By Christopher Monckton of Brenchley
It’s déjà vu all over again, and, frankly, nostalgia ain’t what it used to be. On the climate question, the totalitarians told us we must believe, just believe the experts. As a hard-headed British engineer once defined it: “Expert: x, an unknown quantity; spurt, a drip under pressure.” On the Chinese virus, we are told the same.
Pity the governments that have had to attempt to take rational decisions on what to do about the Chinese virus when, as with climate change, the data are inadequate and incompetently kept, the world body nominally in charge is inept, corrupt and – to put it mildly – deferential to totalitarian regimes, and the soi-disant “experts” cannot agree among themselves.
In Britain, it does not help that the Prime Minister, on five occasions at the beginning of this year, failed to prioritize his time in such a way as to take the trouble to attend and chair the weekly intelligence meeting held in Cabinet Office Briefing Room A.
It is these meetings that are intended to be the gathering-place for information garnered by Britain’s various intelligence services around the world, under the aegis of the Prime Minister and the Chief of the Joint Intelligence Committee. Had Mr Johnson attended those meetings, he would perhaps have intervened to do something about the then-alarming daily case-growth rate at least a month earlier than he did.
As it was, he dithered until two weeks after Mr Trump – who was himself late in acting – declared a national emergency. The consequences are now becoming all too apparent. It is possible that Britain has now lost more of her citizens to the Chinese virus than any other country except the United States and China. We don’t know for sure, because a third of all British deaths arise outside hospitals and are thus ingeniously excluded from the Government’s daily counts, though the Office for National Statistics is now publishing a weekly parallel series giving the real numbers.
Among the truly half-witted advice given by the “experts” are three points that deserve urgent correction. Neil Ferguson, the epidemiologist whose model HM Government chiefly heeds, said yesterday that large gatherings are not particularly important for transmitting the virus. On this point, the South Koreans would beg to differ. Their elaborate and determined contact-tracing has shown that the infection first got its boots on at a large church assembly, to whose members many of the first cases in South Korea were traced back.
Secondly, most Western governments, with less recent experience of fatal infections than those in the Far East, have still not quite learned the importance of asking their citizens, when outside their own homes, to wear some form of face-covering.
As South Korea’s chief of public health has bluntly said in a recent interview, homemade face-masks are by no means perfect, but they help a great deal by preventing droplets from coughs and sneezes from traveling well beyond the 6 ft that most countries have adopted as the minimum “social distance”. Even with masks, 16 ft would be better than 6 ft. Without masks, 6 ft is a dangerously inadequate distance.
Mr Trump, in his three-phase plan for bringing the lockdown to an end as soon as it is safe, has gotten the point about do-it-yourself face-coverings. His plan strongly recommends them. HM Government, however, continues to dither on this as on much else. Unlike Mr Trump, it has proven wholly unable of even giving a hint of what an exit strategy from the lockdown might look like, and people are becoming justifiably alarmed that their elected representatives do not trust them.
The worst of all the pieces of bad advice handed down by the “experts” is the idea that the best way to deal with this pandemic is to let as many people as possible get the infection and acquire what they chillingly call “herd immunity”.
As the South Koreans have discovered, it is far from clear for how long the immunity acquired by those who have recovered from the infection will persist. Until that central question is answered, it cannot be safely assumed that population-wide immunity will be rapidly or effectively acquired.
Here are today’s graphs showing the daily compound growth rates in cumulative confirmed cases and in deaths. As always, they are seven-day averages, so as to iron out random fluctuations in the data. Note that it is cumulative cases, and not just new cases, that determine the future rate of transmission.

Fig. 1. Mean compound daily growth rates in cumulative confirmed cases of COVID-19 for the world excluding China (red) and for several individual nations averaged over the successive seven-day periods ending on all dates from March 28 to April 18, 2020.

Fig. 2. Mean compound daily growth rates in cumulative COVID-19 deaths for the world excluding China (red) and for several individual nations averaged over the successive seven-day periods ending on all dates from April 4 to April 18, 2020.#
Ø High-quality images of the graphs are here.
Having had personal experience of the British NHS, I would say that the most likely cause of the large loss of life to Covid-19 in Britain was mainly due to the appalling standard of medical treatment handed out under the NHS. The consequences are all too apparent.
Australia: pop.25M 6,618 cases, 4,230 recoveries, 71 deaths (20 off 1 Cruise Ship in harbour.)
United Kingdom: pop. 66M 120,067 cases, N/A recoveries(?), 16,060 deaths.
I suspect it has more to do with 7x the infection rate in the UK. This has more to do with geographic location, population density, and forcing of quarantine for entrants as well as refusing entrance to non-citizens that we practised in Oz.
The NHS isn’t great, but it’s not as bad as you make out.
Yes it is. I have had my father die due to poor care and negligence in one of the major London hospitals. One sister that had to get a second opinion from a privat doctor who confirmed that her thyroid had died which would have killed her as well. I arrived in the accident and emergency with a broken arm at 5am and had to wait until 8:30 to see a doctor but there was no-one there, they were just too lazy to do the job they were paid for.
The NHS is a total joke and money pit.
But if you talk to any staff they think you should treat them like a god
I absolutely agree. Having lived much of my life in other countries, I find the NHS bureaucracy mind-blowingly incompetent. I’m sure the medical professionals are as well-trained as in other countries, but they are hampered by an antiquated admin system, which they all seem to accept as being completely normal.
And to criticise the system is seen as being heretical – especially now.
Yes, allowing plane loads of people to come into Britain including from hot spots like Italy and Spain, with no separation in airport cues, no testing – not even an IR thermometer on the forehead- , no quarantine measures was criminally irresponsible. No wonder UK is in such a mess.
CogB
Not true. Once victims have recovered they are not longer contagious. Cumulative totals are everyone who was ever ill, not those currently ill and contagious.
Once again our nodding Homer demonstrates he has no understanding of what these figures mean or how to draw conclusions form them.
In response to the relentlessly negative “Greg”, it would indeed be useful to subtract recoveries as well as deaths from the cumulative cases, but most countries are reporting them inadequately, and the ever-more-incompoetent British Government is not reporting them at all. Therefore, the best we can do is report the cumulative cases (which are in any event a considerable understatement). This has already been discussed in these columns.
So once again you have to walk back your claims.
When challenged this becomes:
Not the same thing , is it. You should have said that initially if you want to make that case.
I have already agreed with you that not counting those cured and discharged is a dereliction of duty.
Daily cases, ie rate of change gives an earlier indication of the evolution of the epidemic that the rather smooth rise of a cumulative total.
A further differentiation clearly shows the break from a typical epidemic evolution 10d after confinement came in in Italy. Maybe by the end of the week we will have the first indication of any changes due to slackening restrictions.
Yes, I have been consistently negative about your lame attempts and false and erroneous claims about what your graphs show.
Rather than just criticising, I have produced a method which does do what you failed to do. I regard that as a positive contribution for the rest of the world, whether it pleases you or not.
“A further differentiation clearly shows the break from a typical epidemic evolution 10d after confinement came in in Italy.”
there is no typical or “control case” for an epidemic.
if you have a historical example where people did nothing in response to an epidemic you might have a control to talk about.
The “attribution logic” folks are using here ( both pro and anti lockdown ) is not very convincing
Some professionals are however getting on the ball and looking at actual mobility data.
In response to the relentlessly uniformed and inaccurate “Greg”, whether he likes it or not it is the cumulative cases, and not only the new cases, that determine the rate of transmission. Where possible, one should deduct the closed cases, but governments are not counting the closed cases correctly. The data are inadequate. Get over it.
The UK data is a mess, which is why I don’t even bother plotting it. But now you jump from there to make the sweeping assertion “governments” in general are not counting closed cases correctly. Convenient, unsubstantiated waffle.
All these data have issues. That is not a reason to throw our hands in the air not analyse any of it.
You naive graphs tell us nothing useful and can not even tell us if we have passed the peak in new infection. You keep regurgitating the same nonsense day after days without admitting your cannot even interpret what you are presenting. You goofed, get over it.
Thanks for the input Mosh.
I have used a very simple model but that is only to detect the break point where we can probably say we are detecting the effects of confinement. There is a large uncertainty in the model fit and how it behaves beyond the break point should not be given any weight at all. Certainly not in terms of peak value, timing of peak of timing of zero crossing etc. The purpose is just to show the form of the curve.
It would not make any difference it I used a Gompertz , SIR, SEIR or other model.
So the control is only a control in the most general terms. The break point is clear enough that we don’t need to be concerned with the exact model used.
Maybe I will grey-out the latter part so that no one thinks I’m suggesting that model is supposed to be an accurate representation of “expected” later development , other than showing general form.
I’m currently trying to extract a weekly “climatology” from the post confinement segment to tack on the end as a predictive model of the coming week. This may serve as a visual reference for any deviation due to relaxing confinement.
We can probably expect a move above constant new case line after about a 10d lag from relaxation. That will be starting from Fri or Sat this week.
Since the second differential is quite sensitive to change this is probably the kind of analysis which will detect it first.
I’m rather surprised how consistent this weekly cycle is in the Italian data. I guess they have the dubious advantage of large numbers to average out random variability.
Spain is very similar , though it has a week less of confinement. UK data is not even worth plotting. US is too heterogeneous: many different epidemic populations all being put in the blender. Maybe isolating NYC could work for a similar analysis.
I’m hoping that Italy, having served as the West’s crash test dummy, can reveal some information ahead of time for other countries, like UK and US which are a little later in their respective epidemic evolutions.
cheers.
“Yes, allowing plane loads of people to come into USA including from hot spots like Italy and Spain, with no separation in airport cues, no testing – not even an IR thermometer on the forehead- , no quarantine measures was criminally irresponsible. No wonder USA is in such a mess.”
simple facts.
The data was uncertain and will remain uncertain
The public was told this was some kind of flu
Experts are attacked right and left.
Politicians make dumb mistakes.
Go figure.
thankfully we will not suffer from mistakes you would have made.
or from mistakes I would have made.
We’ve got a lot of Monday morning quarterbacks and it’s not even halftime yet.
It’s easy to be wise after the event but it does not take career in epidemiology to work out you should be controlling people coming into the country and at least doing the most cursory scan for fever. Other counties were already doing this , they did not even need to have the idea themselves.
No social distances at passport control. WTF?
My mother had a flight out of London in March. After seeing what was happening at UK airports she skipped to flight ( despite having a very important reason for flying ).
Now with most of the country under confinement they are shipping thousands of Romanians and east europeans to under-cut the UK labour market, with equal disrespect for health checks.
No social distances at passport control. WTF?
It’s OK, Greg, we’re not allowed to go to the garden centre to buy some petunias. That’ll more than compensate. Thank the Lord for lockdowns!
Today, government failure is often perversely rewarded. Budgets are increased, more staff it hired, etc. Problems and crises are viewed as opportunities, not to be solved but to be used to acquire power.
@Mosh — Finally a comment without snark. I concur.
As to whether Greg’s or your would make bigger or worse mistake than the experts, we’ll never know because the public has had no real policy debate. Our media fuels fear and deliberately paints Trump in the worst light, while heaping praise upon the experts he is following,
I think the United States has a long history of starting slowly and fitfully, but eventually kicking it into high gear. Picture Usain Bolt getting out of the blocks late, then blowing past everyone halfway through the race and you’ll have an idea of what I mean.
