as somehow being the summary of current understanding, rather than what it is…one more data point, often a low quality one which is not comparable to previous results.
Michael, it’s hard for him to search for what he never had.
Good catch that, in my opinion, renders the results more or less worthless. I remain one who thinks HCQ will prove its worth, but the age discrepancy in this study is too large when one of the most obvious risk factors associated with Covid-19 mortality is age-related.
Obviously a misprint. Check out the next line on % above and below 65.
One obvious problem is that 15% mortality of hospitalized patients is higher than in many hospitals NOT using HCQ….
Zinc?
I am eating healthy foods, taking vitamin D supplements, normal multi vitamins and ZINC.
If I get covid I will immediately start taking HCQ.
Once again this trial is still hospital based.
My understanding is the saturated oxygen is a good indicator of your health status once diagnosed with covid.
Oxygen saturation is the only thing to be concerned about. Anyone can monitor that themselves with a pulse oximeter. $20-30 in the US.
I seem to remember reading that initially they used O2 saturation to see if people should go on ventilators and many people with low O2 were not struggling to breathe. Now they avoid ventilators except as a last resort. So, even O2 saturation is not as clear as once thought. I also read that some of this is similar to high altitude issues but have not delved into it that deeply.
Alternatively, keep monitoring how long you can hold your breathe for. If it stays the same you have not contracted a significant lung infection. Actually, if you keep testing it, the exercise will make it increase somewhat, but it is still informative.
Salute!
Hey! Oxygen saturation might be O.K. for folks with “normal” lungs/bronchial systems, but is not a good criteria for folks like me with modertate COPD and with only about 2/3 to 3/4 of my “original equipment”, heh heh.
I can easily get saturation above 94% ( recommended FAA night figure for pilot supplemental oxygen – those guys up in row 1, seat 1 and 2 of your plane). Special breathing and not moving about quickly I can even get to 92% siting on a deck at 8,000 feet MSL. But there’s a rub. Being borderline anemic I need more red blood cells to carry that saturated oxygen where it needs to go. Which means any increased demand has other effects like very high pulse rates. I have no other problems of any kind that seem to influence mortality with this critter. Can pass an astronaut physical except for the COPD.
Sorry for the war story, but the doctors need to look at the whole picture, and ventilators are not the only last ditch maneuver for a significant number of we old codgers.
I and millions other took the HCH and its brothers and sisters during our tours in SEA plus other places, and Willis can also testify about his “debilitating effects” of ingesting that terrible concoction, LOL. You do not see thousands and thousands of we vets falling down on the street except for factors not directly related to the malaria prophylactic. And where are the millions exposed to the mosquito and not given the HCL for a “blind” clinical trial test? Huh? Ditto for the lupus patients these last forty or fifty years.
Cardinal rule for too many folks in media and even biological science is to deny or make light of anything “orange man bad” says or suggests. And the climate blog we are on here has many examples of what happens when you go against the “settled science”.
Gums whines…
Salute!
Oxygen saturation is a poor metric for anyone with existing lung problems. Ditto for “beong short of breath”. Just ask anyone with COPD or similar condition.
Gums sends…
P.S> Previous post RE: this apparently mod removed/withheld
And that brings up the recommended use of masks as a deterrent for covid-19, since oxygen saturation is the key metric!
Get a pulse oximeter, test yourself, then wear a mask in the prescribed way and watch your oxygen saturation drop!
I’m so glad they have made masks politically essential and all those fancy designs a marvelous fashion statement!
I sure hope HCQ works and the FDA immediately evaluates this study and makes any necessary recommendations.
Months ago many on this site said HCQ needed to be given early with the z pack. Waiting too long may not work. The French doctor that claimed success gave it Early.
The other studies were studying people that got treatment late in disease which is not what French doctor was doing.
I would like to see above study repeated but also add zinc. Death rate hopefully is cut further. And get any decision makers with pharmaceutical ties out of the way. Too much conflict of interest.
Agree with Stevek. As I recall, progression of Covid-19 is nose and throat, often w/o obvious symptoms. As an elevated temperature is displayed, the viral load has already started to mushroom out of control. This is when plasma Vitamin C drops, and probably any free tissue zinc is depleted.
I’ll mention again. You are probably a lot better off laying on the hot, dry sand at the beach than taking the virus back to an air-conditioned space with insufficient makeup air. Above all, avoid staying at home or in nursing homes and restaurants where the virus, at low levels, is recirculated over and over unless ASHRAE’s air change-out rates are greatly exceeded.
As usual, Authority may not be our friend.
Ask and ye shall receive:
https://www.preprints.org/manuscript/202007.0025/v1
Ok, sorry.
The group with HCQ only has a median age of 53y where the control group with no treatment has a median age of 71y.
