Guest Essay by Kip Hansen

Warning: This essay is about a recently emerging concept being applied in medical research. In the course of the essay, it will become clear how this concept might cross over to the field of climatology. Those readers only interested in climate issues or the Climate Wars should move on to the next offering here at WUWT – this essay is not for you.
There is a new concept slowly emerging in the field of clinical medical research. It is called Minimal Clinically Important Difference.
Here’s the definition:
“When assessing the clinical utility of therapies intended to improve subjective outcomes, the amount of improvement that is important to patients must be determined. The smallest benefit of value to patients is called the minimal clinically important difference (MCID). The MCID is a patient-centered concept, capturing both the magnitude of the improvement and also the value patients place on the change. Using patient-centered MCIDs is important for studies involving patient-reported outcomes, for which the clinical importance of a given change may not be obvious to clinicians selecting treatments. The MCID defines the smallest amount an outcome must change to be meaningful to patients.” — Minimal Clinically Important Difference — Defining What Really Matters to Patients by Anna E. McGlothlin, PhD and Roger J. Lewis, MD, PhD
This concept can also be applied to outcomes [that] are not patient-reported but which are simply measured numerically – such as blood pressure, body temperature, blood cholesterol levels and body weight or BMI.
Note: The first literature instance easily accessible is Measurement of health status: Ascertaining the minimal clinically important difference by Jaeschke, Singer and Guyatt (1989) doi:10.1016/0197-2456(89)90005-6 — after the turn of the century one finds more and more frequent references to his concept.
Let’s look at some examples:
Body Temperature:
We take our “temperature” to determine if we are ill or not. When we were children, our parents may have used an oral thermometer to determine whether we were too ill to attend school – if we had a fever, we stayed home – if not, off to school. It is generally accepted that normal body temperature ranges between 36.1°C (97°F) to 37.2°C (99.7°F) – alternately: the typical oral (under the tongue) measurement is slightly cooler, at 36.8° ± 0.4 °C (97.5°F to 99.5°F), with normal generally considered to be 98.6°F (and so marked on your mother’s glass oral thermometer). Well, we see right away that the term normal body temperature is not quite agreed upon. Nonetheless, there are things about body temperature that are clinically well understood: oral or core body temperatures above 100.4°F or so (for persons teenaged or older) is considered a fever and an indication of something wrong – such as an infection — high-grade fevers range from about 103°F-104°F — dangerous temperatures are high-grade fevers that range from over 104 F to 107 F or higher. Fevers are not only indicators of health problems but they can be dangerous in and of themselves. Temperatures below 95°F are considered dangerously low, verging on life threatening as core body temperature continues to fall lower.
Example: Let’s say we were researchers and wanted to test a fever-reducing drug. Various treatments that are supposed to affect body temperature, to treat fevers, would be judged by their action of changing the body temperatures of the patients in a clinical study – measured by thermometer. [Aspirin, for instance, is considered a fever-reducing drug and is often prescribed for just that purpose — it is one of many non-steroidal anti-inflammatory drugs.]
This concept of Minimal Clinically Important Difference calls for the researchers to determine in advance what numerical amount of change will represent the Minimal Clinically Important Difference – the numerical amount that must be surpassed for the results to actually mean that patients’ health has been improved in a way that is important to them – to the patients, to the patients’ health, not just to the doctors, not just numerical/statistical way.
In our body temperature example, it is apparent that lowering a raging fever of 105°F by 0.5°F to 104.5°F (but no lower) – even though it is a 7% decrease in the above-normal anomaly temperature – may not pass the Minimal Clinically Important Difference test – 104.5°F is still a raging fever and the patient may not be clinically better off. If the treatment does not bring it down by what was pre-determined to be the MCID (in this case, the MCID might be to reduce the fever to a certain level) then the treatment is less than successful or the effect of the treatment is not significant. It does not matter that the result – lowered average temperatures of patients in the study by 0.5°F – was found to be statistically significant if the result itself does not meet the pre-determined, and correctly identified, MCID.
Likewise, one could look at various treatments that lower a study cohort’s average of some metric – like blood pressure. This is often an approach used by epidemiologists looking at large health databases.