The UK does not have a large loss of life. On a population basis we are lower than Belgium, Spain, Italy and France. We are similar to the Netherlands. Germany counts deaths entirely differently, but we may not be much worse than them. So for large European countries we are relatively OK.
Yes, in a consistent and defined manner. This is quite different to the anarchic, piecemeal mess in the UK.
Your point may be relevant though – if you explained it rather than making unfounded assertions.
Could you explain the difference in counting and how this ends up with Germany’s figures which look WAY better begin about the same as UK?
thanks.
Germany doesn’t test the dead. There, if you die of pneumonia without a prior COVID diagnosis, you don’t count as a victim of the CPC. In the US, if you die in a car wreck, but then test positive for the WuWHOFlu virus, you are such a victim.
Dunno if the U.K. has such a standard or not.
My sister is an RN and she is amazed how we are skewing the data. If someone dies from a heart attack but has the flu, we don’t count those as flu deaths. If we applied the CDC’s recommendations for counting Covid-19 deaths to the common cold, how many cold deaths would be have?
I believe this overcounting issue is deliberate. The more official deaths, the more money goes to the bureaucracy, the states and to the hospitals.
It has the US standard. No numbers mean anything in the UK, the only stats that can be used that have any foundation in fact are the total morbidity numbers reported by Euro Momo. They show 3 things. Firstly the all age excess deaths acoss Europe ( and the UK) have the same amplitude, duration and shape as the flu deaths of 2018. Secondly Sweden and the UK, France, Itlay, Spain have exactly the same excess amplitudes, durations etc, ie lockdown makes no difference at all. Thirdly the seasonal flu excess deaths in the winter of 2019/20 didn’t happen, they were waiting for CV-19 , so died 4 months later than usual.
And finally the excess death trend is sharply DOWN , all acoss Europe.
So even if all countries have different reporting methods, overall they cumulate to show its no worse in aggregate than flu in 2018 and its almost over.
Can we have our lives back now, pretty please?
Spot on John. And to jeffery P’s point.
The Government has put the economy into a controlled dive without assurances they can pull up in time.
In the final analysis, it will be more about Media, Political and Bureaucratic CYA for killing the economy. The redistribution of federal dollars (read debt) is simply extortion to buy “Big Medicine” i.e the Healthcare Establishment’s cooperation with the Central Authoritarians, who are resting comfortably in their mansions eating gourmet ice cream and don’t want the great unwashed masses to storm their castle when this is all over because they no longer have jobs.
This is the primary reason why they need to pump the numbers up. Even with dummie numbers they still are having difficulty making this look like it will end up being any worse than a bad flu season.
How to read the tea leaves. We have years of data and a relatively stable death rate. If total deaths don’t spike dramatically and flu and pneumonia deaths all but disappear or fall off a cliff during this period of Corona then you will know the fish is rotting at the head. But then some of us have known that for years.
The inflammation that is caused by ChiCom19 has been shown to cause blood clots which have caused heart attacks in ChiCom19 patients.
We don’t really need to test for the virus though. Just look at the overall mortality each week and the number above the average is likely to be caused by covid-19 unless you can think of a different major cause. The UK as just released data (ONS) for the week ending 10th April and there were 8000 above average deaths, compared to 6000 the prior week. Hopefully we are at the peak now.
“Main points from latest release
The provisional number of deaths registered in England and Wales in the week ending 10 April 2020 (Week 15) was 18,516; this represents an increase of 2,129 deaths registered compared with the previous week (Week 14), is 7,996 deaths more than the five-year average and is the highest weekly total since Week 1 in 2000.
Of the deaths registered in Week 15, 6,213 mentioned “novel coronavirus (COVID-19)”, which is 33.6% of all deaths; this compares with 3,475 (21.2% of all deaths) in Week 14.”
https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/weeklyprovisionalfiguresondeathsregisteredinenglandandwales
In response to John Tillman and Jim W, it is already clear from the EUROMOMO statistics that there is severe excess mortality in several countries, including the UK, whose own excess mortality statistics for weeks 14 and 15 show so sharp a spike in excess mortality that they have caught the professor of statistics at Cambridge by surprise.
Once again , Mr Monckton, is unable to produce any numbers relating to the deaths “with’ or “of” Corona.
So a good idea of a petri dish is the French Aircraft carrier where those on board would have been in very close proximity.
Sorry for the repeat- but I feel we have had enough of the lock down was necessary.
“On a French aircraft carrier 1081 soldiers tested positive. So far, almost 50% of them remained symptom-free and about 50% showed mild symptoms. 24 soldiers were hospitalized, one of them is in intensive care (previous illnesses unknown).
In response to Phoenix44, one must adjust for the date on which the first cases were recorded. On that basis, Britain is a couple of weeks behind Italy or Spain, so our numbers will, alas, rise over the coming weeks.
The date the first cases were recorded is unlikely to be the date the first cases arrived.
Yes, I’d say the first cases in Europe probably arrived two or maybe even three months before the first “confirmed” cases. The virus seems to need quite a bit of effort to get into the immune system. So those who get it early, while it’s still at a relatively low level among the population, tend to get mild symptoms. Later, when more people around you have it, you’re at more risk. That might also explain why (political lies notwithstanding) the Chinese got caught with their pants down.
Mr Lock is guessing how long before confirmed cases the first infections arrived in Europe. Since the earliest cases in Wuhan date from mid-November 2019, and the first confirmed cases arrived in Europe in mid-January 2020, it is not plausible to imagine that there were infections in Europe in mid-October 2019, three months before the firstr confirmed cases and – ridiculously – one month before patient zero in Wuhan.
farmerbraun thinks it entirely plausible that travel originating around Wuhan from November onwards could have gone to any country in the world, bringing a virus along for the trip. It’s what virus does.
It would then follow that isolated cases were present in many areas of the world from about December; this does not seem implausible.
Christopher, you have missed my point, and Neillusion’s point too. The first internationally reported cases from China may have been in November. But were those the first confirmed cases? I don’t know, and neither do you. And when were the first actual cases? Even the Chinese don’t know that.
You are skeptical of the case data from the UK, are you not? And rightly so. So why are you not at least as skeptical of what the Chinese have said?
I don’t think our weekly numbers will rise now. 8000 above average deaths from 3rd to the 10th April following on from 6000 the week before is hopefully our peak. I would expect no more than 8000 the following a week and then a decline from this point, but we will have to wait and see.
Data from the weekly posted ONS stats.
You cannot compare death rates across nations without
stratification for age and co morbidity
just STOP comparing national rates until you have the data properly stratified
Hint, you will need cross tabs of comorbidities, age, and standard of care applied.
THEN you might begin an analysis
Steven
Why can’t this be done in real time.
Individuals such as nick stokes and Clive best are able to run WORLD temp anomalies with fancy graphs in a couple of days after the end of the month.
How comes nations states under an unprecedented disaster can’t collate death certificate data?
‘Why can’t this be done in real time.
Individuals such as nick stokes and Clive best are able to run WORLD temp anomalies with fancy graphs in a couple of days after the end of the month.
How comes nations states under an unprecedented disaster can’t collate death certificate data?”
reporting systems of various countries are not UNIFORM
what data is collected
what data is publishable,
what codes are used
etc.
and it takes time.
One example from Korea. A 17 year kid died. required an autopsy,
then several rounds of review by various government agencies
then an outside review.
verdict? not covid
Additionally in uk the attending dr is supposed to sign the cause of death.
The attending dr is the dr who is supposed to know the full history of the patient.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/877302/guidance-for-doctors-completing-medical-certificates-of-cause-of-death-covid-19.pdf
By now these doctors should know that the importance of filling out the certificate correctly wrt to the nations health and economy.
Do these morbid numbers even exist?
Steven
I thought they were UNIFORM. AFAIK Korea, Italy, uk and others all use the same international ICD Code for reporting cause of death
https://www.abs.gov.au/ausstats/abs@ur momisugly.nsf/0/47E19CA15036B04BCA2577570014668B?
See Australia’s example.
The IMHE have experience combining and comparing this data for countries.
Yes I agree it will take time to compile all data, but if analysing even 80% yielded a pattern. Say disease x sufferers were more prone to COVID and this was evident in multiple countries then this info would be invaluable.
I’m just thinking how a team like BEST or individual like Clive BEst or Nick Stokes can compile temp data from all over the world why similar teams in a national emergency can’t.
” it is far from clear for how long the immunity acquired by those who have recovered from the infection will persist. Until that central question is answered,”
Why, suddenly, are they pretending that the antibodies created by overcoming a viral attack are essentially transient? I have never heard of such a thing and evolution indicates that our immune system would have a longer memory to prevent a re-infection immediately after a successful repulse of a virus. Those who do not have any residual immunity at some level would not survive.
It appears that the”experts” are seriously interested in pretending we know nothing about viruses, disease, and our immune system, which then means that everything is possible. What fun.
At this point, there is cogent evidence that the C-19 that has been observed is very likely exosomes given off by our tissues in response to a number of stimuli or challenges. So, the tests are testing for a response to a challenge, not the virus causing the illness. As there are many reasons that we make exosomes, which contain RNA, the existing tests only measure for something many of us have for a variety of reasons —this also explains the high number of positive tests in asymptomatic people.
This brings into question what an antibody test will test for. If you have antibodies against your own exosomes, you have an auto-immune condition, which is not good. There is a chance that they might accidentally focus on antibodies for the actual virus that is making people ill. One can only hope.
As the flu season is a salad of viruses, we simply do not have the ability to sort out all the viruses a person might have at one time and, instead, have been focusing on the RNA from a symptom of the viral challenge or even stress challenge, which can indeed cause exosome generation.
In response to Mr Higley, nobody is “pretending” that immunity to the Chinese virus may be short-lived. Some 19 cases in South Korea have cleared the infection and have subsequently been re-infected. This is unusual. If this result is replicated more widely, then it will simply not be possible for us to assume that “herd immunity” will ever be acquired.
More precisely, “Some 19 cases in South Korea have been tested as cleared of the infection and have subsequently been re-infected.”
South Korea has done a fantastic job of testing, tracing and isolating victims. They have managed to stop the spread of the virus. But they have only done that by testing 100s of 1000s of people.
How many false positive test results would one expect from that many tests? More than zero , surely. Maybe as many as 19.
We do not yet know that the virus mutates quick enough to re-infect people within a few months.
I am afraid 19 is not the correct number, it is 163.
https://edition.cnn.com/2020/04/17/health/south-korea-coronavirus-retesting-positive-intl-hnk/index.html
While I’m sympathetic about your experience with the NHS, I think that this is one instance where it’s not their fault. I put the blame on dithering politicians and obstructive public servants. Oops. Sorry. “Civil Servants”.
My father died in an NHS hospital in 2014. He was only 90. The responsible doctor seemed to be very competent, but he was hugely overloaded and only had 3 or 4 minutes to explain to my brothers and me that our father was probably not going to survive beyond a day or two. He wasn’t responding to their treatment plan. I wonder how much time the doctor had to examine my father again, and review the original treatment plan?