There is this interesting COVID-19 age calculator:
https://profile.covid-age.com/calculator
Just checking with the exact same other parameters gives of course very different results for 53y vs 71y.
The median age is a too big confounding factor to draw any meaningful conclusions from this study. The jury on HCQ is still open.
exactly…
median 71….nothing…the oldest group
median 53….HCQ…the youngest group
70 and up is the group most at risk
See my comment above
No, you are wrong. Age and other factors were controlled for in the regression model:
Multivariable Cox regression models and Kaplan-Meier survival curves were used to compare survival among treatment groups while controlling for demographics (e.g., age, gender), preexisting medical conditions (e.g. CVD, lung disease) and clinical disease severity (mSOFA, O2 saturation).
The results of the regression with factors like age taken into account were that HCQ reduced mortality by 66% and HCQ+Zithro reduced it by 71%
In the multivariable Cox regression model of mortality using the group receiving neither hydroxychloroquine or azithromycin as the reference, treatment with hydroxychloroquine alone decreased the mortality hazard ratio by 66% (p<0.001), and hydroxychloroquine+azithromycin decreased the mortality hazard ratio by 71% (p<0.001).
However, if you get Covid19, you are perfectly within your rights to decline treatment with HCQ. Please do not deny me my right to use that treatment, since it is my body and my life. Thank you.
There are some bizarre features in that Cox regression. Firstly their allowance for age, which is just 2 level (HR 2.6 for age >65). But the differences were very large, and 2.6 doesn’t cover it. Then they allow HR of 1.7 for being white. In most analyses, being non-white increases the HR. I wonder if they just got it reversed.
But again, the outcome is just strange. On the face of it, being in the much younger group gave an HR of 0.51. Allowing for age should increase this. But instead, the HR diminished to 0.34. The comorbidities far outweighed the effect of age. But why would the much younger group have so much greater comorbidity?
Why would a younger group end up in the hospital? Kinda seems like that’s a hint.
Could be the demographics of where the hospital sits. The hospital sits in Dearborn Michigan, the largest Shiite Muslim community in North America. The population is young and not assimilated to the American culture. There are multiple families living in many single family dwellings. There are not many old people in that area. The strain they got was probably the deadly strain from Iran with little mutation. That was a very hard hit area early on.
@Mike
Doesn’t it depends what you can draw out of a Cox regression on your grouping and your null hypothesis?
I really would like to see a grouping based on patients receiving steroids vs no steroids with the same data set. Cause that is 71% for HCQ and only 36% for control.
This is good news. But this study did not use zinc with hydroxychloroquine. One theory says that zinc interferes with the virus’ ability to replicate in our cells. But zinc does not easily get through the cell wall. Hydroxychloroquine increases the permeability and aids in getting the zinc into the cell. At least that’s the theory. It would be interesting to test that theory.
Zinc is readily available in red meat, chocolate, oysters, crab, nuts etc. Bloodwork is routine in hospitals and deficiencies are ameliorated with a pill. I imagine the majority of North Americans have ample zinc. An 8 oz serving of beef gives 100% Daily Value, 4 oz of chocolate 33%. Shellfish, crab, dairy….
…that’s a lot of chocolate! The large Hershey’s bar only contains 6.8 ounces! You’d have to eat almost two of those big bars to get 100% of your zinc!
Jeff
Thanks for reviewing a serious study. .
Now see Zelenko’s preprint just posted on his Zelenko Protocol of rapid early treatment with Hydroxychloroquine, Azithromycin and including Zinc. Note 84% reduction in hospitalization. Only 1 death in 141 treated patients.
Scholz, M.; Derwand, R.; Zelenko, V. COVID-19 Outpatients; Early Risk-Stratified Treatment with Zinc Plus Low Dose Hydroxychloroquine and Azithromycin: A Retrospective Case Series Study. Preprints 2020, 2020070025 (doi: 10.20944/preprints202007.0025.v1). PDF
Abstract
I wonder if the LANCET will publish this study after their last retraction.
No, their damage has been done–water under the bridge, bodies in the grave!
How much responsibility do the media and rabid democrats have for a significant number of deaths incurred due to covid 19 by fighting against the use of HCQ; which is now found to be of benefit?
It seems to me that the media and Trump hating Democrats (but I repeat myself) should be held responsible for promoting their own ideology rather than questioning the results of prior studies that turned out to be as poor as most climate studies.
People died.
+10
CDC: total Excess Deaths now negative – Total deaths now BELOW average
See Excess Deaths
Interesting link. Perhaps the mortality has gone below average because those who died early in the pandemic (mostly in nursing homes) were going to die within weeks or months of other causes. If they passed in the pandemic, the mortality numbers post-pandemic would be expected to be below the average for the date as some part of the expected current mortality occurred a few weeks early . . .
“CDC: total Excess Deaths now negative”
That’s to be expected, because the lock-down has cut deaths from flu and auto accidents, and workplace accidents.