High Blood Pressure:
Note: Blood Pressure numbers represent another science war – though a quieter one. For many years, doctors considered 120/80 to be ideal and anything under 140 to be OK but now the threshold for hypertension has been dropped first from 160/100 to 140/90 and now, with prehypertension defined as 120/80 to 139/89, to where maximums of normal have been set at 120/80 – what used to be ideal is now the maximum acceptable before treatment is recommended. In the UK, however, blood pressures are usually categorized as: low (90/60 or lower), normal (between 90/60 and 139/80), and high (140/90 or higher). A recent study says doctors have been over-treating high blood pressure in seniors and that seniors should not be treated until their BP exceeds 150. And on it goes, with advocacy groups (and drug companies) pushing for the setting of official limits low and evidence-based-medicine doctors pushing back.
Example: Doctors wish to test a new blood-pressure-reducing drug. The doctors carrying out the study will be testing the drug on men with High Blood Pressure (US standard) >140/>90. Before anything else, they should define the MCID for blood pressure for this cohort – I don’t know what it would be, but they would have to set it before the study is carried out.
Let’s just guess that the average systolic blood pressure (the higher number) for the cohort is 150. In a cohort of 1000 men receiving treatment for high blood pressure (HBP) the study finds average reduction in systolic pressure to be 5 mm Hg, lowering the average to 145. Is this a MCID?
Well, I don’t know – the study’s authors would determine this by comparing their result with their pre-determined MCID. (In my opinion, 5 mm Hg with HBPs of 150 or so would not bring any one patient relief from the symptoms of HBP nor improve their health in any important way.) However, the result may have been found statistically significant with a very small P-value – it may just not be clinically important.
[ An aside: There is one more thing about many of today’s medical studies that is amusing – there might have been some effort in the above hypothetical blood pressure study to say that while that 5 mm Hg might not be much for individual patients it would be significant in public health setting (and I know this sounds crazy – but this really is claimed quite often in epidemiological studies) because 5 mm HG times 1,000,000 people is a huge reduction in public blood pressure! Epidemiological madness. ]
We have established that the Minimal Clinically Important Difference must be determined before the study is carried out, as part of the study’s planning and design. This is logical as the researchers must know in a general way what measurement tools to use – glass-and-alcohol oral thermometers or high accuracy digital thermometers, for instance. Or whether blood pressures should be determined my nurse-operated sphygmometers or mechanical digital equipment. What measurement scales to use: tenths of a degree C or thousandths of a degree C. How many subjects they must have to determine results to that accuracy or scale. There is no need for high accuracy thermometers if the MCID is “reduces body temperatures to within 1°F of 98.6°F”. No need for high-tech/high-accuracy blood pressure measurement tools if the MCID is “reduction of systolic blood pressure by 20 or more mm Hg.” Researchers comparing actual results with a pre-determined MCID will then know if their results will mean anything important for patients – to know if they really have a meaningful, clinically important, result.
So why is this concept being presented here at WUWT?
· First, because a pre-determined MCID is a very interesting addition to the scientific method in general. Requiring researchers to define what magnitude or type of result is clinically important (or in other fields: physically important, culturally important, militarily important, environmentally important, etc.) [Note that MCID may not apply in basic research in which one is simply trying to find out what there is to find out.]
· MCIDs become part of the study’s findings — just like methods and study design – and thus can be peer-reviewed. They can be taken into consideration when colleagues review (critique or praise) the resultant paper.
· MCIDs make it much more difficult to inflate the value of a research finding by disguising its insignificance. MCIDs can greatly reduce the bloat of “nothing-found” research papers being published – and the endless follow-on studies to those “nothing-found” studies.
Once you get the concept, you’ll be able to spot studies that should have been held to a MCID standard – that might better have been returned to the authors by peer-reviewers with a note: “What was the MCID for this study? Do you think that your result passed your MCID test?”
What does this have to do with climate science? Could or should such a concept be applied to climate science studies? If so, which ones and under what circumstances?
I will give just one example, and then we can all discuss this in the Comments.