According to graphs and data published in UK press about 95k people have had an outcome. Cases – (deaths+currently hospitalised) to give recovered cases. Data on numbers in hospital in UK can be found on the internet
That gives a survive/death ratio of 85/15. So the death rate of all cases including those unreported will be considerably lower.
Having a NHS that has been under funded for decades and having the most vulnerable closeted together in homes seems an ideal way of getting the maximum death toll.
“Having a NHS that has been under funded for decades” that statement is utter crap. The NHS in the UK was fed huge quantities of money during Blair’s administration, and that only ended in 2010. Since then the NHS has had no real cuts, simply the growth in funding has slowed. This followed from the financial crisis of 2008 presided over by the then Labour goverment. We continue to pour money into it despite its dreadful bureaucracy.
The winter crisis in the NHS now stretches form October to March even without novel viruses. The underfunding of the NHS is not a theoretical discussion point. It’s a fact of life… and death.
The financial crisis of 2008, US sub-prime mortgage mis-selling and the collapse of Lehmann brothers were not caused by the Labour Party.
The economic incompetence of austerity when interest rates were low and investment was desperately needed was the fault of Lib Dem and Tory Governments. A fault that is killing people today.
The large loss of life is likely due to patients who were misdiagnosed and intubated with high PEEP. Most covid patients need high oxygen, not high PEEP that can irreparably damage lungs with normal compliance, as most covid patients have.
High oxygen is helpful by adding hydrogen is going to address the problem at its root. High O2 is a compensation, not a treatment. The observation that it is chemical pneumonia not viral pneumonia is significant.
I concur with you South Korea has fought the battle fearless even our country Kenya. Am over 40 and for the first time in my life I have missed to attend the church becoz the govt banned all social gatherings. Hotels are take aways, all schools closed and lock downs by counties. Curfew Nationwide from 7pm.
Last week a Maasai was recorded whipping people with a rod saying the govt ordered you keep two metres distance.
Hand washing in every shop and masks are compulsory yet others wonder why Africa is winning low infections. That’s why it’s not about rights, freedom it’s about discipline by which means necessary. Corona is an ass and must be defeated through all means necessary.
While you’re at it, ban driving, sailing, skiing, and all contact sports. We can’t have any injuries or death, can we? Then we’ll all live forever!
What about bathtubs? Bathtubs are the number one killer in households. Should have been outlawed ages ago.
Just the other day a friend mentioned his doctor was treating him for corona virus. Told him to take a large irish whiskey after a hot bath. I asked how he liked the whiskey, but he said he was still working on the hot bath.
Is it the bathtub or the electric hairdryer which is the actual cause of death ?
Death because of a bathtub or death with a bathtub?
😉
We shall also ban dihydrogen monoxide as it k!11 lot of people by making irreparable damage to the lung. This poison is known to contaminate practically all domestic water taps!
Venice Beach, CA did the reich thing (sieg heil!) and filled in a beachfront skateboarding park with sand so that impertinent youth couldn’t use it. Seriously.
https://twitter.com/bennyjohnson/status/1251647382057553927
Long live the youth!
https://twitter.com/JoeySalads/status/1252101549355986945
https://twitter.com/JoeySalads/status/1252101876272656384
What a bunch of brainless jerks. Like you spoil one spot for skating and everyone goes home and self-isolates as a result? WTF are they thinking.
This is almost as good a Bedfordshire pigs dumping black dye in a beauty spot to stop people going there.
That level of stupidity should be a criminal offense.
The beauty spot is notorious for drownings (google map ref: 51.99440002,-0.25799110)
People (usually the young) go swimming in it, not realising that it is quite deep, and very cold, and hence get into trouble. Probably they (police) are fed-up with pulling dead bodies out of it…
Why are the bulk of the British workforce confined to home (barracks, prison)? Why have billions of pounds been allocated to help those confined? Because government edicts powered by xspurts ignored the reality of the demographics that said that this very workforce were at a very low risk of any serious consequences from the virus, and, went ahead and hobbled the wheels of the economy. The billions helicoptered into the economic crisis of their own making could have been directed to ensure that the most vulnerable in society were properly protected and that alternate locations to treat virus victims could have been properly equipped to avoid burying hospitals already at their limits. In addition, money could be spent now to help define detailed requirements for the nation’s plan for the next epidemic; nothing like a real time exercise to help get it right because the next pandemic may be far more lethal.
I fully agree with this, and the results could have benefited the vast majority of us for decades.
Having said that, I’m very glad I didn’t have to make the decision and have the possibility of a massive death toll on my hands. 2020 hindsight (see what I did there?) is nice to have, but they did not have that luxury when making decisions. I think we should reassess and reconsider now, however.
That is phase 1 of the trump plan. Send the hwalrgt back to work and the vulnerable shelter in place. The obvious solution.
We were told the goal was to ‘flatten the curve’, so our medical response infrastructure was not over run. We have met that goal. Was that a lie? If not, our economy has crashed and is approaching an unrecoverable inflection. If it was in error or a lie, there is nor reason to participate further. Either way, there is no longer any reason to participate in the lock downs.
Our national ‘lock downs’ have not suppressed ‘essential services’. Let’s give that greater consideration!
#FreedomIsEssential
#WorkIsEssential
#PrivateBusinessIsEssential
#PaychecksAreEssential
#SocialismIsNotEssential
#FascismIsNotEssential
#DictatorialGovernorsAreNotEssential
#BankruptingTheUSTreasuryIsNotEssential
Time to get back to work, before the government diktat ‘cure’ proves more lethal than the Chinese virus.
In response to J Mac, now that intensive-care capacity has not been overwhelmed, it will indeed be possible to phase out the lockdowns. Mr Trump has already sketched out a plan for easing lockdowns, and is calling out those states that are imposing them too severely. HM Government, behind the curve as ever, has still been unable to give any indication of the exit plan, and people are becoming justifiably impatient.
Though there was – rightly – support for the lockdown in the UK when it was clear to all that the health service would otherwise have been overwhelmed, now that that crisis has largely been averted it is time to get people back to work. We shall still have to take sensible precautions, but, on the figures as shown in the daily graphs, lockdowns have largely done their work.
…on the figures as shown in the daily graphs, lockdowns have largely done their work.
Post hoc ergo propter hoc
There is no evidence the slowing of the increase of infections is due to the lockdowns. Other predictions were made that the infection rate would reduce due to the normal response of a coronavirus to warmer weather. There isn’t any evidence for that, either.
There is evidence from serology testing worldwide that the infection rate is possibly more than an order of magnitude greater than the positive tests of those infected and reporting sufficient symptoms to be tested. There will be many cowering in place whose immune systems have successfully neutralized the corona virus infection. These are not in any of the models.
As a minimum those below age 70 should be cleared to live as normal although with special caution if they have vulnerable family living with them. Not restarting the economy will be a far greater risk to life than the decaying Wuhan corona virus infection rate.
In response to Ian W, it is not yet clear that the immunity conferred by clearing the virus will endure. In South Korea, there have been some cases who cleared the infection and were then reinfected. That is why one cannot rely on “herd immunity” until one can be sure that the immunity will endure.
PJF continues to get everything reliably wrong. The rate at which an epidemic spreads during its early stages is chiefly governed by the infectivity of the pathogen and the mean daily person-to-person contact rate, which, whether PJF likes it or not, has been greatly reduced in countries without lockdowns and very greatly reduced in countries with them. In Britain, the contact rate is down by 85-95%, according to cellphone data. It is a not particularly difficult calculation to work out how quickly hospital systems would have been overwhelmed in the UK if the contact rate had not been sharply reduced.
The later one acts to deal with an epidemic, and the less determinedly one acts, the more necessary and prolonged is the lockdown necessary to put matters to rights. With sufficiently determined action at the outset, as in South Korea or Taiwan, the epidemic can be prevented from ever getting its boots on.
Now that the lockdown in the UK has succeeded in its primary purpose of preventing the hospitals from being overwhelmed, dismantling the lockdown can begin.
PJF continues to get everything reliably wrong.
Monckton of Brenchley continues to resort to ad hominem and diversion instead of concentrating on addressing the point. I said there was no evidence the lockdowns were responsible for slowing the increase of infections. To counter, Monckton of Brenchley produced a collection of vaguely related, technical sounding boilerplate that, unsurprisingly, offered no evidence.
Indeed, Monckton of Brenchley’s own graphs offer no evidence the UK lockdown was responsible. The line began falling before the lockdown and has continued smoothly downward, without any indication that the “85-95%” reduced contact rate had the slightest impact.
Either Monckton of Brenchley’s graphs do not represent reality, or the lockdown’s impact was tiny compared to whatever really did begin the downward trend.
“…on the figures as shown in the daily graphs, lockdowns have largely done their work.”
Sweden, no lockdown, Norway, lockdown. Two otherwise very similar countries in most of the aspects (population, habits, health care systems, etc.) :
– try to find any significant difference in the daily cases curves between those two countries.
For instance, look at the two peaks and compare them to the population of each of those countries :
– no difference.
Wasn’t the purpose of the lockdown to limit the daily cases peak (flatten the curve !) so as not to overhelm the healthcare system ?
The fact is that there is not a shred of evidence of any lockdown effet on the daily new cases.
https://www.worldometers.info/coronavirus/#countries
Informative interview of a Swedish epidemiologist who explains, among other things, why the Ferguson pseudo-science paper (not even published nor peer-reviewed) is flawed :
This is a good video. There were many good questions asked and the epidemiologists does a good job answering them.
In response to Petit_Barde, the daily compound case-growth and death-growth rates in Sweden are appreciably above those in Norway. Indeed, the rate of growth in deaths is currently among the highest I am monitoring.
The rate of growth in death is not related to the lockdown policy but to many other factors (health care system, cases age distribution, cases co-morbidity distribution, cases stage of detection, adopted treatment, etc.).
As said before, with respect to those criteria, Sweden and Norway are very similar.
Lockdown can only have an impact on the total infected relative to the population.
In this respect, Sweden and Norway are in the same ball park :
– lockdown in useless.
Conversely, we will have to count the homeless, the unimployed, the suicides, the mortality due to delayed treatments, etc. This will be the very (and only actual) impact of this “pandemia”.
This pseudo-pandemia is a much ado about nothing and lockdown is just a way to create an actual economic and social disaster from a absurdly exaggerated problem.
As a British, you should adopt the motto :
Keep Calm and Carry On !
A claim is made in the video above that Sweden in general has larger nursing homes compared to Norway and this is reflected in the case and death statistics because of community spread in those homes.
Sorry Petit_Barde, but the total number infected depends totally on the number tested and you must know that.
But the Deaths do not.
Sweden 156/M population
Norway 33/M population
Denmark 63/M population
Finland 18/M population
Why are you obfuscating?
It does not matter what Comorbities the patients had.
It does not matter how old they were.
The Swedish System allowed them to become infected and they died.
Norway 181 dead
Denmark 64 dead
Finland 98 dead
Total 343 dead
Sweden 1580 dead
The Swedish system caused 1237 excess deaths compared to the other 3 nordic countries.
The present UK govt are just following the eugenics template……lose the old/sick/disabled and save money!
