
Guest post by Jim Steele,
We must consider the unintended medical consequences of societal lockdowns hoping to prevent the spread of COVID 19. Unintended consequences are exemplified by past polio epidemics that left some of my classmates crippled. For the most severely afflicted, a polio infection required, not a ventilator, but an iron lung for children to breathe. The polio virus had likely been around for thousands of years, but in the 20th century severe epidemics began. Why?
In 1992 Dr Krause from the National Institute of Health published, “There are numerous examples of old viruses that have caused new epidemics as a consequence of changes in human practices and social behavior. Epidemic poliomyelitis emerged in the first half of this century when modern sanitation delayed exposure of the virus until adolescence or adulthood, at which time it produced infection in the central nervous system and severe paralysis. Before the introduction of modern sanitation, polio infection was acquired during infancy, at which time it seldom caused paralysis but provided lifelong immunity against subsequent polio infection and paralysis in later life. [emphasis mine] Thus, the sanitation and hygiene that helped prevent typhoid epidemics in an earlier era fostered the paralytic polio epidemic.”
Indeed, it was the more affluent people with higher standards of living that were most affected by polio epidemics, because their children were more likely isolated from milder strains.
As is the case for most rapidly mutating viruses, there will be various strains. Some will cause mild effects while others could be deadly. A strain’s virulence may depend on a person’s age and health. There are several strains of influenza virus, so vaccines are adjusted each year. There were 3 strains of poliovirus that were identified. Vaccinations eradicated two types and now groups like the Rotary are funding work to eradicate the remaining type. The observation that early exposure to polio viruses provided life-long immunity raises the question regards dealing with COVID 19. To what degree is sheltering in place preventing people from becoming naturally immune when infected with a mild strain?
The larger the population of naturally immune people, the greater the “fire-break” that prevents the spread of a more deadly strain. Just as social distancing minimizes the exponential growth of a deadly strain, it also prevents the exponential growth of naturally immune people. If so, perhaps a more targeted approach would be better. Our elderly population are the most vulnerable and are often confined to crowded facilities. People with compromised health conditions should self-isolate. We definitely need to minimize the spread to those vulnerable people. Perhaps designating one hospital to specialize on COVID and another for non-COVID medical care is a good strategy. Stopping medical care for a far greater number of people with other severe problems out of fear of spreading COVID 19 is not wise. And is it wise to quarantine everyone?
The fact that many people have tested positive for COVID 19 virus but had no symptoms suggest there are various mild strains that could naturally impart immunity. These mild reactions are primarily seen in people younger than 50 years old. However, once those younger cohorts gain immunity, they will be less vulnerable as they age.
Recently in the New England Journal of Medicine Dr Fauci wrote, ” If one assumes that the number of asymptomatic or minimally symptomatic cases is several times as high as the number of reported cases, the case fatality rate may be considerably less than 1%. This suggests that the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%) or a pandemic influenza (similar to those in 1957 and 1968) rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively.”
Dr John Ioannidis is a Professor of Medicine, of Health Research and Policy and of Biomedical Data Science, at Stanford University School of Medicine, director of the Stanford Prevention Research Center, and co-director of the Meta-Research Innovation Center at Stanford
He wrote an opinion piece A fiasco in the making? As the coronavirus pandemic takes hold, we are making decisions without reliable data suggesting we may be overreacting.
In contrast to Imperial College model suggesting over a million Americans could die, Ioannidis argued, “If we assume that case fatality rate among individuals infected by SARS-CoV-2 is 0.3% in the general population — a mid-range guess from my Diamond Princess analysis — and that 1% of the U.S. population gets infected (about 3.3 million people), this would translate to about 10,000 deaths. This sounds like a huge number, but it is buried within the noise of the estimate of deaths from “influenza-like illness.” If we had not known about a new virus out there, and had not checked individuals with PCR tests, the number of total deaths due to “influenza-like illness” would not seem unusual this year. At most, we might have casually noted that flu this season seems to be a bit worse than average.” The Imperial College and Ioannidis’s model will be tested soon, as American COVID deaths stands at 2,871 as of March 30th.
Nonetheless, it will be difficult to determine how effective a societal lockdown was if COVID 19 behaves like influenza. Flu infections dramatically drop beginning around April. Relative to seasonal warming, a lockdown may have a minimal effect. Perhaps by inhibiting the spread of a natural immunity, we may be setting the stage for another big wave of COVID 19 next year. These are questions must be debated.

Jim Steele is Director emeritus of San Francisco State’s Sierra Nevada Field Campus and authored Landscapes and Cycles: An Environmentalist’s Journey to Climate Skepticism
“Nonetheless, it will be difficult to determine how effective a societal lockdown was if COVID 19 behaves like influenza.”
We are still in flu season in Europe and we already have 14d of confinement to look at:

I see no reason to attribute the slow down in exponential growth to restrictions. The change started BEFORE it came into force, not after median incubation delay of 5 days.
You’re right. It was about the same even in China. Some behavioral change people made themselves or some other factor is at play. The outcome from Sweden should be interesting as they did not close schools for aged 16 and younger students.
I disagree. I do not know of any city environments where the coronavirus has taken hold and it has slowed down and plateaued without very strong defensive protocol, such as strong quarrantine and travel bans.
The Diamond Princess is actually an example of how quarantines work. Within a very short of time, 20% of the passengers were infected. And this was with a poorly done quarantine. Once a true quarantine was initiated of COMPLETE separation, there were zero new cases. Now 20% is certainly much greater than the 1% in the above article.
Also the article said .3% was the CFR on the Diamond Princess. This is completely wrong. The current case fatality rate is 1.4% with 20% of the infected still sick after 5 to 6 weeks. 15 of the 100 passengers still sick are in critical to serious condition. We can expect a likely case fatality rate of two to 3% for the Diamond Princess. And that is in consideration of good hospital care for 100% of the infected.
Yet there is an even better example. There was a single location congregation of over a thousand church members and over 80% became infected within a very short span of time.