Take a quick re-look (or first look) at my recent essay “Baked Alaska?…”. This essay includes some results that might have benefitted from the MCID approach. The basic hypothesis presented about the climate in Alaska is represented by Mike MacCracken’s, chief scientist for the Climate Institute, statement along the lines of ”how long-term trends will play out in Alaska” which are claimed to have been dangerously warming.
This one image gives us all the data in one go (enough for purposes of this discussion):

Box (a), labelled 1920-2012, shows a long-term warming trends in 12 of 13 climate regions of Alaska, with the state-as-a-whole warming 0.9°C over the 92 year period. Box (d), labelled 1981-2012, however shows the entire state warming trend of only 0.1°C over the latest 31 years. The North Slope (at the top of the state) has a warming trend of 1.9°C over the same 31-year period. The climate region that includes Fairbanks, Alaska is shown with a 31-year cooling trend of -0.1°C.
Do you see where this leads? What is the Minimal Climatically Important Difference that we should be looking for in this data? Does Fairbanks’ -0.1°C 31-year trend meet a logical and scientifically supportable MCID for average temperature? Does the North Slope’s +1.9°C? Does it make sense to look at MCIDs for statewide annual temperature averages? Can a MCID even be set for annual average temperature alone?
Are there such things as Minimal Climatically Important Differences in climatology? Well, for Fairbanks, Alaska we find that despite 31 years of cooling trend their “# of frost free days” has increased by 50% since the 1920s (see the link Page 29). Now that’s a climatically important difference! The “fact” that the temperature has been trending down for a period long enough to be called climate disguises the climatically important difference of a significantly longer growing season – extremely important to this agricultural area – “one of Alaska’s premier agricultural regions and produces one third of Alaska’s agricultural products.”
Maybe climate science is spinning its wheels and wasting its time looking at all the wrong metrics….metrics for which one cannot define a logically and scientifically valid Minimal Climatically Important Difference. Instead, producing what Dick Feyman would have called “cargo cult science” – science aimed at supporting or proving one’s pet hypothesis instead of trying one’s darnedest to disprove it; spinning the narrative and the data to make one’s desired result look more probable, to make one’s itty-bitty “leans-my-way” result look strikingly significant.
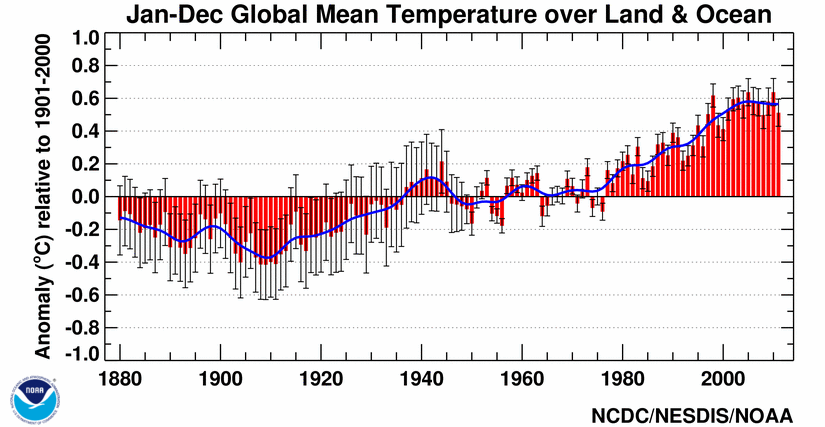
Of a few things I am certain – one of them is that a difference in a couple of hundredths (“hottest year on record”) or tenths of a degree Centigrade of annual difference in the derived “apples-and-oranges” metric we know as “Annual Global Mean Temperature Anomaly Over Land & Sea” does not, and probably cannot, pass any possible scientifically valid Minimal Climatically Important Difference test.
{kind=link}
In the same way, I would argue that nearly every political-boundary-based climate data set does not present any information that could lead to a valid Minimal Climatically Important Difference, based on the concept that political boundaries almost always comprise more than one climatic region (as in our Alaska example – for which 13 are proposed).