CMoB,
Wannabe fascist Governors like Jay Inslee-WA and Tony Evers-WI are stating that, if the serfs don’t stop complaining about the government boot on their economic throats, “more draconian measures will be needed”. Freedom loving peoples reject draconian diktats. We have no love for kings or dictators, here in the USA. It is encoded in our national DNA, our Constitution, our Amendments, and our Representative Republic.
Washington and Wisconsin state citizens are going back to work. If #JapingJayInslee and #WorstGovernorEvers choose the police powers of the state to further apply the heavy boot of government to the economic throats of Washington and Wisconsin citizens, their “draconian measures” will spawn an open revolt. Wannabe dictators, take heed! The foment is nearly at boil!
I will be in Madison this Friday to help make it clear via peaceful protest that most Americans feel that way.
Bless you, Dave Miller!
I live in WA state and have family in WI. Jay Inslee and Tony Evers are ‘two of a kind’, in decidedly unflattering similar ways.
I always thought an ex-spurt was a has-been drip under pressure.
I think we need proof of how many died to Corona virus.. So far none.
And still no peer review of Neil Fergurson’s work.
“In a new analysis, the Centre for Evidence-Based Medicine (CEBM) at the University of Oxford argues that the lethality of covid19 (IFR) is between 0.1% and 0.36% (i.e. in the range of a severe influenza).”
Agreed.
I don’t understand this thing “dying with” or “dying of” COVID 19.
In uk medical certificate of death have four options for cause of death.
Ia, Ib, Ic and II.
I think it works like this.
Example :Elderly person has diabetes and hypertension but died of pneumonia heart failure caused by COVID
Ia heart failure
Ib pneumonia
Ic COVID
II hypertension ( doctor may consider hypertension impacted death but not diabetes)
If the above is done correctly the statistics of each country should pick up what is the key co-morbidity. This will further fine tune most at risk
“Dr John Ioannidis of Stanford University has released the results of a serology study done on a sampling of Santa Clara County residents. He sat down with John Kirby from Journeyman Pictures to explain the results.
The study found that between 2.5% and 4.2% of residents have antibodies relating to Sars-Cov-2, a far greater percentage than ever previously thought, between 50 and 85 times higher than initial estimates”
https://off-guardian.org/2020/04/19/watch-covid19-fatality-rate-in-the-ballpark-of-seasonal-influenza/
There are huge question marks regarding this study. FFS, the population sample were invited for testing via a Facebook ad. It’s complete nonsense.
How does Facebook make it “complete nonsense”? The sample was selected from those who answered it to make it random. Yes, the study is not conclusive but what data is then? Ionaddis is no fool, and no crank, and this is not an isolated result – there are now 10-15 good examples that the infection rate is far higher than the models think, and the death rate consequently much lower. We have twonaurcrsft carriers two studies of pregnant women, two studies in Germany and Italy, the infection rates amongst all cause deaths, and more. All point to the same thing. And very little support g the original death rates. FFS.
A Facebook ad attracts those who are interested in the topic, i.e. people who think they have had the virus or been in contact with someone who has had it. It’s not random.
I don’t know what you mean by the “original death rates”. If you are referring to the CASE fatality rates then so what? We know they were wrong but NO-ONE used them in any model. Ferguson used 0.9%.
Viewing FaecesBook is a sample bias all on its own. You cannot “randomise” out a bias in your sample.
Who does FB algos choose to throw this ad at ? Another totally unknowable bias.
That does not mean the result is wrong. It could right despite the sample bais, or right for the wrong reason. The problem is you can’t know that. So “complete nonsense” may be a bit dramatic but it is very poorly constructed and should not get past peer review as a method.
There are indications that 2.5% is too low.
“How does Facebook make it “complete nonsense”? The sample was selected from those who answered it to make it random. ”
no.
the bias is called self selection bias
In Santa Clara county you could not get a test unless you had severe symptoms
So, if you had had symptoms and could not get tested, then you are likely to sign up
for the free test to find out.
And bring your kid which was allowed.
people who thought they might have had corona were motivated to take the test.
For example, 100 people ( twice the number that tested positive)
showed up with invalid or IDs that did not match the ID they used to sign up
Mother perspective: I do not think there is any chance I am exposed. Therefore, why on Earth would I go out to a place people who think they might be sickness gathering?
People not infected have avoided getting infected by not taking unnecessary risks.
So, what reason could I have to respond?
To toss a negative into the mix so they get an accurate result?
So self selection bias, plus self elimination bias.
Huge question marks over Neil Ferguson’s work. He has never been correct on any of his predictions and his work is not peer reviewed.
Ferguson’s UK model looks to be spot on though he may have under-estimated hospital deaths.
Under current intervention measures, Ferguson’s model predicted we would remain within ICU capacity and that the UK hospital numbers would peak at the week-end of April 10th 2020.
My daughter (Birmingham,UK) emailed me last night to inform that numbers peaked at their hospital on April 10th and have been falling ever since. She is now involved in planning a return to normal.
Like I said – SPOT ON.
except we cannot confirm who died “with” or “of ” the disease.
So not spot on.
Though in the UK I am sure they will circle the wagons to confirm his numbers. Luckily other countries were not so foolish to shut down and will always be there to mock his non- peer reviewed work.
Richard, as usual, is allowing prejudice to override reason. Ferguson’s model said when the pandemic would peak. It appears to have peaked when he said it would. He also predicted that the UK, with lockdown, would remain within intensive-care capacity. We have remained within capacity. The question whether one books deaths of Chinese virus as merely with Chinese virus is irrelevant to these two predictions, which have proven correct.
If Richard were to talk less and read more, he would know that Ferguson has made his code available to international experts for scrutiny and, that early results indicate that the code has passed muster.
It is not appropriate to attack someone’s model merely because one does not like the results. One must have a good reason. Ferguson is wrong when he says that large gatherings do not have much impact in spreading the infection, as South Korea’s experience with a church gathering has demonstrated. But that does not make his entire model incorrect.
Ferguson’s model predicted that in the absence of control measures the infection fatality rate would be about 0.5%, or 40 million deaths out of 7 billion infected by the end of this year. That infection fatality rate appears to be borne out in reality, thus far. My own estimate, based on casting back deaths, was 0.1 to 1%, midrange estimate 0.34%. Ferguson’s estimates are consistent with that.
Monckton of Brenchley wrote:
. . . Ferguson has made his code available to international experts for scrutiny and, that early results indicate that the code has passed muster.
Selected academics privately investigate fellow academic – no problems found. Never seen that before, have we?
Apparently if the code is to be released publically it will have to be “cleaned up” first. Yes, I’m sure it will scrub up nicely.
Christopher: “Ferguson’s model said when the pandemic would peak. It appears to have peaked when he said it would.”
So, it peaked on April 10th, the very day the UK chucked 3,000 or so late tests and so a lot more “new” cases into the mix? BTW, the Netherlands, Portugal and Ireland also had huge peaks of new cases on that day. Yeah, right. Do government reported stats represent reality, or do they merely follow the models? Oh, and I can think of another area – “temperature” – in which that may also be a problem.
Monckton of Benchley, is now ignoring all the data illustrating that the Virus is about the same as a heavy flu and –
“New data of German authorities show that in Germany, too, the reproduction rate of Covid19 had already fallen below the critical value of 1 before the lockdown. General hygiene measures were therefore sufficient to prevent the exponential spread. This had already been shown by the ETH Zurich for Switzerland as well’
Monckton of Brenchley is ignoring the fact that it was Neil Ferguson’s first prediction of 500,000 dead that led to the lock down.
I thus find the him unreliable and cherry picking facts.
The point is Ferguson’s work was not peer reviewed and should have been based on all his other predictions from the past being hopelessly wrong.
In any company he would have been sacked and yet still , Mr Monckton, continues to protect him
Warning.
Monckton articles – read with caution.
Monckton- “my own estimate, based on casting back deaths, was 0.1 to 1%, midrange estimate 0.34%”
We all knew this “According to data from the best-studied countries such as South Korea, Iceland, Germany and Denmark, the overall lethality of Covid19 is between 0.1% and 0.4% and thus up to twenty times lower than initially assumed by the WHO’
“A new serological study by Stanford University found antibodies in 50 to 85 times more people than previously thought in Santa Clara County, California, resulting in a Covid-19 lethality of 0.12% to 0.2% or even lower”
“The Finnish epidemiology professor Mikko Paunio from the University of Helsinki has evaluated several international studies in a working paper and comes to a Covid19 lethality (IFR) of 0.1% or less (i.e. in the area of seasonal influenza)’
“A US study comes to the conclusion that the new corona virus has already spread much further than originally assumed, but causes no or only mild symptoms in most people, so that the lethality rate could be as low as 0.1%”
If Neil Fegurson had any credibility his work would have reflected this but in his usual form he went full on alarmist.
The mention of 500,000 dead led to the lock down.
actually, China shutting down led to the lock down. They gave a penny ante in a 100 trillion dollar bet. Can we set the world up to lockdown? They won the bet and are still in total control of the game.
Plenty of info coming out now-
https://www.businessinsider.com/south-korea-coronavirus-testing-death-rate-2020-3?op=1&r=US&IR=T
That was published March 5th — over 6 weeks ago, and probably based on information even older. That’s worthless for decisions that need to be made now.
What crisis in NYC!
This lad goes round NYC on his bike and a camera. Check him out before he’s taken down . . .
the first 17 videos –
https://www.youtube.com/user/lincolnkarim1/videos
That guy’s videos are amazing. It appears that they’re us absolutely no crisis in NYC. If this is true, and it would be very difficult to falsify his evidence, it appears that the Mendacious Sensationalist Media are pushing a real fraud, and NYC is trying to cash in on it in the worst way.
https://youtu.be/eBfDTwScCLI?t=71
What a jerk. He’s screaming at a friggin ambulance driver “switch the damn engine off!” when he had been told repeatedly they are not allowed to do that.
Yet another leftist TWAT having a hissy fit because someone will not follow his political agenda.
I’m sure this must be the same guy who was in vidio shop screaming “It MADAME actually” after being “misgendered”, before offering the sales attendant outside to show him how “female” he was.
This asshole is berating front line workers in the middle of a crisis for creating “pollution” on a day when there’s no traffic in NYC. Total disconnection with reality but a great change be WOKE.
Now what exactly does this show about “crisis ” or not. Maybe link to vid and a time which you think we should look at.
He sounds like Henry Pool, but his video of the Central Park BS Hospital is worth a look.
It all looked pretty deserted on the ones i watched.
Why does this drivel continue. Why not consider what actual epidemiologists like Knut Wittkowski say?
Or how about this:
https://www.who.int/mediacentre/news/statements/2017/flu/en/
https://www.pbs.org/newshour/health/cdc-says-more-people-die-of-influenza-worldwide-than-who-estimated
This info ought to be the lead in any story about the dangers of C19.
Think the MSM doesn’t have an agenda?
And by the way, here in Japan, classes of H.S. students at cram schools were packed through the first week of April. Could it be that Japan’s extremely low death rate was due to allowing herd immunity to develop.
It does not seem possible that herd immunity was achieved in Japan when all of the statistics show few cases. Of testing done there, more than 90% of those tested are not carrying the virus.
There is some other factor(s).