Currently there are approximately 220,000 coronavirus cases that are complete. Buy complete we mean the patients are either healed or dead. In those complete cases, 19% are dead. Yes, it is true that there are many mild cases that never get listed on the record. But there are also many death, particularly in China that never get listed as caused by Covid-19.
Wait a second…if it is spread by people being in contact with each other, and we are not in contact with each other, how can this not be making a difference?
I think prior to lock downs, many people saw the writing on the wall and isolated themselves. That could have changed the curve somewhat prior to formal lock downs…in fact I know it did in my case.
If no one comes near me with the virus, I think I have a high likelihood of not getting it.
I think we all saw that many people were proactive, they washed their hands, stayed home, cancelled flights, etc.
Nicholas says “If no one comes near me with the virus, I think I have a high likelihood of not getting it.”
Indeed. But the question remains, Have you reduced the likelihood of getting a mild strain of the virus and immunity for life versus the deadly strain.
Based on the fact 95 % of recently confirmed cases have shown a mild condition, wouldn’t the better bet be to let yourself contract a mild form, unless of course you have a compromised immune system?
I have no spleen (car accident, 1982. The blood they have me to save my life also was how I got Hep C. Cured now. This is how I became a patient advocate)
Which places me at high risk of certain forms of pneumonia…but generally these are bacterial pneumonia’s…and I get regular vaccinations.
But having viral respiratory infections could make it easier for me to get a bacterial secondary infection.
But I am making the specific case to make the more general case that I do not understand the argument Greg was making. After all, quarantine is about the one way we have had for a long time to slow or halt the spread of diseases for which we have no treatments or vaccines.
I had considered for a brief while that it would be best to get infected early…like beginning of March, rather than later, when hospitals are overrun, beds and supplies running out or used up, staff overworked rather than geared up and waiting…
But this is a rapidly evolving situation, and as new information becomes available, I for one believe I have to be able to integrate that info and change my mind about…pretty much anything.
Making up one’s mind is about the surest way I have ever seen to shut down receptivity to new information.
In any case…One new idea that seems to be emerging is that this virus has a rather stable genome, while it had been more generally accepted up to recently that this type of virus was one that rapidly mutates.
There are other reasons to wish to become infected later, rather than sooner, which I find to be on more solid ground, in terms of what we can expect going forward. Such as the likelihood that the massive effort to understand and treat this virus will bear fruit at some point.
I expressed below some questions in my mind about the idea that there are known to be viral strains that are more or less virulent. It may be the case, but I have not seen the evidence.
I am no expert of the evolution of infectious diseases, but I did read Paul Ewald’s books on the subject many years ago.
I guess I should dig them out and reread them.
My general sense of it is that over time, infectious diseases have been widely thought to evolve towards being more benign, but of course that idea has been challenged.
Ewald seemed to argue, IIRC, that certain habits of people can cause evolution towards more benign or more virulent strains of infectious diseases.
Of course, if there is some solid evidence that there will be worse strains of the virus over time, then it becomes a complicated equation, which is really unknowable.
Predictions being hard and all that…
I am seriously considering going back to school and getting involved in some research, getting a more advanced degree. (I was “supposed” to have gone to medical school at Penn…but never went after being accepted) There are important questions we need answers to.
One questions has been niggling in my brain for years, and I have raised the subject here numerous times: What happens if someone ingests a subinfective dose of a pathogen?
Will the result be immunity?
Can we figure out how many virions will allow antigen presentation and antibody production, but not be enough to cause a systemic infection?
Can we measure such a dose of a virus, and ingest it for the purpose of inducing immunity?
Does this happen all the time, and explain why and how someone we are in close contact with can get a virus we never have had, and is known to be communicable, and yet not get sick?
It happens all the time…so…why when someone gets the flu in a house full of people, do only some people get it from them?
Is the number 95%? That seems encouraging.
Many reports list a higher percentage, but of course no one knows the denominator.
I think in balance, right now it is best to wait to get it.
It seems likely everyone will eventually be exposed, but this is just a WAG…who knows.
I would not want to get viral pneumonia…it sounds very unpleasant.
But…if you know how I can get me a mild case…please do tell. I would sign up for that right this instant.
There is no mild strain. Differences in mortality come down to immunity, infectious dose, and site of initial infection.
Dozens of medics are not killed by the flu every year.
SARS1 had a mortality rate of 15%(once you ignore BS chinese numbers) with a 50% death rate for over 55s. This obviously isn’t as bad (mostly because an initial nasopharyngeal infection gives you more time to raise an immune response before it infects your lungs, if you get a direct lung infection, like medics or SARS1, you end up with many more lung cells infected when the immune system kicks in, resulting is severe damage) The diamond princess appears to be a bad example, because much of the infection was likely due to fomite spread, rather than respiratory transmission, so people had better outcomes. South Korea estimates that there is only 10% asymptomatic patients and they do more testing than almost anyone.
Flu on the other hand is proven by serology to have a 80% asymptomatic rate. While Case fatality rate is 0.1-0.5%, mortality is 10 times lower at 0.01-0.05%.
With the best treatment and detection as seen in South Korea, the Mortality rate is about 2+/-0.5%. That triples if you run out of beds. This disease is 50 times more lethal than seasonal flu and the entire community has zero immunity. In my country (Australia) ICU bed run out when cases hit 40k, or 0.2% of the population infected, while peak infection if left unchecked would probably see 500K in hospital and 50K needing icu beds that only total 2000.
Just compare Norway to Sweden to see that infection rates per day are tripled and death rates are 10 times higher if you don’t enforce lockdowns.
” I do not understand the argument Greg was making. ”
You are probably trying to read more than what was written. I remarked that there is not change in the French case data which supports a change due to introducing restrictions. That is the evidence not an “argument”. I did not make any further argument about why that should be or what should be implied.
I posted Italian data below which does seem to show a clear effect with about the right timing to support causation.
I wish you the best in handling your personal predicament. You seem pretty aware and open minded so you are better equipt than most.
Hi Greg,
I had forgotten you are in France. For some reason I always think of Greg as an American name, but of course that is not at all the case.