And elective surgeries sometimes have very negative outcomes. They have bern postponed, as well.
Evidently covid19 or maybe relentless global warming agenda science causes critical thinking to drop like a rock. Hcq was always a candidate for early stage use not in near death stage. So we finally got a study result for that early stage. Duh
Follow the link in the title above above, then click on the PDF of the prepublication proof to the right. It gives the full paper.
https://c19study.com/
The studies that have negative results all have the phrase “late stage trial” which is KNOWN to fail. Why are they subjecting people to a course of action they know will fail?
Some of us with years of experience and only trivial side effects from chloroquine thought this was bleedin’ obvious and it turned out we were right. If chloroquine was NOT taken before the onset of malaria, administer within the first two days of symptoms. IF chloroquine WAS being taken, then the malaria was a chloroquine-resistant type, so an alternative was needed. And chloroquine CAN work against other viruses, AND things that are not virus-based.
Unfortunately, there has always been a gap between what is good practice in tropical medicine and what is done in temperate climates. Don’t succumb to malaria if you are going to a temperate or non-malarial country. They will be all over you, but won’t have any idea what to do. Same with any thing like infected wounds, tropical ulcers etc. In the tropics you use grease-free topical treatments, eg paints, not the greasy gunk that is the basis of most topical treatments in temperate places.
Up here in the north of Australia, every year, we used to get know-nothings from down south coming tell us about climate-responsive design. Most of it completely wrong, would make buildings hotter not cooler. The only thing they got right was don’t come up when the heat/humidity problem is at its most severe and it’s cyclone season.
Remember that the remdesivir trial had one set of endpoints, then changed the endpoints part-way through, then ended the study early because of the marked improvement of the new endpoint for time to discharge, and found that you need to treat 30 patients to change the medical outcome of one person.
Oh, and they’re charging thousands of dollars per patient. Can’t forget that detail, since it explains all the rest.
Gilead’s drug will cost $3,100 per course, but it is always emphasized somewhere in the spiel that the insurance will pay for it. So people don’t have to worry about the cost.
A shared responsibility — out of sight and out of mind — construct to obfuscate price and effectiveness.
And Fauci is directly connected to the drug
Bob,
Evidence?
Saying over and over is not evidence.
Remdesivir shortens the time to disease resolution by some 5 days.
At over $10,000/day for hospitalization, it is a bargain.
And it is free in clinical trials.
Are you against people selling things for money that they invented?
Ever wonder why most useful drugs are invented by U.S. companies operating in a for profit basis?
The price is $230 to $310 per dose.
It may only take 5 days(6 doses) to work.
But no one is forcing anyone to pay to get well faster.
Anyone is free to spend the money and stay sick as long as they wish to stay sick.
…or take NHCQ + Zn for $50 with minimal side effects! Again, your choice!
Let’s consider Tamiflu. It only works if you take it within 48 hours of symptom appearing. It just lessens the severity of the flu and shortens the duration by only 1-2 days. It carries side effects especially in younger people, it should not be given to those with underling conditions concerning heart and kidney health. Yet it is prescribed without a blink of an eye.
HCQ seems to act in a similar way in that it must be taken early on and it lessens the severity and shortens the duration of COVID. It has side effects but all drugs do so certain people shouldn’t take it. So what’s the real problem? Is the cost too low? Does Gilead have a hand in this? Makes you want to go Hmmmmm?
Follow the money.
Tamiflu also creates influenza resistance AKA “super” flu.
I wonder how much Gilead stock some of these politicians have acquired since this started. Nice to be able to pressure a cheap competing drug out of the way as the top Democrat voices have done over the last 3 months.
Turkey still gives HCQ+ to every infected patient. Right from the beginning the ratio of recovered cases versus active was one of the best in the world. Turkey has had a significant number of cases over time. So they should have the largest data base for HCQ usage/corona virus in the world. That data would be interesting to look at.
Also India, who are a big manufacturer of HCQ, have authorised its use and have a death rate of only 13/million population compared to 658/million in TDS afflicted UK.
https://www.statista.com/statistics/1104709/coronavirus-deaths-worldwide-per-million-inhabitants/
All very suspect why those trying to develop a vaccine dismiss hydroxychloroquine. The Zinc component also omitted to reduce the reported efficacy- also very suspicious. You would think that if they were genuinely looking at curing COVID, they would not be going out of their way to discredit something that works.
Please explain why certain vested interests are trying so hard to dismiss a cheap, safe and simple cure.
From comments on JoNova’s site in earlier threads, I gather that there are any HCQ studies in the pipeline, and that some of them are looking good. So I’m optimistic we’ll be able to rub the noses of disgraceful media like WaPo in their poop. And disgraceful scientists like Dr. Bright, an erstwhile FDA bigshot who clamped down on HCQ use early on.