The most successful nations at containing the virus so far have been S Korea, Taiwan, Singapore, Hong Kong , Greece, Australia and New Zealand.Eg Australia with a population of 25 m has had about 6700 cases and 70 deaths whereas Sweden , which has had a relaxed social mixing policy has had some 1500 deaths in a population of 10m- only 40 % of Australia’s
The methods these succeesful nations have used vary so there does not seem to be any one star best method but what does seem common to them all is that they acted decisively early’
This is essential because in the early stages of the virus striking a country the infection multiplier can quickly reach 2.5 or 3 ie so 10 infected people can infect a further 25 or 30 and so on
In Australia we have now contained that multiplier to 0.5 so 4 infected will only infect 2 and those 2 only another one Thus if this continues the virus will eventually peter out
It can be seen from the above the necessity to act early before the multipliers have a chance to get going
How that is done has varied across the above countries whose methods have variously included rapid imposition of border barriers, wide spread testing, mandating social distancing methods including various levels of economic lock downs and reduced social interactions eg sport, restaurants, bars, clubs closed and requiring personal distances, follow up contact tracking, widespread use of masks and improved hand hygiene plus rigorous protections for those liable to infection ie medical staff plus testing of staff in care and nursing homes etc
“The methods these succeesful nations have used vary so there does not seem to be any one star best method but what does seem common to them all is that they acted decisively early’
yes, yes ,yes,
The same held true in 1918 with the Spanish flu.
A bad decision taken quickly and measured beats waiting for better data and certainty.
Patton: A good plan violently executed now is better than a perfect plan executed next week
Look. People approach this problem thinking they can engineer their way out of it.
if we only had good numbers
if we only had better models
If we only had double blind studies of medicine
The list goes on.
The simple fact is that action was required; it was required to act under EXTREME uncertainty
with the Bonus wicked condition that the problem would spread exponentially
for a while.. how long? nobody knew. Nobody will ever know.
the other day I was reading an interesting piece that compared infection rates in cultures
that kiss on the cheek, versus those that shake hands, versus those that bow.
guess what?
who knows maybe slowing the virus was a simple as wash your hands, cover your cough (with your elbow) don’t touch your face or shake hands? you’ll never know with certainty. especially when people
don’t listen to advice. Free advice at that.
When you told others it was no worse than the flu, when you focused on uncertainty did you influence people to be a little lazy about these simple measures? you’ll never know.
How many people got infected because of nancy pelosi’s advice to celebrate in SF china town?
You’ll never know.
here is what we do know. In early Jan the mayor of Wuhan went ahead with a local celebration
that 10s of thousands of people attended. And if you were watching you saw him get spanked by Beijing. There’s a clue for you. But apparently people could not learn by watching others fail.
Anyone who could not see that urgent action was required must have been residing on another planet in January and February 2020. China building a massive hospital in Wuhan to treat the sick and dying was one of the more dramatic early clues.
Sick, dying and dead being stretchered off the Diamond Princess in Japan was another vivid clue.
Taiwan is, without a doubt, the gold standard of action and outcome. Acted fast, closed borders and began tracking. Six deaths in a population of 24M. Taipei has twice the population density of London. There is nothing better than being prepared, using lessons from past experience.
I am certain Boris Johnson would mark his actions on CV19 close to bottom of class. He has some credibility for surviving the virus and recognising the efforts of the medical team that got him through it.
ScoMo in Australia took a great lesson from the 2019/2020 bushfire season. He created the emergency cabinet that comprised the State Premiers, himself and key Federal Ministers as required. They meet regularly (almost daily) on internet hook ups and co-ordinate action. The Federal Government has limited powers to act internally but considerable resources in terms of military and money supply – the Premiers have authority to act on internal matters. The States have some variation but they at least know what each other State is doing. ScoMo has proven a great leader in the circumstances. Australia has 71 deaths in a population of 25M. Could have been considerably less with earlier action but way above average.
The WHO was praising China’s response in late January and into February noting that China had helped to prevent the disease from spreading to other countries
The WHO finally made the assessed a pandemic on March 11.
If he (BoJo) had not been PM, he wouldn’t have gone into the ICU. He didn’t need that level of care. Most hospital CoV patients are not in an ICU.
And his sluggish reaction, which was probably intentional, has effectively delivered his “herd immunity” just the same. While avoiding the level of blame attribution that no action would have led to.
For once I’m happy to agree with you Steven.
Most countries dithered and acted on the problem far too late, especially the UK.
However, this pandemic might turn out to be a success, bizarrely, for the UK.
In the winter of 2017/2018 there were 50,000 Excess Winter Deaths (ONS), ‘Excess’ being over and above the number of deaths we could usually expect during other periods. It was a bad flu year, but passed with barely a murmur.
I have no idea what the total deaths this winter are yet, I don’t think the ONS keep a running total, but it’s worth noting that although Excess Winter Deaths here have been falling, the average is still ~20,000 or so.
How illustrative of our NHS will it be if, during a global pandemic, the country ‘recovers’ with fewer Excess Winter Deaths than during 2017/2018?
The problem is that COVID19 is not in the normal Winter period, only March is considered near wintertime.
This is a Spring epidemic after the flu season has usually finished, it could even become a summer one.
I once remember reading a comment on the lines of “everyone will make wrong decisions what makes a good executive is making the right wrong ones”. It appears that this was the essential first step when there was little accurate information, making the right wrong decisions.
Richard
It is what is called following your gut feelings. Some people have better intuitions than others — or longer streaks of good luck.
Your leaving out Vietnam. 268 cases and ZERO deaths out of a population of 97M. Vietnam reacted the minute they heard the words “virus” and “China”. They have been down this road with the Chinese before. They fought to stop the introduction of the virus rather than the spread of the virus.
My information from Hanoi says that they went into shut-down before we did in Australia, and isolated several towns with the virus. They definitely worked at controlling the spread.
Let me rephrase. Vietnam fought from the very beginning to stop the virus from arriving in Vietnam by shutting down borders and airports very quickly. Very few people arrived with the virus. For the few that did their ability to trace the infected persons contacts and quarantine both the infected person and all contacts was swift and effective. But this strategy was only successful because so few infected people were ever allowed to enter the country.
Vietnam did react quickly, but its low case numbers and lack of deaths are dubious.
CPT Crozier, skipper of USN carrier TR, docked in Da Nang on March 5 because he was assured that the only CPC virus cases were in the north. Yet with few crew ashore, his ship was infected. One sailor has died.
CVN-71 also took on some stores in Vietnam.
Eg Australia with a population of 25 m has had about 6700 cases and 70 deaths whereas Sweden , which has had a relaxed social mixing policy has had some 1500 deaths in a population of 10m- only 40 % of Australia’s
I’ve read on one forum explanation from a Swede – they dropped the ball not protecting enough care homes where virus wreaks havoc now what pushes mortality up. They also weren’t doing enough testing. Still, longer term comparison is still to be seen. It may turn out that Swedish know what they’re doing. The main purpose of the lockdowns after all is to protect hospitals from overwhelming and, as far as I’m aware, this is not happening in Sweden, despite relaxed lockdown.
There are signs of resurgence in Singapore.
Yes, their numbers are rocketing this week:
https://www.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6
That is the Johns Hopkins world ‘sick map.’
“We don’t know for sure, because a third of all British deaths arise outside hospitals and are thus ingeniously excluded from the Government’s daily counts, though the Office for National Statistics is now publishing a weekly parallel series giving the real numbers.”
Most other countries don’t include deaths in nursing homes or at home so to get a like for like picture these must be included for all nations.
We also need to sort out those who died WITH CV and those who died OF it. Again we are following WHO CV guidelines on this as are Spain and Italy. If we want to get a fair picture, either every nation needs to work on the WHO parameters or we need to sort out ourselves the genuine CV deaths from the remainder.
Yes, Christopher’s remark is nonsense. There is no ‘ingenious exclusion’. What happens is that there are two independent systems of death reporting in the UK, and they work on different timetables.
The first system is transmission of data from hospitals to Public Health agency. Since the UK operates a mainly socialized and centralized medical system, the hospitals are used to reporting lots of data, and so they report all tested cases which have died. This doesn’t happen overnight, but each day there is a total which is all those reported in the last 24 hours. It will contain deaths over the last few days, because not all hospitals get their deaths in immediately.
Then there is a separate system for recording deaths outside hospitals. Its the usual system of doctor issuing death certificate in cases where the death was at home or in other non-hospital institution. It is not deaths of tested cases, the diagnosis is based on the judgment of the attending physician.
Not surprisingly, this second system results in later reporting of deaths than the first. Its also much more fragmented, so the reports trickle in.
The agency that reports these is the Office for National Statistics. Their report has at least a one week lag.
No-one is trying to conceal anything, no-one is being ingenious. The various bodies are simply reporting the numbers they have, and then catching up as more data comes in.
PHE also reports in detail how many of the hospital deaths reported on a given day actually occurred in the last 24 hours, and how many occurred on each of previous days. So no, there is no ingenious attempt at concealment there either.
The reports are still useful and indicative despite this, because the method is consistent since the start. So 1,000 deaths falling to 500 is still indicative, because it really does show a fall, even if that fall is not from 1,000 in the last 24 hours to 500 in the last 24 hours. Over a couple of weeks this gives you an idea of trend.
However, in the UK, the key indicator is bed occupancy rates. These are published every day in the afternoon at the daily government press conference, and they show at the moment that occupancy rates are definitely falling. Death rates should follow.
Suggestion of UK government attempts to manipulate the data are ridiculous to anyone who takes the trouble to examine what is known and what is being published.
In response to Michel, there has been considerable, and justifiable, criticism of HM Government for not making it clear at its daily press conferences that the death count should be 50% higher than the figures it is reporting. The people want the clearest possible picture, and the Government is not giving it to them.
It has been quite clear since the start of U.K. Government daily reports that the figures were for hospital deaths only. Please get off you hobby horse and stick to your graphs, which are informative.
In response to Mr Snook, as the South Koreans have demonstrated it is necessary to make sure that all deaths of those infected with the Chinese virus, and not merely those from hospitals, should be included in the daily totals. This is a pandemic. One cannot afford to dilly-dally as the civil service usually does.
As Mr Mosher has pointed out, there will be some cases where the cause of death cannot be immediately determined. However, in most cases, death from the Chinese Virus is not difficult to detect, to attribute or to report.
A uk medical certificate cause of death MCCD has four spots for cause of death.
AFAIK the MCCD should be submitted to registry office with nine days under normal circumstances. Under our current circumstances why can’t a team of admin staff input all the data daily.
There have been thousands of COVID 19 deaths in various western nations.
The full stats should be available on co-morbidity to determine a theme of deaths.
Much of the death rate of Covid19 can be attributed directly to the fact that N95, N99 and N100 – even P100 masks are only designed to stop 0.3 micron and larger particles… and Covid-19 is 0.125 microns in size. Due to the masks creating a rather large negative pressure when used while exerting effort they simply “atomize” the virus right off of whatever it is lightly stuck to and the person wearing the mask becomes infected. Many of these masks are NOT designed for medical situations and have front-venting exhalation ports that blast the wearer’s cooties right onto patients or other surfaces.
Turns out that HEPA systems are designed for 0.01 microns but only if you buy ACTUAL HEPA cartridges, most filters for “HEPA” units rely on multiple passes through the filter to achieve removal.