I used the word argument in more of the legal sense…meaning “the point of view being offered”.
You are one who seems to make logical arguments, and I found myself reading your comment and not understanding.
Thank you for the kind words, and let me return the sentiment and hope that everything works out as well as possible for you and those close to you.
I must confess that there has been pretty much a news overload, and I was not specifically aware of what measures are or were taken in France, or any changes contemplated.
I am not at all sure how it might work there, but over here in the US, I do not think any one person could or did call for the present state of affairs. It seemed to be more of a sequential series of reactions to events as they happened.
Even as someone who has long thought a global pandemic was not just a matter of time, but overdue from an historical perspective…I never imagined what we are seeing now would happen, and especially not for a disease with such a relatively low death rate, compared to other deadly illnesses.
I think it is the number of people who need to be hospitalized and the length of time they need such care, that has been driving most of this. Even without any specific “cure” for a given disease, modern medical care has allowed for people to survive far longer than would otherwise be the case, by simply treating each symptom as it arises, and waiting for the patient to overcome the infection by their own immunity.
In retrospect, it seems surprising that leaders have chosen the responses they have chosen, rather than, for example, ordering a massive effort to procure PPE, create large numbers of beds in special hospitals commandeered from existing buildings, and requesting a volunteer army to care for the sick. Such an approach seems more like what what has always been done in all out wars in the past, and in certain public health emergencies also.
Some of the responses and actions taken by public health authorities makes no sense at all to me, and in many cases has been entirely counter productive and even ignorant and obtuse…such as the insistence here in the US that masks were of no value for individuals to protect themselves and everyone else, or the complete failure of imagination that allowed the virus to propagate widely without anyone being aware of the extent of the spread in real time until it was far too late to contain the virus.
Probably the single attribute of the disease that has caused such an ineffective response is the number of people who get the virus and spread it without showing any symptoms.
It seems like a long time ago that officials were attempting to screen for infected individuals by scanning people getting off planes with a thermometer, even after it became obvious that running a fever was not a common or early symptom of this particular disease.
We do a much better job of monitoring/guarding for invasive insects that we have done for determining if a known contagion was spreading through our populations.
Another such failure was allowing for possible treatments to be used without making an immediate and coordinated effort to make sure they were used in a way which would most rapidly allow a determination of efficacy using known methods to make that determination. At this point thousands of people have been treated with many different drugs, and no one has any objective data available, even after all this time, to discard or retain any of them, with one or two exceptions. Done properly, we would already know what works and when and could have every production facility geared towards manufacturing those particular drugs. I am not even sure there is a global effort underway to manufacture all of the main candidates for efficacy so there will be a large supply when we do have such information.
We need to know what works, when it works, how much it helps, and how much of these things we will need.
Instead, we have a civilization which is better at quickly making a huge supply of a popular doll in a short time, than at making a cloth mask, or even being able to agree that containing our oral and nasal secretions is important when a respiratory infection, spread by droplets from and to our mouths and noses, is sweeping like wildfire though our people.
Because of the high rate of transmission of covid19, it seems likely that just about everybody will at some time be exposed to it. Isolation at home is not intended to stop this, merely to reduce the number of patients who have the disease at any one time. This reduces the strain on medical services and hopefully allows more patients to make a full recovery.
I just noticed your name change, Bloke!
+ a bunch of pluses.
In every instance I look at on the W.M. site I see that the slow down starts AFTER quarrantines and travel bans.
Good article by Jim Steel as always, but consider, unlike the flu, there is very little herd immunity to this.
Let us consider the Diamond Princess
Correct current CFR is about 1.4 percent.
95 are still sick after five plus weeks.
15 are serious/ critical. So let’s take a WAG at 3 percent mortality, with 100 percent getting good hospital care.
( This is almost 10 times the articles .3percent)
For about 1/2 the group exposure time or more the passengers were in a simi effective quarrantine. Yet still in short order 20 percent were infected. ( 20 times the article assumption)
100 percent of that spread stopped when the passengers entered true quarrantine. In another group example 80 percent of just over 1000 members of a single congregation became infected with Covid-19. And this in less then 3 weeks. 1 percent infected is, IMV, absurdly low and incapable of developing herd immunity.
Even with quarrantine and travel bans this virus has proved capacity to overwhelmed hospitals. Treat it like a normal flu and the models would prove correct, and the economic damage would then happen just the same.
Currently 19 percent of over 220,000 complete cases, ( either fatal or cured) have died. So CFR is now 19 percent, and rising. That is with massive quarrantines and travel bans.
Yes, we know that at least one third are very mild or asymptomatic. We also know many thousands, especially in China, have died from this, and Covid-19 was never properly assigned responsibility.
I am still waiting for one major city to not enact quarrantine and travel bans, just to see how bad it gets. Consider that it got far worse in China then their ” official” numbers indicate.
David,
IOANNIDIS does give a lower case mortality rate for the Princess as other have subsequently died but his 0.3% for the total population is based on applying different rates to each age class.
Based on his assumptions U.S. population gets about 3.3 million people infected. Some say his estimates are too low but right now we have 184,487 confirmed cases.
He estimates 10,000 deaths and right now we have 3,756 deaths.
As Fauci’s article argues there are high numbers of asymptomatic or undetected mild cases, and he estimates 0.1% fatlity rate. When we get antibody tests we, will then be able to determine the fatality rates and the level herd immunity.
We can only wait and see
Thanks Jim, while I agree with waiting for more complete study for final CFR, this is manifestly more contagious and deadly then the common flus. Far more, as nothing has come close to overwhelming hospitals with such low numbers in such a short period of time. The Diamond Princess avoids all missed cases, and 20 percent were infected in under two weeks with Simi quarrantine. CFR will be 2 to 3 percent, maybe higher with the best hospital care.
Again, I know of zero instances of the curve bring flattened sans strong defensive protocols. And even with those protocols it takes two weeks to slow this bugger down. ( If it takes longer it is because testing is way behind the curve.