It does not help water-starved farmers in the Midwest to know that the farmers in the Central Hudson Valley of New York have adequate rain for their crops, thus keeping the CONUS Average Precipitation at an anomaly of zero against the 30-year average. Nor does it benefit the victims of Mississippi River flooding to know that their sorrow is not caused by climate change but rather just by a perfectly-historically-normal warm and rapid snow melt season hundreds of miles away. It is unlikely that small changes in annual average temperatures, measured and reported in single-digit tenths of a degree, are Minimal Climatically Important Differences but the differences within the same data set that reflect annual minimum temperatures, measured and reported in tens of degrees, might make the difference between wide-spread insect infestation with its resultant damage and freedom from serious insect damage – certainly a Minimal Climatically Important Difference. In this last case, the MCID might be whether or not it has remained continuously below -20°F for seven or more days.
I’ll start the comments off with this question: In all the issues that are considered here at WUWT – in all the numerical and statistical presentations of findings here, on other climate science sites and in the climate science journals-of-record – what type of results might inform science better if the concept of Minimal Climatically Important Difference was used in study design and results evaluation?
# # # # #
Macro or Micro? While this photo looks like it could be some crystalline growth on a flat surface, looking a little chaotic with its resemblance to the Mandelbrot Set, it is actually: “Macro: Cumulus clouds over the South Pacific Ocean (Image created by Jacques Descloitres, MODIS Land Rapid Response Team, NASA/GSFC, additional image processing by Stephen Young.)”
# # # # #
Author’s Reply Policy: My father was a doctor, an M.D., a pediatrician – I am not. The medical examples are written from a general public perspective. If there are medical errors – please inform, but do not blame. I use them only to make a point about MCID.
I am not particularly interested in climate science or the Climate Wars – my focus is more on science methodology, scientific ethics and science journalism, its use and misuse. This essay is about the concept of pre-determined MCIDs and their importance as an additional research method or tool – bridging the concept from its current use in clinical medicine to other fields – in this case, climate science. I’d like to hear your views.
# # # # #
WC Litzinger,
SciMag is putting their spin on it. But they don’t like the way it came down. Here is a different view.
Your link seems to be to an article in the Daily Caller that deals with Sen Inhofe. Was that your intent?
With the exception of an exceedingly rare but probably very serious condition called Malignant Hypertension, high blood pressure HAS no symptoms. It is correlated with a bunch of undesirable things, but for the most part causation is at best hazily defined. There may well be another, undiagnosed, condition that is causing the hypertension and treating the hypertension is may be, at best, cosmetic.
That said, I agree that a 5mmHg reduction for any single patient is of dubious value. Hoiwever, there is a related argument that might have some merit which is that if a treatment demonstrates an average 5mmHg reduction and if treatment is actually required the drug may have more impressive affects for some individuals.
Reply to Don K ==> All valid medical points.
The “the drug may have more impressive affects for some individuals” is perfectly true….this is where MCIDs are particularly useful…Does the treatment make an important difference for some individuals? Enough individuals to be still important in clinical practice?”
A HBP drug that is found to be extremely successful with 20% of those treated might be a clinically important breakthrough.
The concept can – should – also be applied to government policy.
A number of years ago I complained about the Congestion Charge in London for example. The claim was that it would reduce commuting times by 10%. That sounds a lot until you think that commuting times are 40-60 minutes for most people. Thus I was being “saved”, at great expense and inconvenience, four minutes each morning.
What exactly was I supposed to do with that four minutes?
Reply to Tim Hammond Jan 23 0243
This is another example where a solution is sold on the basis of a statistic which has very little to do with the problem. Problem in the case of London was the inordinate number of cars entering Central London, which caused much of the traffic congestion (not all – some was caused by the buses, and possibly most by the interaction of buses and cars).
Solution was to institute a boundary tax on entering Central London. I have checked the Wikipaedia article on the congestion charge, and find that there is no indication of any claim it would reduce commuting times by 10%. (There are mentions of improvements of from 30% in the early stages dropping to about 7% later). I suspect the claim was newspaper flummery, rather like the claim that the “Titanic” was unsinkable. What was intended was to improve the speed of buses and make their journey times more reliable (which it did), provide money for improvements to public transport (which it did and still does) and hopefully to reduce some of the pollutant gases from operation of motor vehicles – which it possibly does – there seems to be some disagreement.