So the problem, and likely the thing that most caused the deaths, was Trump de-funding the CDC department tasked specifically with detection and response to coronaviruses.
Alcohol doesn’t touch coronaviruses. France has found some strains that will survive 1 hour at 200°F.
Coronaviruses are *not* ‘alive’, they are little encapsulated punji sticks of DNA. They survive up to 80 days in controlled environments and can be distributed globally inside commercial packaging.
I doubt even the special department at the CDC was fully ready for this one.
“Swiss chief physician Pietro Vernazza
The Swiss chief physician of Infectiology, Professor Pietro Vernazza, has published four new articles on studies concerning Covid19.
The first article is about the fact that there has never been medical evidence for the efficacy of school closures, as children in general do not develop the Covid disease nor are they among the vectors of the virus (unlike with influenza).
The second article is about the fact that respiratory masks generally have no detectable effect, with one exception: sick people with symptoms (notably coughing) can reduce the spread of the virus. Otherwise the masks are rather symbolic or a „media hype“.”
Richard, who is reliably wrong about everything, says masks do not work except where worn by sick people with the symptoms, whose coughs and sneezes even the most basic mask will prevent from circulating. But one does not necessarily know that one has the virus. One could spread it inadvertently. That is why everyone should wear masks in public, as the South Korean chief of public health has made clear.
“Richard, who is reliably wrong about everything” Mr Moncton in his wisdom is now criticizing The Swiss chief physician of Infectiology, Professor Pietro Vernazza .
“The Swiss chief physician of Infectiology, Professor Pietro Vernazza, has published four new articles on studies concerning Covid19′
“The second article is about the fact that respiratory masks generally have no detectable effect, with one exception: sick people WITH symptoms (notably coughing) can reduce the spread of the virus. Otherwise the masks are rather symbolic or a „media hype“.
In 2018 and 2019 Trump asked for increases in spending for emerging infectious diseases, Congress passed larger increases and Trump signed those budgets.
I am somewhat puzzled by Prjindigo’s report that the Covid-19 virus is small at 0.125 microns thus purportedly rendering most masks unable to prevent its inhalation as they are designed to stop particles 0.3 microns and larger
Yet tThe argument for the 1.5 metres social distancing was made on the basis that the virus was relatively “large and heavy” and could not be borne in an aerosol and thus would “fall to the ground” within that space if maintained between people.
Can you shed any light on this apparent contradiction please?
A much higher percentage of severe cases of Covid-19 among men than among women indicate some role for male sex hormones, in particular 5-alphahydrotestosterone (DHT). In that case, you should think about the use of Sabal Palm Extract by men.
OMG. I call BS.
Really Ren? How do you narrow it down to such a specific factor like DHT when there are likely dozens of very real differences both social and genetic between men and women?
Stop the BS. Stop the snake oil selling.
This is quite obvious if you associate age (over 45 years) and gender. Look at the statistics from New York.
https://www1.nyc.gov/assets/doh/downloads/pdf/imm/covid-19-deaths-confirmed-probable-daily-04192020.pdf
Confirmed
-Female 3399 (38.6%)
– Male 5385 (61.1%)
– Unknown 27 (0.3%)
Death rates of males are higher than females, particularly so in the 60 to 80 year old range, no matter what the cause, ranging from 30 to 50% higher depending on place and circumstances.
Insurance companies should stop charging lower life insurance premiums to women. That’s sexism and therefore despicable.
It appears that women are not prescribed ACE inhibitors (ACEi) and ARBs nearly as much as men are, especially women who can become, or are, pregnant, where they are contraindicated.
ACEI-induced cough is twice as common in women as in men, which suggests other treatments are used, as is done in E Asia countries because E Asians experience a similar side effect; calcium channel blockers are the first-line treatment in those countries instead of ACE inhibitors.
Diuretics appear to be used in elderly individuals.
Maybe it is because semen is loaded with zinc, vitamin C and B-12.
As far as masks and other PPE goes with this +strand RNA respiratory virus that is very contagious … a virus that likely escaped out of a BSL 3+ or 4 level of containment measures in Wuhan China with personnel with various levels of PPE training. A virus that likely was circulating for multiples of weeks in each location before health authorities took note.
Does anyone really think Joe-Blow the average guy who has never been taught how to wear an N95 mask (or handkerchief or any mask) on his face can stop this?
So you are saying that the Head of Medicine of South Korea, who has been through 3 epidemics and controlled both the SARS and COVID19 ones actually doesn’t know what he is talking about?
Because he says that it is ESSENTIAL that everybody wear Face Masks, Glasses and Gloves when outside of their own homes.
Have you not watched his video?
Mr O’Bryan does not understand the elementary epidemiology of containment. As the South Korean chief of public health explains it, face-coverings are not perfect, but they do pose a considerable barrier to the virus, particularly by intercepting particles that would otherwise be emitted by the wearer’s coughs and sneezes. To control a pandemic of this kind, wearing masks in public makes obvious sense. It is simply not appropriate or prudent to be reckless.
To avoid a pandemic of this kind don’t slaughter animals in unhygienic ways.
People wearing mask drive me nuts.
When I see an Asian person wearing a mask it triggers my insular cortex and amygdala causing disgust/fear/anger. It just happens it’s natural.
This COVID really wears you down.
When we analyse disease burden simple things such as headache and backache are some of the highest burden on western society.
Health wise the sum of the individual stress of millions of citizens may be a greater disease burden than COVID 19 deaths
I would not compare death rates just yet. Those of us in the Southern Hemisphere who have partially strangled the outbreak may be in for a second whammy come our winter flu season. Random testing in NZ is showing very low infection rates. But, there is enough community transmission to explode if the conditions are right
If this is a persistent virus it will keep going, one way or another, until herd immunity is near-saturated
I remain of the view that season and temperature is a prime influence
This show ain’t over yet, by a long shot
CMofB
It is these meetings that are intended to be the gathering-place for information garnered by Britain’s various intelligence services around the world, under the aegis of the Prime Minister and the Chief of the Joint Intelligence Committee. Had Mr Johnson attended those meetings, he would perhaps have intervened to do something about the then-alarming daily case-growth rate at least a month earlier than he did.
I assume you have the read the minutes, then? Johnson does have a number of ministers who deputise for him and presumably he will be aware of the meeting agenda. The suggestion that the PM needs to attend every single meeting to know what’s being reported is ridiculous.
The rest of this post is in the same vein. There is good reason to keep the hospital and community deaths separate.
1. Hospital deaths have actually been tested for Covid-19 so they are those that have died from the TESTED population.
2. Community/ Care Home deaths have not been tested. They are not part of the Test numbers.
3. Hospital deaths give a clear consistent dataset which enables policy makers to assess the success or otherwise of any interventions.
4. ONS figures are based on death registrations which lag reported hospital deaths.
Considering that the whole purpose of any intervention strategy is to prevent the healthcare system becoming overwhelmed it is the hospital numbers are of immediate interest.
Regarding your suggestion that Johnson should have intervened “a month earlier than he did”. The UK government issued the ‘lockdown’ instructions on March 20th. A month earlier would have been before Italy or Spain had taken measures and before the UK had any evidence of community spread. While there were a handful of cases in the UK these has all contracted the virus abroad. Most of Europe considered Covid-19 as low risk in the early part of the year.
The post is simply a rant.
Good point about deaths in care homes – these are usually not tested though there is an anomalous increase I reckon (compared with baseline from previous years for the same weeks) what suggests covid underneath.
As per earlier action I understand His Lordness differently – he’s not advocating strict lockdown in the UK in January, he’s advocating early mass testing, contact tracing and travel restrictions, in short bring here South Korea approach. And in this BoJo failed miserably. Lockdowns are only necessary when this preferable approach failed and virus spread is out of control.
The UK did early testing. That’s how they knew that the first few cases had contracted the virus abroad and it was via contact tracing that they knew that there was community spread on Feb 28th.
It is true they had trouble sourcing test kits so mass testing was difficult but the real problem for the UK (and NY and to a lesser extent Madrid & Milan) was the outbreak in London. This would have been like looking for a needle in a haystack even with a mobile fully-equipped testing unit.
The 2 countries who appear to have been most successful on testing are South Korea and Germany but both of these countries ‘enjoyed’ an element of luck. South Korea, in particular, found around 2/3 of their early 8k cases were among a religious sect. They tested all 210,000 members of a secretive group who were effectively semi-self isolating anyway. I’d argue that SK never really experienced an outbreak.
Germany also discovered a significant single source of infection from those returning from Skiing trips. This gave them a strong lead on further cases but, credit to them, they got on the front foot and stayed there.
I still believe, though, there probably are a number of confounding factors that we don’t fully understand yet. For example What is happening in Belarus. Nothing has been cancelled. There was a full league programme of football on Saturday. The President has advised the people to drink vodka and take regular saunas ( backed by science as it happens) to ward off the virus. Belarus has recorded 5 deaths per million – Germany’s has 55 deaths per million. Poland & Ukraine have also got off pretty lightly.
The epicentre has tended to track across western Europe.
Older, unhealthier and fatter populations in Western Europe?
tonyb
Can that explain the difference between 5 per million & 200+ per million?
Belarus has recorded 5 deaths per million…
Recorded and had are two different things. You can’t trust any figures out of Belarus. It is a bizarre half-communist dictatorship. The most interesting thing that will come out of Belarus, which they won’t be able to hide, is whether COVID-19 will cause massive death or economic destruction. I predict neither.
In response to Mr Finn, the UK’s pandemic containment plan, unlike that of South Korea, was fatalistic: it assumed that containment would fail – which it duly did. In South Korea, the program of testing, isolation and contact-tracing was a great deal more vigorous than in the UK,, which is why it worked.
Mr Finn, in drawing attention to Belarus, is failing to take account of considerations such as spare ICU capacity, which was nonexistent in the UK, and therefore obliged the UK to lock down so as to delay the transmission of the infection. Now that the lockdown has achieved its purpose, it can be slowly and carefully dismantled: but the UK, behind the curve as ever, has thus far failed and failed and failed again to reveal to the nation what steps it proposes to take to end the lockdown.
I’m not arguing against the lockdown. I’m simply suggesting there may be a number of confounding factors when comparing death rates.
Mr Finn has not, perhaps, attended a COBRA meeting. However, the purpose of such meetings is to exchange information and take decisions on important risks. The Prime Minister’s absenting himself from those meetings for five successive weeks is rightly and widely regarded in the UK with more than a little dismay. Reading the minutes after the meetings is no substitute for being there.
And there is no good reason to keep hospital and community deaths separate. The South Koreans require every death of anyone infected to be reported immediately, so that proper decisions can be taken in a timely fashion. One understands that many commenters here have no experience in containing pandemics, but one of the iron rules of successful containment is accurate and up-to-date information, particularly about those who have recovered and those who have died. HM Government has not been keeping proper records of those who have recovered, and it has not put any system in place for immediate reporting of deaths that occur outside hospitals. These elementary steps would have been taken by any competent administration.