Their are credible estimates that in densely packed population centers, 80 percent would be infected within two months of normal behaviour. 80 percent of a church group of over 1000 was infected in two weeks!
All the known bad centers would look like a nice summer day compared to what would happen if this was left to run wild.
People would truly panic, and work would stop. The overwhelmed hospitals would be broken, vastly worse then the worse case so far.
China had no choice but to institute the Wuhan shutdown. ( Not to mention the rest of China) China did not destroy their economy over a few thousand cases.
Their numbers are FUBAR. They shut down all observations. They disappeared many reporters. The suffering people of China deserve to be listened to.
viruses can’t grow exponentially in the wild … humans do not not all live in the same block and interact with every other member of their city in the real world …
most peoples social circle is very small and smaller still is the circle that you interact with in a way that could pass an infection … (contact mostly) … and we already social distanced before whenever we got sick …
yes there is a tiny percentage of those with no symptoms who “could” infect others … of course if you show no symptoms its for 1 reason … a low viral load … and guess what else is low when you have a low viral load … your ability to infect others …
Lock down the sick seniors and everyone else back to work … let the seniors out in the summer …
Restaurants, salt and pepper shakes, table tops, counters, fast food counters, that package of ketchup handed to you fro your fries, self-serve checkouts at the grocery store, the gas pump handle at the gas station. The glass of beer handed to you by the bar tender, money change (bills and coins) handed you by the cashier…..
Then go visit your aging parents, your grand parents, the aunt who just got a round of chemo for her cancer…
duh.
you should change your handle to The Dumb Lord.
Evidence Dark Lord?
I have seen plenty of circumstantial evidence for asymptomatic carriers to readily be transmitting the virus.
Like…most people have no idea how they got it, and it somehow got all around the planet with no apparently sick people in evidence.
In fact every story I have read about known transmission pathways involves people spreading the virus either before getting symptoms, or without ever getting symptoms.
Nicholas McGinley
March 30, 2020 at 11:57 pm
I have seen plenty of circumstantial evidence for asymptomatic carriers to readily be transmitting the virus.
—————————-
Unintended Consequences?
A good part of asymptomatic carriers do not transmit the virus because of shedding of the virus… no active incubation.
The next wave many such will be first stage “infected”, and in the case of no immunity acquired, for whatever reason, at that point, higher chance they will go through the disease, in some cases at full, regardless of no underlining conditions.
The “slide bar” will keep dropping over time,
that of the high risk group will drop, enveloping and becoming “well mixed” and less discriminatory…including age;
and better the herd immunity now is not blocked and keeping up with it…
as else natural falling of severity of the disease over time and it’s periods will slow down.
My understanding is that for most of the world, apart from Italy and maybe Spain, no
much difference there, as the viral infection already done the most impact in consideration of herd immunity, or it will, as it goes through population(s).
Modern, “sterility” obsessed populations, have already being fully impacted, almost,
where further “sterility” modus operandi and social “barriers” gains no much.
The poor populations have no any chance whatsoever there… with blocking the herd immunity, even if some not so fully impacted yet.
Please do not take my word for granted, especially as I happen to be a non expert in this issue.
cheers
as a senior and one with a compromised immune system I made your suggestion last month. It seemed logical at that time. Certainly we would be better protected with more masques etc in the chemists and less problems in getting food delivered
as a senior with a mild heart condition and allergies I am sick of this crap. the cure is going to prove far worse than the disease. numbers are important when discussing what effect any actions are having. When 8,000 people die in America every day, 2.9 million a year from all causes we better start looking at just who is scamming who. 3,177,204 died worldwide of the freaking flu in 2018. Sanity will eventually have to prevail.
It happened in step-wise fashion.
First schools were closed if a single student was found to have been in the building while he or she had the virus, and the intent was to disinfect the building and reopen it in a few days.
Should they not have done that?
Then a sports league cancelled (or suspended) their season when a single player was found to have the virus.
Should they not have done that?
Then a concert here and there.
Then a large operator of amusement parks.
Then a whole school system.
Then entire businesses shut their doors when an employee was found to have been spread the virus.
Should the owners and operators responsible not have done those things?
Then another sports league, then borders closed and flights from affected regions prohibited on an ever widening basis.
Should that not have been done?
Which particular action was unwise, or wrongheaded (maybe all of them?), which assessment of risk or liability was poorly analyzed?
At this point some people are calling certain politicians accessories to murder for not acting sooner, when those same people were ignoring the threat at the time in question, and criticizing that same leader for the early actions that were taken.
And simultaneously, other people refuse to believe that anything out of the ordinary is or has occurred.
People who know nothing of medicine or pharmacology are proclaiming themselves experts on new drug approval, and calling for discarding the principles and methods that have allowed us to keep large numbers of people from taking unsafe and ineffective drugs that cure nothing.
I can cite an single person in the hospital which may be very indicative of what our main problem is here: In Australia, a young astrophysicist (who is a research fellow at a large University) is in the hospital after getting four magnets stuck up his nose while trying to “invent” a way to keep people from touching their face.
That is our problem.
The Dark Lord – March 30, 2020 at 8:37 pm
Dark Lord, ……. Both Joel O’Bryan and Nicholas McGinley “jumped on” your comment with both feet, ….. but neither you, nor them, mentioned one of the most prominent “pathway” which flu viruses take advantage of to infect the general population. And that “pathway” is the Public School System.
To infect the homes and neighborhoods for 50+- miles around, ….. just send one (1) child to school with the flu or flu symptoms …… and within 3 days there will likely be dozens of children, parents, etc. …… also infected.
So, from September thru December, ……. the schools are breeding ground for flu transmissions. They were “slow-on-the-draw”, ……. but cities and State finally closed the schools, ………. When they should have been the 1st things closed down.
I am about the only one who has mentioned schools, unless I overlooked something.
“They have subways, and everyone uses them…plus DeBlasio kept schools open long past when he should have closed them.