In general, it can be called a success in its original aims.
If you did save four minutes travel time, you could always boil a couple of eggs and eat them on your way in, as long as the bus driver does not see you or the other passengers object. You thus improve your diet, to the benefit of your general health – the “Congestion Charge Is Good For You”
To answer your question, I would first have to assume that climatogly these past 30 years has been about science. It’s an assumption I find impossible to make.
Actually blood pressure could be a symptom of something else rather than its cause, as indeed is body temperature. We know for a fact that lowering an excessive body temperature or raising an abnormally low one is immediately beneficial to the patient, and therefore it is valid to address the sympton then go on to investigate the cause, although the body’s own mechanisms may well be able to do that inside the right temperature range. What is not so immediately obvious is that changing a high blood pressure conveys instant benefits (it may, but in the majority of cases it does not – this does not of course rule out long-term beneficial effects). Correction extreme blood pressure probably will stave off immediate effects, but the range of acceptable blood pressure readings (i.e. the numbers) is hugely greater than for body temperatures.
If we now consider side effects, we enter a different realm. The side effects of the odd aspirin or paracetamol taken for a few days at most and at ‘on the packet’ doses are unlikely to lead to significant side effects, whereas long-term or huge dosages might. The treatments for high BP on the other hand, are ‘rest of your life’ treatments, and for these, side effects almost certainly will manifest themselves, possibly with a severity that is more inconvenient to the patient, and perhaps even life-threatening. For example, if the HBP medication increases cholesterol levels, and that requires a statin to treat – a statin that in fact affects the efficacy of the BP medication, but also leads to raised blood sugar levels and a diagnosis of type 2 diabetes, for which the treatment raises cholesterol levels and further affects blood pressure, then one enters a sort of medical equivalent of ‘whack-a-mole’.
Moreover, we find that one or other of these medications might cause hives, increase of sensitivity to sunlight, muscle spasms and cramps of such severity that the patient is bedridden for months on end, blurred vision, mood swings, schizophrenia, suicidal thoughts, appearance of blotchy skin, growth of breasts and erectile dysfunction in men, loss of hair in women (and men, but many of them are baldies anyway), dizziness, joint pain, increased frequency of urination leading to severe loss of sleep – and one begins to wonder if the physician prescribing the drugs is not a greater hazard to the patient than the original symptom of HBP.
In climate science, the application of the ‘cure’ has equivalent debilitating effects on our lifestyles and economies, for no observable effect on the climate, so it not only fails the minimal effect criterion, but also the ‘do no harm’ one.
Reply to Daft Lassie ==> Not so daft…your medical points are very good — and enter into the realm of MCIDs and MCIDs for side effects (negative MCIDs?).
Juan Slayton, commenting above, can testify to the problems created by over-treating HBP.
If you are a medical professional, perhaps you can advise him.
This may be a version of the perennial idea that data analysis of outcomes should be done using a utility function. It’s been around a very long time, but never seems to be implemented to any degree. Presumably, people are wary of arguments over their chosen function (here MCID) in addition to all the other statistical problems?
Reply to basicstats ==> In clinical medicine studies the pre-determined MCIDs would be very pragmatic — does the patient feel better, is his condition markedly improved, both in the estimation of the patient’s doctors and the patient himself, does the patient think he is importantly improved?
The MCID is unlikely to be a result of statistics, though it would certainly show in the statistical results. But just because there is a significant statistical result doesn’t mean there has been a Minimal Clinically Important Difference achieved.
Climate Migration?
What is the Minimal Climatically Important Difference in TEMPERATURE sufficient to cause climate migration?
The alarmists claim: Climate-Induced Migration: A Looming Crisis
However, the FACTS, of people voting with their feet, show that:
Census: Florida’s population overtakes New York’s
Perhaps relevant:
http://www.numberwatch.co.uk/trojan_number.htm
Reply to CaligulaJones ==> Brignell’s Trojan Number is a spin technique to misrepresent the findings of a study.
Had the author’s of the study being misrepresented in this way used a MCID approach, their results would have been already evaluated against a pre-set concept of what would be a clinically important finding — and the spin-meisters would not be able to get away with twisting the miniscule insignificant findings into something else.