And of course the Government should have intervened immediately. There should have been a proper system of testing, isolation of carriers and tracing of their contacts in place, and it should have been vigorously pursued with the aim of preventing the infection from spreading at all. This was not done. Once it was clear that it had not been done, the country should have been locked down a month earlier than it was. My household was locked down by the end of February, not by 23 March, the date when the Government finally got around to locking the country down. In the containment of pandemics, hours count, and one should certainly not dither for weeks, as HM Government did, while the experts on the activist and passivist sides of the debate continued futilely to wrangle.
1. COBRA. Johnson has a full cabinet of presumably capable ministers at his disposable. From wikipedia
The composition of a ministerial-level meeting in COBR depends on the nature of the incident but it is usually chaired by the Prime Minister or another senior minister,
This is exactly as I understand it. PM is often absent if there is more pressing business to attend to. Brexit took priority earlier in the year.
There is. There would be no consistency. Hospital deaths are those that have been tested. Community deaths haven’t been tested. There is at least a 10 day lag between ONS reported deaths and the hospital deaths. Mortality is a key indicator of the response to interventions. To keep lumping community deaths from a fortnight previously in with hospital deaths distorts the picture.
In fact I’m not sure you fully appreciate the lag in the hospital deaths. It now looks as though the mortality peak was on April 8th – but for London it was 4 days earlier. Given that the average time between infection and death is at least 3 weeks and that the UK lockdown began on March 23rd it’s just possible the lockdown was unnecessary.
There would be no consistency. Hospital deaths are those that have been tested. Community deaths haven’t been tested. There is at least a 10 day lag between ONS reported deaths and the hospital deaths. Mortality is a key indicator of the response to interventions.
I’ve heard ONS is compiling and will release some fresh data later this week so we shall see. From what I’ve heard from today update they estimate hospitals deaths account for 8-9 out of 10 covid related deaths. If that’s correct that lives the question about increase in ‘community deaths’. Before today update there was an interview with a lady from the Imperial College – she indicated there is a surge in non-covid related ‘community deaths’ again calling people not to be afraid calling for help if needed. If that’s confirmed it’s concerning. We hear continuously how many lives lockdown is saving what is great. For the full picture we should also hear how many people lockdown is killing.
Yeah, looks like there is a surge in deaths across the UK:
The Office for National Statistics said there were 18,500 deaths in the week up to 10 April – around 10,000 more than is normal at this time of year.
More than 6,200 were linked to coronavirus, a sixth of which were outside of hospital.
But deaths from other causes also increased, suggesting the lockdown may be having an indirect impact on health.
Nick Stripe, head of health analysis, said they were trying to understand what had been happening with this increase in non-coronavirus deaths.
He said it could be that people with other illnesses were avoiding going to hospital treatment – visits to A&E have halved since the pandemic started.
But he added it could “take years to work out”.
Coronavirus: Number dying hits 20-year high
———
So yes, that confirms that lockdown is saving some lives. And is killing other lives.
A theory about why ‘large gatherings’ and ‘super spreading’ could be combined: by aerosols.
Large gatherings (churches, stadiums, huge parties etc.) often know loud speaking and / or singing. What happens when singing or when speaking loud is that air is forced between vocal cords under higher than normal pressure. Theory: high pressure and high speed in ‘narrow spaces’ (vocal cords) could easily lead to the formation of VERY SMALL droplets that easily can form aerosols.
In case of sneezing smaller droplets are formed as well: also in high pressure circumstances: https://youtu.be/vBvFkQizTT4?t=41 (some minutes)
It has been proven that aerosols remain a long time in the air, potentially infecting a lot of people: super spreading.
How much I believe about this disease is hard to quantify, however Sweden is not locking everyone down and they are not, so far, experiencing catastrophe. This makes me doubt Britain is out of line with other European countries unless the population here have less natural immunity that other countries. There maybe some substance to that notion as we have a substantial percentage of our nation who eat too much, hardly ever exercise and look as if hygiene is not something they necessarily care about.
Laying this aside what must confuse, well it does me, is how deaths are being recorded, especially those that are going to occur anyway. People die everyday from a myriad of causes, so not every death, even if the individual has contracted COVID-19, can be laid at the door of this disease. Many would have died if we had a bad flu epidemic. This assessment makes the reaction to the epidemic frightening given the damage it must do to the economy, not least because next winter we need to have enough food, a concern as Britain only supplies little more than 55% of its own needs. If the world economy is damaged we might not be able to get enough supply!
“As the South Koreans have discovered, it is far from clear for how long the immunity acquired by those who have recovered from the infection will persist. Until that central question is answered, it cannot be safely assumed that population-wide immunity will be rapidly or effectively acquired.”
That is important question.
Hmm. You could say you are not going to get the question answered, soon enough.
And there number other questions, you aren’t going to get answered, soon enough.
In terms of lockdown, I think events will overcome it, and the rational process of getting the answers
to questions will be later- or too late to help with planning issue of leaving the lockdown
Or doubtful Italy going to have the answer, they going to get out of lockdown fairly soon,
And it looks like Sweden is going to solve their Chinese virus problem, fairly soon.
Roughly it seem Sweden new daily cases has leveling off for about week, and roughly could continue to
level off in another week. Sweden death per million is 152 and likely it will reach 200 per million
in one week. Or Sweden total is 1,540 and be total around 2000 in a week, is not type of exponential
which one use a lockdown to stop. Or if looks much worst than that, in few days, additional social distancing might be needed. Or if much better than that within 5 days {unlikely} Sweden’s plan worked, and less than 200 deaths per million could happen period of another month.Or terms of 1/2 year it’s unlikely death million will be less then 200 per million. Sweden has 450 critical ill and unless Sweden has treatment which more successful than is typical [maybe better ways using ventilators or stuff like that} that number will result in more death being added without addition of new cases.
Italy has 2,635 critical ill but has 6 times Sweden population, so, per million close to Sweden.
UK has less critical ill per million, but has +5,850 new cases which is significantly more than Sweden or Italy per million. And would be a lot more new cases {it seems obvious without lockdown and more death].
But I think UK cities can get more out lockdown and sooner than compared to areas of low population density- or failed idea getting herd immunity would allow more “herd immunity” in cities.
Though don’t know how such immunity “works”. But it seems like Sweden was a guinea pig, Italy appears willing to be one. And assuming experiments work, UK could leave lock down in about 2 weeks, assuming it does not want to join the experiment as quickly.
But regardless of how UK government takes “action” it will done in about 2 weeks.
But in terms long term problems related to it, the important questions should answered.
And maybe in terms other global regional problems with virus, those important questions can answered
quick enough.
Milord,
Good to see that infection rate is gradually falling, thanks for these reports. With respect to Ferguson – didn’t he talk about large outside gatherings as sport events? Your example is inside gathering, supposedly much more dangerous. As far as I can see your recommended strategy would be take back control over the virus now (through strict quarantines) and then employ South Korean approach? What concerns me is if ‘herd immunity’ is fool’s hope that means South Korean approach has to stay in place permanently. No sport events, no concerts, no church gatherings (Apocalypse now?). And total government control over activity of the citizens.
“What concerns me is if ‘herd immunity’ is fool’s hope that means South Korean approach has to stay in place permanently. No sport events, no concerts, no church gatherings (Apocalypse now?). And total government control over activity of the citizens.”
Well probably not a fool’s hope, I say instead it’s working, question is how well is it working, and how long does it work. If really crazy about it, you could try storing a lot antibodies. But don’t know antibodies in blood have anything to do the surface of throat which is infected. Though it seems to me you have answer, why there is antibodies in the blood. But anyhow, it seem the S Korea is “doomed” unless they get a vaccine, but vaccine seems same problem as herd immunity.
But S Korea not “doomed” because they have time, they could find solution, AND/OR they could “lock up” those most likely to get seriously ill and die from virus, and serious illness and death is low for normal healthy population. Or find out who is seriously affected, and isolate them. And other though people it’s less of problem. Of course there other fears, like repeated exposure over the years can add more problems. But we seem to somewhat know, that serious illness could/probably cause longer term health problems. In that case, S Korea looks like only winner, well, Japan doing ok, and so far, so, is India.
Japan is doing bit tighter lockdowns right now, India implemented draconian lockdowns few weeks ago with 4 hour notice to wider population. The whole point is how to avoid that, keep economy more or less running and at the same time keep virus spread under control. And here South Korea and Taiwan are shining examples. Surprisingly Sweden too, though they’ve got much higher rate of deaths per population. But one Swede elaborated on that – initially they did awful job in protecting care homes what now pushes mortality much higher. Not sure though if this explanation is reliable.
From a comment posted on the Tony Heller site, “Things are going to get better”
https://www.youtube.com/watch?v=bfN2JWifLCY
This interview with one of Sweden’s and Europe’s more respected medical professors, is worth the 34 mins run time.
I would also recommend reading Tony Heller’s updates which is where I found the Swedish clip. The comments section is a rich hunting ground for worthwhile additional information.
We still have no reliable test for Covid 19 antibodies.
–From a comment posted on the Tony Heller site, “Things are going to get better”
https://www.youtube.com/watch?v=bfN2JWifLCY —
I listen to 1/2 of it. Roughly I agree with what he says.
But .1 Percentage is higher than I think it is. But he didn’t give a time period
1 percentage of US is 3.2 million, and .1 is 320,000 but I assume he giving a high number,
so he is not wrong. And he could be assuming no mitigation is done. Sweden is doing lots of
mitigation. Sweden has pop of 10 million, 1% is 100,000 and .1 is 10,000. And currently Sweden has 1,540 deaths. And I think fair to say if Sweden got 6000 deaths, the public would change it’s mind.
And I said above I think Sweden will get 200 deaths per million, which is .02 percentage.
But I am giving upper limit, it’s just what think is likely. I would not surprised if .05 percentage
or 500 per million. I don’t think anyone would say Belgium with 490 deaths per million will have less than 500 per million. Though it’s possible Belgium has miscounted it’s 490 per million number.
But no sane Belgium politician would claim without have good evident that 490 number could be miscounted. But months later, it might be corrected.
But Sweden only has it’s buses 1/2 full and has no subways, that a significant mitigation vs New York City
or London. Plus Sweden isolated it’s vulnerable population- which is what Governor of Florida did and Florida has less strict lockdown type stuff. And Florida has 38 deaths per million and Sweden has 152 deaths per million, and if Florida maintains it’s isolation of vulnerable population, it probably will not have as much as 152 deaths per million. I think Florida warmer weather is a mitigation. Or people aren’t stupid if they retire to Florida- despite the hurricanes.
I think the doctor listens to, too much CNN.
Mr Baikie makes a number of important points. Like him, I hope that Sweden’s limited-lockdown strategy works: at present, its rate of increase in deaths is among the fastest that I am recording.
Also, now that the lockdowns have worked in those countries that implemented them (in Britain, for instance, the health service would have been overwhelmed if the country had not been locked down), we can learn from both South Korea and Sweden and begin to end our lockdowns.
However, it is not yet possible to compare total deaths as a fraction of population between different countries, not least because the infection began at different dates in various countries, and one must allow for this before making direct comparisons.
Milord,
I hope that Sweden’s limited-lockdown strategy works: at present, its rate of increase in deaths is among the fastest that I am recording.