Schools are germ factories, and kids are germ fountains.”
https://wattsupwiththat.com/2020/03/30/unintended-consequences-polio-and-covid-19/#comment-2951706
What is the difference between having a discussion and “jumping on a comment with both feet”?
I only stepped lightly with one foot on tippy toe, with slippers on.
Jumping on something with both feet sounds rough.
I said nothing rough.
I have not seen anyone disputing that there is symptomless transmission since the opening days of our awareness of this whole thing.
It may be one of the most distinctive hallmarks of this novel virus…that it can be spread readily by people who have no symptoms, or such mild ones they are not noticed.
It seems more likely though that the entire phenomenon of transmission of diseases by people who themselves are not outwardly sick, has been overlooked or minimized more than warranted, for a range of illnesses.
Typhoid Mary never believed she was making anyone sick, even while she left a long trail of dead bodies in her wake wherever she went.
Amazing story by the way…cognitive dissonance on steroids.
She was immune to the bacillus, but carried several pounds of it in her gallbladder.
She infected at least 51 people, and is suspected in hundreds more though it could not be proven since she began to change her name with every new job.
In every place she worked as a cook, within days to weeks of her becoming employed, people became sick and some died.
Twice she was locked up.
Her case went to the Supreme Court, which refused to release her.
Looking at the Italian data (see daily new cases) this is exactly what I thought :
https://www.worldometers.info/coronavirus/country/italy/
BTW, there seems to be a (more or less) week long period in this data.
The first week maximum appears one week after the Italian lockdown (March 8).
Two other two waves appear, one 2 weeks after the lockdown and the last 3 weeks after the lockdown.
Roughly the same weekly waves appear in the French and Spanish data.
Is this a simple coincidence or perhaps linked to the average incubation time or … ?
Any though ?
The first week maximum appears one week after the Italian lockdown (March 8).
Two other two waves appear, one 2 weeks after the lockdown and the last 3 weeks after the lockdown.
According to the Hubei data, the recorded cases peaked about 12 days after the lockdown. This would seem to make sense since the incubation period is about 5 days while the more serious symptoms appear a few days after that.
I can’t give a definite answer to the double/triple peaks in the Italian data but is is possible that while cases are declining in one region (e.g. Lombardy) they are increasing in another?
According to the Hubei data
I’d take any data out of China with a large dose of salt given all we know about their lack of data integrity (to put it nicely) in regards to this virus.
Speaking of the numbers out of China, this is the second article I’ve seen on this subject.
https://www.wsj.com/articles/chinas-coronavirus-count-excluded-infected-people-with-no-symptoms-11585650226
“but is is possible that while cases are declining in one region (e.g. Lombardy) they are increasing in another?’
Certainly, yet testing being way behind the curve, verses good testing can account for many aberations in the data.
A column at the WM site of daily tests would be helpful.
Thanks,
It’s good to look at the whole from time to time. It’s nice to see that there are still people with that capacity.
Very informative and even eye opening. Will share with my LINE community in Thailand. Thank you very much.
ขอบคุณมาก
The trillion dollar question is how long COVID19 immunity lasts. Unlike polio, the corona viruses that cause about 20% of colds create an immunity that only lasts months. Without knowing this, it’s impossible to know what the correct strategy should be …
The expectation that I keep hearing is that mutations will make the virus less virulent over time.
Just been reading posts from an expert group on LinkedIn which is tracking different strains around the world. Very interesting stuff. Apparently there are eight identified strains so far; the mutations are small and, apparently, do not make the virus more deadly.
However, identifying each strain allows epidemiologists to follow the routes taken by the infection. So, for example, they have determined that the Covid infection on the west coast originated in Washington, whereas east coast patients have a strain that came directly from China. The information they are accruing is fascinating and, apparently, is being used to help develop a more efficacious vaccine.
I think the prevailing view is that there are many strains of multiple common cold viruses, hundreds in fact.
We likely do have memory cells for cold we have had, but there are a lot of them.
This would explain why kids get a lot of colds, older adults very few of them.
I used to get them all the time 45-55 years ago, now almost never. Cannot recall when i had one last…but it was when I went up north from Florida for a Holiday and there were kids running around.
I’ve not had a decent cold in years!! I did have a mild bout of ‘flu two winters ago which was the first in a long time.
Mrs N was reading an article somewhere today that suggested that this beast appeared to be remarkably stable for a coronavirus which ought to help the search for an efficacious vaccine. The cynic in me wondered if that might lend credence to the (conspiracy) theory that it was manufactured!
I can confirm Jim Steele’s theory about polio. Three of us caught it about age 7 (skinny-dipping in a local stream, or so the theory went!). I ended up partially paralysed for a month and with one leg a half-inch shorter than the other, the other two had something similar. One wore a leg brace at least into adulthood.
In those days it was known as infantile paralysis.
Yes, we have particular immune cells that remember.
A blessing of the current situation is the rise of Ninja Nerd Zach Murphy YT channel. He has great postgraduate level medical science lectures. On point, CoViD-19 and an eight episode Immunology playlist.
Yes, we have particular immune cells that remember.
A blessing of the current situation is the rise of Ninja Nerd Zach Murphy YT channel. He has great postgraduate level medical science lectures. On point, CoViD-19 and an eight episode Immunology playlist.
the corona viruses that cause about 20% of colds create an immunity that only lasts months
=========
Why would the immune system work that way? Isn’t a more reasonable explanation that there are a large number of different cold viruses? As a result children always seem to have a cold, but adults less and less as they age.
Because children gather together in confined spaces, called classrooms & when not in classrooms, are in close, physical contact with each other. Noticed how they, and their parents, all get coughs & colds every autumn, as they go back to school after the summer holidays?
I looked it up, and it seems to be accepted that there are over 200 circulating virus strains that cause common colds…most are rhinoviruses, about 1/3 corona viruses, and some are adenoviruses…with some others mixed in for good measure.
And many strains of each of them.
The immune system is a high cost feature of physiology. It has to be a measured response. In a likewise manner we don’t use a bazooka to kill a fly in the house or keep hundred cans of fly killer on hand in case we get an infestation. Our immune systems have been fine tuned over millions of years to generate a limited response and then sleep with one eye barely open.