The MCID approach is very effective against these types of shenanigans.
Too true.
Before the Amazing Randi walked back his true beliefs on climate change due to the typical anti-science backlash, he was one of my personal heroes (still is, but a bit…tarnished).
He still created one of the better methods for dealing with folks with irrational beliefs: he lets THEM decide what the outcome is supposed to be, then creates the test they mutually agree upon.
Of course, when they fail, the blame games gets into high gear. See: number of excuses for The Pause. What are we up to, 40?
Sad that scientists are no more sophisticated than run-of-the-mill charlatans when it comes to making excuses.
Coming into this discussion late, so my comments in reply to people’s posts are probably irrelevent now, but there are moves to have all clinical trials registered prior to commencement and to have their methodologies and end-points (whether using an MCID or not) listed in advance. This is being done specifically to prevent the kind of statistical shenanigins that has gone on for far too long. In addition, registered trials must have their results published somewhere – even if they are negative – to remove the publication bias that exists.
This move is actually being supported by the pharmaceutical industry as they are actually the ones being fleeced by preliminary studies claiming positive effects that don’t hold up after they company has spent hundreds of millions on development. Throwing out useless treatments as early as possible is the biggest saving drug developers can make.
[We’ll get into re-defining normal to “create” a a whole new class of people who nee treatment in another discussion. That is about increasing the use of a drug once it is known to have an effect.]
Kip:
Great thought provoking post. Might be a good idea, but I’ve already got my Doc ticked off at me.
I was going for dendritic agate. Making my image identification only off a little, if we use a galactic system scale.
Reply to ATheoK ==> Dendritic agate would have been a good guess — I have seen polished slabs that look exactly like that – in fact, the local gem and rock club has their annual show in two weeks — which I will attend. Anyone near Cape Canaveral is welcome.
Kip, may you find the rocks you desire.
I’m collect rocks too, well sort of. I’m not a labeler, but I love to go rock hunting and bring back piles. The best stuff gets a window display, the good stuff gets clear glasses, the humdrum get buckets and pails and what’s left goes in the garden and borders.
I did come home with a granite slab from an old quarry. It was down a hill in the stream.
Nothing like sending kids into the yard to search for crystals (Herkimer, Amelia county, Arkansas), fossils and stuff.
I might’ve been a magpie, raven or a pack rat in a previous life… oooh, shiny, color…
And yes, I’ve seen large thick slabs of polished dendritic agate that one can get lost in, like flying a small plane through Jupiter’s clouds.
When I finished your essay and learned the image’s subject, I did go back and look again with a different viewpoint. Good stuff!
Reply to ATheoK ==> I once lived up above the Mohawk River in New York, and had Herkimer Diamonds in the creek behind our grist mill. My two oldest kids used to find them all the time.
Using the medical analogy, Specialist prescribed new drug for my arthritis, it worked really well, my arthritis settled right down. I went to GP and asked about the intense headaches, he looked up new drug on MIMMS. Blood pressure was dangerously high. No problem he said we will control that with other drugs. i questioned his opinion, whoops, bad mistake and not done. Something told me I had a problem here, so I rang the drug manufacturing company and asked their opinion, and told them what my GP said, they wanted to know GP’s name and phone number, about an hour later, I got an abrupt phone call from GP, saying take no more of arthritis drug, and don’t take blood pressure tablets either. What can I say DUHHHHHH!!!!!!, and he has the university degree. Would have loved to have been a fly on that wall. I have found out that my instincts are better than all the training, and that I saved my own life in this instance. Yes we should listen to the Experts (drip’s under pressure), but we should also listen to those little voices in our own heads, that says something is wrong here.
Reply to lyn roberts ==> Glad you got it straightened out. I grew up n a home with a PDR (Physician’s Desk Reference ) on the living room table — I never take anything without fully reviewing the full data.
The PDR saved me from the worst drugs of the 1960’s as well.
Reblogged this on gottadobetterthanthis and commented:
–
MCID application is a good idea. It will be useful if it is used.
Reply to Lonnie ==> Thank you, sir.