Death is one counter. Another is however situation in hospitals – lockdowns were aimed predominantly to save hospitals from overloading. Looks like such overloading is not happening in Sweden. This country is truly big experimental zone. Very different strategy than South Korea or Taiwan but may be equally efficient in the longer run – no-one said that there is one and only one canonical strategy for everyone.
Great interview, indeed.
You probably need to go to cartridge style respirators to actually filter viruses. Probably explains why so many front line personnel have been infected.
The n95 masks are probably fine so long as you don’t wear them too long. But pretty soon the droplettes the mask captures are going to evaporate as you breathe, freeing the viruses to travel thru the mask.
Somebody explain the plan here. The virus is so infectious that one infected person can generate a global pandemic. So, since we can’t ever eradicate the virus completely, we are thus doomed to practice social distancing, with its inherent crippling of economic activity, forever.? Is that the plan? Like, nobody’s ever going to kiss anybody ever again, let alone eat in a restaurant or go to hockey game?
Come on, come on, come on. The virus exhibits different symptoms in different people, and most people either don’t get sick or get a mild illness that clears up. Some people die, but most of those are very, very old. (Do you know anybody who is eighty? I know quite a few, and none is able-bodied, and most are near death.) At a certain point we’re just going to have to sacrifice the people who are vulnerable to death from COVID-19, in the same way that we sacrifice an expected number of people to death from motor vehicle accidents. That’s the inevitability here.
How is death from COVID-19 worse than death from anything else that kills old people every day?
Ian C., Your tone of impatience is very understandable to me. After all, the very title of the current head posting indicates disappointment in those very experts whose advice we’ve been effectively following through the whole lock down or business shutdown scenario in most countries. At the same time, there seems to be a general presumption with many of the commentators here (the head poster, Lord Monckton, included) that it is a *good* thing to have followed the official advice, because it is all so appropriately precautionary you know!
It appears that in the face of any virus whose spread is seen as ‘novel’, some sort of arbitrary and/or extreme lock down is now required, with other costs or other increased risks being no object.
Probably the worst aspect of some of the comments here, I think, is all the hand wringing over how much *more* should have been done so much *sooner*. Granted, China shouldn’t have lied about the start of it, shouldn’t have covered up or silenced it’s own health professionals. At the same time, if the ‘risk vs benefits’ discussion could have started sooner, maybe the biggest potential benefit of that would have been that the response could have been significantly more *deliberative*.
I mean, say, talk over what to do, maybe even take time out for a whole week or ten days of global debate on the more disruptive kinds of measures contemplated (sacrilege, I know, people debating whether to embark on draconian measures). Wouldn’t that have been a better approach, instead of just whaling away with great sounding, but horrendously socially and fiscally disruptive, ‘business shut down’ measures?
In response to Mr Coleman and Mr Blenkinsop, lockdowns were necessary because otherwise hospital systems would have been overwhelmed, and most governments were rightly unwilling to allow that to happen.
Now that the primary purpose of the locdowns – preventing the collapse of hospital systems – has been achieved, the lockdowns can be, and are being, carefully dismantled.
But it should not be assumed that this virus is harmless just because it chiefly kills old people. It remains dangerous, and we are going to have to be rather careful until a vaccine is found.
And if no vaccine is found?
Christopher
You said, “… lockdowns were necessary because otherwise hospital systems would have been overwhelmed, ….” That was the assumption that rationalized the lockdowns. However, where was the public discussion about whether social distancing alone might have been adequate?
I take issue with several assertions in this post by Ian Coleman
First “that people over eighty are not able -bodied and most are near death”
Well some are but not all are so decrepit
I am eighty- five with current blood pressure 117 on 67 with pulse 55 I can do fifteen push ups I do regular bush walks and can still run repeat sprints
Then we have ” most people either don’t get sick or get a mild illness that clears up” ( from the Covid -19 virus)
This naive idea that the corona virus is really just another form of flu which will only carry away the most health- afflicted geriatrics already near death is dangerously ill informed
First it is not only geriatrics who are health -afflicted Unfortunately chronic diseases such as diabetes , asthma and hypertension are prevalent throughout a wide range of age groups These diseases are considered to predispose sufferers to be at enhanced risk from Covid -19
Furthermore we have just seen a report on TV here in Australia of an Aussie medico working in NYC who was saying that this virus is producing some unexpected bad effects in patients not seen in influenza infections, notably vascular diseases including strokes and brain damage, and that in early middle age people.
There is so much we do not know about this virus eg does surviving it provide immunity and if so for how long?-or Can people be reinfected?
and if the answers are respectively No and Yes then the so -called “herd immunity ” argument starts to look questionable.
Is it in fact transmissible through aerosols? Initially it was said not to be but more recently some scientists are now not so sure
Last “do we sacrifice an expected number of people to death from motor vehicle accidents as Mr Coleman suggests?
I don’t know what the US numbers look like, but here in the state of Victoria in Australia we have reduced the annual road deaths from around 1000 to about 450 with now three times the traffic by a range of measures such as tough drink and drug driving testing and punishment, compulsory seats belts, mandatory vehicle safety changes, improved road design, and speed and intersection cameras
So we don’t just sacrifice people as suggested but at least here public policy is to work assiduously to progressively reduce road deaths both in their rate and absolute numbers.
Christopher – I agree with you on pretty much everything, other than the point about how we should let the virus go through society (herd immunity). Analysis of available datasets shows this is very infectious with an overall mortality about 0.5%. Weighted towards the older generations unfortunately for them. From Diamond Princess and also Italian death stats in hospitals. The corollary is that it has also spread very far and wide and obviously fast.
Now it is uncertain if any longer term immunity can be acquired. If it can we need to get minimise the time everyone is locked up. And if it can’t, then the question is ‘now what do we do ?’. We are just going to have to learn to live with it.
Either way, as Trump said, we can’t let the cure be worse than the problem, so we need to get everyone back to normal as fast as possible.
“Either way, as Trump said, we can’t let the cure be worse than the problem, so we need to get everyone back to normal as fast as possible.”
—
Effective antivirals is how it is ‘lived with’. Until we have these it is wiped it out with isolation, and kept out via borders, and the sure-fire and fail-safe practice of a quarantine period.
That way a traveler with CHICOM-19 fails, and not the economy and people in the country they elect to travel to.
In response to ImranCan, I too am in favor of unwinding lockdowns as soon as it is sensible to do so. However, the discovery that “herd immunity” may not be available to us is bad news. It removes the only credible excuse not to have lockdowns in those countries whose medical facilities would otherwise have been overwhelmed.
Unless a vaccine can be found, we are going to have to be careful with this particular pathogen. Notwithstanding the clamor from some commenters here for all restrictions to be ended, on the frequently-stated ground that this is no worse than the annual flu, the British data, from all three regions of the United Kingdom, show a sharp spike in excess deaths in the past two or three weeks – indeed, the worst such spike since modern records began 15 years ago. The spike is so startling that the Professor of the Public Understanding of Statistics at Cambridge has said that even he, who has seen everything and is not usually caught by surprise, was startled by it.
Anyone following our case-growth and death-growth graphs here would not have been thus surprised, for it is clear that this pathogen is a lot nastier than some had at first thought. It will, however, soon be possible to ease the lockdowns in most countries, since their primary purpose – preventing the healthcare systems and hospitals from being overwhelmed – has largely been achieved.
“the British data, from all three regions of the United Kingdom, show a sharp spike in excess deaths in the past two or three weeks – indeed, the worst such spike since modern records began 15 years ago.”
You mean the lockdown caused a spike? So we can’t stop the lockdown?
I live in France and, personally, I don’t pay so much attention to SARS-CoV-2 (coronavirus) numbers and statistics, as they’re obviously an approximation.
We all know by now, that neither the number of the coronavirus infected that are published (daily!) in France and the different countries mean a damn thing, nor the coronavirus deaths (equally published daily!!!) mean anything at all. They are both approximations, and I will let the experts decide as to what the numbers really are later, perhaps in a year or so, when they will have enough data to filter the garbage input.
Nevertheless, what *everybody* (well, almost everybody) believes, including WHO, is that the coronavirus is a serious threat to human life. Serious enough, to halt all normal social activity, including business.
Unfortunately, in France, the numbers don’t match with this belief. I don’t mean the SARS-CoV-2 numbers, no: I mean the global death rates do not show any threat at all.
What the global death statistics show is that every year there’re clearly two seasons of death rates: Summer (from April to September) and winter (from October to March). In France, summer AVERAGE DAILY death rates are around 1500 and winter they are around 1750. In other words, every year you have about 250 average deaths every day.
Of course, these are average season death rates, and they are *obviously* due to the “seasonal” respiratory infections. When you get into the details, every year, the pattern is identical: You have a peak that lasts two months, then death rates get rapidly back to normal. Sometimes, there’s just one high peak, sometimes there’re two smaller ones. The months that the peak starts depend probably on the weather and/or other causes, I’m not sure (I am not an epidemiologist, after all).
Here are the statistics of the average daily deaths per month for the last six years in France, including the latest (finalized) March-2020 numbers as given by the INSEE:
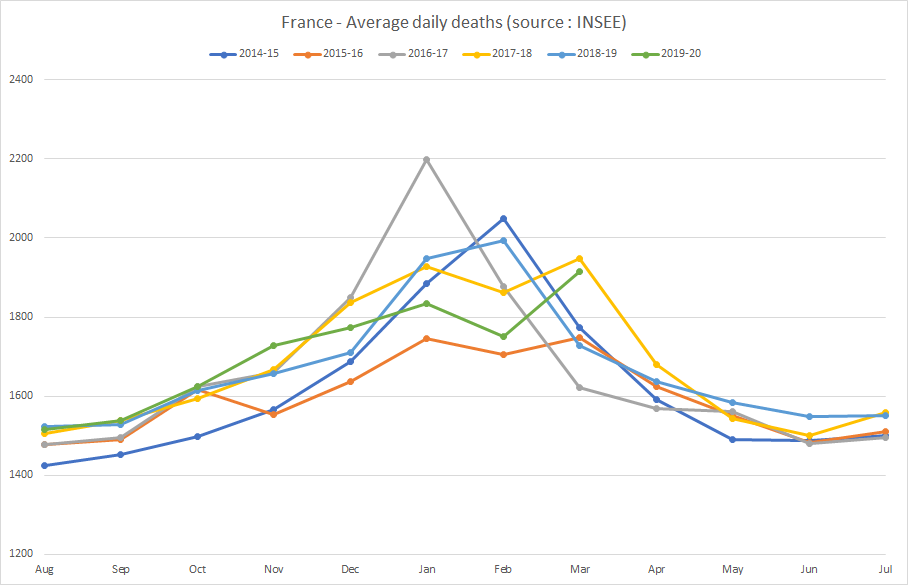
So, I repeat, when I look at these stats, I struggle to see how (or where) this coronavirus “disaster” is represented in the global deaths. Because it is not. There’s no trace of it!
What I see, is an average, predictable, “normal” death-rate picture.
Statistical fact: Every single year, 50% of the deaths in France are of people above 83 years old. Accidental deaths are negligible.
I wonder what the numbers in the UK are. But I doubt they are much different. 😊
Good comment.
The question is how does this progress? We don’t know unfortunately.
Thank you.
I agree that we should monitor closely its progress. Nevertheless, let’s bear in mind that March 2020 was (in France) the peak month.