MikeP
March 30, 2020 at 6:32 pm
————————
The question about how long the immunity lasts depends on what you think immunity is.
Immunity to infection or immunity to disease, so to speak.
In general term mainly immunity means immunity to the disease, the immune response of the immune system to the infection.
When you were a baby or a child you were vaccinated, given injections which helped your immune system to rump-up and have the proper efficient response ready to go prior to a possible infection.
Your immune system does not forget, that immunity last for all your life… but does not stop or prevent infections… just prevents the disease or lowers significantly its impact.
When immunity is gained, the immunity response is always ready to go at the first notice or first “alarm bells”, and in the case of mutations it upgrades accordingly in it’s own over time.
So if you get immunity to COVID-19, it will last for life, but you still are subject to other infections from COVID-19 over time through the cyclic rounds, with possible symptoms and some “light” impact… generally speaking.
The seasonal cold flu happens due to combination of factors like virus shedding ( dormancy – hibernation) and wear and tear of the organ tissue that is subject to such infection, and not because of the loss of immunity.
The way COVID-19 “looks” thus far, it seems like it is going a be around for quite a good long while.
Cold, you know, wear and tear, cold flu… corona viruses cold flu…
It is the wear and tear that triggers a burst of virus and the activation of the incubation period from the state of dormancy or hibernation.
Oh well, the main point, regardless of what said or claimed in all that above;
The immune system does not forget,
immunity gained lasts for life…
does not prevent infection though… and it will adjust over time to mutations.
cheers
“The fact that many people have tested positive for COVID 19 virus but had no symptoms suggest there are various mild strains that could naturally impart immunity.”
Or, just possibly, as has been stated publicly by at least two medical experts, the earlier test (modified use from the test for the SARS virus) had an excessively high false positive rate, making it near useless for tracking the true spread of the disease. It just may mean that some of these people have been exposed to SARS, have an acquired immunity to it, and have had no exposure to WuFlu. Or possibly that they have had no exposure, and have no immunity to either SARS or WuFlu. Or that ambiguous test results were applied to force a quarantine on a individual in an abundance of caution, or to generate a worst case, upper bound public health statistic (guess) while scrambling madly to contain and manage an epidemic.
Undoubtably, both milder variations and cases of natural immunities exist. At this point, detecting signal from noise just isn’t possible. Toward which alternative shall we fail: too cautious, or too careless? Or shall we wait for more reliable data?
I am impressed with the model from IHME (https://covid19.healthdata.org/projections Dr. Christopher Murray) as mentioned by one of the President’s task force physicians. It seems to be similar to the one the government is following, and much different from the models (Ferguson, et al) based on Spanish flu, but still quite grim.
SARS?
No SARS circulating.
Yes, SARS is circulating. The official name of the virus that causes COVID-2019 is indeed SARS-CoV-2
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it.
The WHO didn’t want to scare the people who would be scared of it.
Greg is correct. It is the SARS-CoV-2 virus, the name of the epidemic the WHO gave COVID-19.
Read more carefully. He did not say SARS Co-V-2.
He said SARS, and was talking about Wu Flu in the same sentence…
SARS refers to the strain that infected people about 16 years or so ago then went away.
SARS is not SARS Co-V-2, it is SARS Co-V-1.
SARS is NOT SARS Co-V-2. Wu Flu is SARS Co-V-2.
-d is saying he believes that the original SARS is still around.
By the way…they are not very closely related, phylogenically:
From what I have read, this strain diverged from Bat corona virus 20-70 years ago, and the divergence of the original SARS virus was even further back.
But there does not appear to be only one opinion on the exact points of divergence, as a search will turn up several variations of these:
The way I understand it, SARS and MERS are also Corona “relatives” (maybe why this one is ID #19) with similar structures. Once in the environment, they don’t go away, but the population does develop immunity, so, indeed it is not circulating. The test used in Asia and the EU was developed from the test created on behalf of W.H.O., previously used to detect SARS. For WuFlu it is a “better than nothing” screening tool, but with a high false positive result.
I am quite likely and willing to be corrected on the details, but I’ve used up my acronym quota in just a few sentences.
The 19 is because is was isolated as a novel virus in 2019.
Thanks. That makes some sense in the context of a 2019 outbreak. My understanding is that SARS, MERS and WuFlu are all considered “Corona” variants because of their electron microscope structure and similar (perhaps zoological?) origin. I don’t have a sense of how they are officially designated as they are isolated, except that CO seems to come from COrona, and V is either from Virus or Version. Assumed that ID means identification number. I’ll take it either way, but I’m on my daily acronym allowance again.
It’s been easy to miss thanks to a sleight of hand in giving a name to the *disease* that’s different than the name of the virus, but the “Wu flu” IS SARS.
The name of the virus determined by the organization of virus taxonomists is:
SARS-CoV-2
which makes the old SARS into
SARS-CoV-1
The WHO didn’t want to tick off an unnamed Asian country that starts with a C and ends with hina.
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it
The WHO leadership is controlled by the Chinese Communist Party. Yes. It really is.
Probably like the UNFCCC as well.
Before we had this new virus, everyone just called the other two SARS and MERS.
So it is not correct, in my opinion, to say Flu Wanhu is SARS.
Yes and no. the “Wu Flu” is a result of a SARS virus (SARS-CoV-2) so it is technically correct to call it so. However, while related, it’s not the same strain as SARS-CoV-1 (the original SARS) so could be confusing to the uninformed to use the same name (SARS) to refer to the two.
I think if the same name is used to describe two things, that is confusing even to people who are well informed.
So, Mr. Endicott, it’s better to confuse everyone by giving the disease a brand-spanking-new made up name, “COVID-19”, *after* the world’s taxonomists correctly identified the virus as SARS-CoV-2?
We use “flu” to refer to new and possibly fatal influenza strains regularly without significant confusion. This SARS du jour is SARS-2, or maybe SARS part deux. Son of SARS. Wuhan SARS, SARS-Wuhan. Or, since there isn’t any SARS-CoV-1 in the wild and hasn’t been seen since 2004, just SARS could be used conversationally without much danger of significant confusion.
As with all words that have multiple meaning, it entirely depends on the context being used
So, Mr. Endicott, it’s better to confuse everyone by giving the disease a brand-spanking-new made up name
1) ???? I don’t think you mean to be addressing me with that comment as I’m not the one advocating for “giving the disease a brand-spanking-new made up name”
2) all the disease names are “new made up names” when they are first discovered. SARS (the original) was a ” brand-spanking-new made up name” back in the early 2000s.
3) this is a SARS virus, so I agree that calling it a SARS virus is perfectly OK, given proper context. It’s also not the same SARS virus as the previous one, so referring to it differently is also perfectly OK, given proper context. After all not all Flus go simply by FLU, we have had Swine-Flu, Bird-Flu, Spanish-Flu, etc. sometimes they’re referred to by names that don’t include the word Flu, such as H1N1 (or N1H1 if you are Joe Biden). The point being there’s more than one way to skin a cat, and more than one way to refer to a disease
It is fine with me if we call it a ham sandwich.
Who knows how to get a mild case.
I’ll buy dinner for whoever can say.
Hell…a month of dinners, anyplace that has steak on the menu.
COVID-19 is the name of the disease, aka WuFlu. It stands for COronaVIrus Disease-(20)19.
The virus which causes the disease is called SARS-CoV-2.
It’s nice that in general projections are becoming less severe. Dr. Murray has deaths peaking in the U.S. on April 15. I’m hopeful that it’s sooner than that, maybe this week.
I’m impressed with the *graphics* but pretending you can fit a complex model like that to such short sample is BS.
There is ZERO information in the little data present about how high it will go and when it will peak. Whatever the parameters are which are being used, they are coming form elsewhere, not fitting to the data. Probably simple WAG and gut feelings.
Britain is rethinking its testing strategy over concerns that the test is as much as 30% false positives and negatives.
This follows on from reports from Italy and Spain that the disaster they are experiencing may well be due to faulty tests received from China.
These test errors resulted in infected patients being unwittingly grouped with uninfected patients.
The first line tests had shown a pretty spotty accuracy in China and Spain (China sourced). It’s possible the U.K. first line tests are just as bad. The U.S. CDC test appears to be about 98% accurate given the number of confirmatory lab tests that have a negative result (1~2%) according to CDC published data. So U.S. positive cases are double-validated as positive.
I know of eight cases locally with only one that will be potentially officially counted – the test results are headed for confirmation by a CDC lab. I suspect we probably have millions of infections in the U.S., China had 10 million or more cases (and 50,000 or more dead), and Italy has a million infected… but we won’t see those numbers all counted. Roughly 30% or so of cases are asymptomatic and 60% or so have mild symptoms that might not even result in a doctor visit or tests… so we’re counting just 10% of the cases and basing mortality and prevalence on that. This is also what happens with the flu, but we’ve long figured out how to estimate from the positive cases just how many wild infections went undetected.
‘millions of infections in the U.S., China had 10 million or more cases (and 50,000 or more dead),”.
I agree, especially, from my research, with the ” or more”. I am very certain China did not destroy their economy over a few thousand cases.
I am certain many mild cases are missed. I am also confidant many deaths are never properly attributed to this as well, and not just in China. The penimonia pathology of Covid-19 is a 98 percent certain way to identify the virus, and nobody uses this.
Log analysis of Italy seems more encouraging:
Thank you so much for the very well written piece! I have neither the education or intellect of the author, but I have been making a very similar argument since this “lockdown” began. My wife and I live on the East side of King county where this virus was first recognized. We both have volunteered and been paid to work in the past at the ill fated Life Care Center in Kirkland, which was a very fine facility that offered a higher level of care than almost all other “nursing homes” in the area. So we take this very seriously.
This virus seems to have been circulating in our community for a considerable length of time before it was identified in a tragic way at the Life Care Center. The spread was likely more widespread than originally believed. I believe this is why deaths and serious illness have peaked here before they have in other parts of the state and country. The lockdown can only really be expected to slow the transmission of the virus hopefully until more effective treatment for the vulnerable groups, not end the threat.
Steven, you and your wife are very fine people.
So, are you saying there deaths that were attributed to pneumonia or other respiratory problems before the Life Care Center outbreak?
The Center had 3 to 7 deaths per month, on a regular basis with about 120 residents. Until deaths spiked above 7, there was no indication that any thing special was going on.
Thus regular activities, including the coming of medics, and the cross-working of staff at other similar facilities had done much damage before anyone suspected something. Another few days passed before officials started to exert control.
Washington State is just now, maybe, catching up.
Someone close to me used to work in long term care approx. 20+ years ago. It was known at that time that during flu season a significant number of residents would become infected and many would die. It was also the practice to schedule much of the staff with part time hours. This resulted in many staff working at multiple facilities and contributing a great deal to the spread of the illness. It is a structure that saves money so it is allowed, if not encouraged.
Steven Miller,
We live near Ellensburg, about 100 miles east of you.
There are only a few senior care facilities over here.
They closed after Thursday, March 5th. My wife and friends played music in one on that day. By the following Thursday all the places were off-limit to all.
None are reporting cases of this virus.
The misfortune of Life Care of Kirkland was, perhaps, a cue to get in front of this at other places.
circulating in our community for a considerable length of time before it was identified
≠≠==≠===+=
I suspect that it was in a popular casino in northern California the 3rd week of Feb. Lack of access to testing prevented confirmation.
Dr. Steele this is well worth thinking about, thank you. I was reading about the influenza cycling through recruits at the various military camps during WWI. They observed increasing virulence as new batches of recruits were brought into the camps. What turned out to be mild and relatively small numbers in the beginning became deadly and widespread when it began to spread in the subsequent populations.
Here’s an interesting discussion of the Spanish flu. Debate continues.
http://www.cidrap.umn.edu/news-perspective/2011/09/study-suggests-1918-flu-waves-were-caused-distinct-viruses
I think there are two primary reasons the Wuhan Coronavirus has caused so much panic. The first is that it is novel and no one has any real feel for how deadly it may be. The early figures out of Wuhan were alarming and the first SARS was certainly very deadly. The second is the early response of the Chinese Government. First they tried to cover it up, suppress reports, claim there was no person-to-person spread, and invoke their lackeys in the World’s news media and their pet politicians to claim there was no problem, no reason to quarantine, just the flu mate. Then the CCP freaked out, shut down everything and started spraying everything with bleach. These actions are worthy of some serious paranoia.
Then the modellers jumped in with their GIGO mortality estimates and the MSM switched from ‘racist’ to ‘we are all gonna die’. Every new death a headline, but no information on how old or already sick they may have been. What is a country’s leader to do?
Too late now to expected a reasoned approach. Lockdowns aren’t the end of the world* and far less destructive than a war. We may actually see less mortality this year than normal – traffic is way down, crime is down, anyone feeling sick is probably seeking help sooner rather than later, Wuhan-related deaths are probably harvesting mostly people that would have died from other complications or infections anyway. All those people who may have died if there had been no lockdown get a new chance on life. That’s not a bad thing. Those that Wuhan kills that would have survived are out of luck, but the lockdowns probably mean that this number is lower than it may have been.
An added benefit is that the World’s leaders now have no excuse for not developing a solid pandemic plan. As far as we can tell at the moment, Wuhan Coronavirus is not all that deadly and if the infrastructure for a pandemic had been in place, there would have been little or no disruption. The next pandemic could be far worse. Let’s hope the response isn’t like it has always been for Australian bush fires: a couple years of good intentions and then forget about it.
*Australia just started limiting alcohol purchases, so maybe it is the end of the world
Excellent article. I was a kid when polio raged and remember seeing pictures similar to the picture in the article. We had an adult neighbor in an iron lung.
My problem with the numbers being reported is that we don’t know how accurately numbers have been weighed. There seems to be a bias to claim all deaths were caused by covid. But are pneumonia deaths ascribed to covid because of the virus or an unhappy coincidence. We also have no idea what the real denominator is when reporting death rates.
There is no reporting standard. In Italy and Pennsylvania, the dead are being tested for coronavirus, and if positive, that is the cause of death regardless of other conditions. Other places are doing different things.
It’s almost like there is a conspiracy to minimize useful information.
When you were a kid, do you remember how “polio” was defined? What tests were made to know how had “polio” and who was “just” paralysed?
“perhaps a more targeted approach would be better”“. Yes.
I am puzzled by a seeming conflation between mild symptoms in some people, and hypothetical mild strains of the virus (there is some evidence of possibly two or more strains in Asia), and the apparent tenancy for the disease to hit older age groups harder and also largely spare the youngest age groups.
I do not think the mild cases of the disease experienced by some 80% of those infected has anything to do with viral strains.
Part of what is happening could be related to the size of the initial infective dose.
But it is clear people who are asymptomatic can and do pass the virus to others who may get a severe case and wind up with viral pneumonia.
But there has to be more to it than that.
Something else is going on with kids apparently, unless somehow nearly 100% of the youngest age groups are avoiding a large dose of virions entering their bodies.
No one understands this virus very well, and in fact many of the early mistakes that were made involved inferences about this virus behaving like other viruses that were closely related phylogenically.
It was assumed that asymptomatic transmission was unlikely, or only possible for a short period of time.
Most viral infections and especially respiratory ones are most contagious when a person is sickest.
It was not understood how many people were asymptomatic, or that these people were not just carriers but spreaders of the disease.
I think it is still not understood how it seems to spread so readily in some circumstances, but barely at all in other circumstances…even within the same person within a span of days.
There have been people who infected large numbers of other people but not their spouse that they lived with.
I cannot think of any other virus that gives either mild or no symptoms in 80% of people, but sends the other 20% to the hospital, or that makes some people so sick they spend weeks and weeks on a ventilator, while others get well quickly and go back home in a few days.
And the whole thing with three distinct stages of illness seems unusual as well.
But I think it it turning out to not be true that only old and frail people are getting severe cases of the disease and viral pneumonia. Rather, the old and frail are the ones least likely to be able to survive weeks of viral pneumonia. Young and strong people with supportive care can usually survive just about anything.
But a lot of younger age individuals are getting viral pneumonia, which is very unusual. They are just not dying of it very often, and when they do it is typically after several weeks.
The again, some young and relatively healthy people seem to have died in a few days.
It is not a typical illness at all, or so it seems to me.
I suspect that perhaps there is huge amount of viral shedding at some stage of the infection, and that perhaps also the number of virions that constitutes an infective dose varies greatly from person to person.
There is also a gastrointestinal component in some percentage of people who get exposed and infected, and some of these people get diarrhea. It is not unusual for a huge amount of virus to be present in the feces of such patients. This seems to be not getting much attention in the warnings given out. Zero in fact.
Someone needs to investigate this and probably a good idea to close public restrooms in the meantime.
Early on, there was word out of China that cases of the gasotrointestinal variety were milder.
Is it possible that infection by two strains could act synergistically?
Anecdote : reposted on Facebook a report of a Valladolid ( 100 clicks north of Madrid) couple still in quarantine as well as lockdown in their flat with eleven kids, ….wife got it first , then husband, grisly but not hos pital, then all/some of the smalls , in whom it gives digestive symptoms, explosive vomiting and diahorrea , over fairly quick and she used plenty of bleach in the bathrooms , account taking for granted that folk KNOw the kids version is like this AND possibly dont know that the digestive version has a high viraload in stools (_ and vomit ?).
link
https://www.religionenlibertad.com/espana/648072270/Chema-e-Irene-con-11-hijos-y-con-el-coronavirus-en-casa-La-fe-es-lo-que-mejor-nos-funciona.html
Later reports have also contradicted early reports, suggesting the gastrointestinal version may be more serious.
Yes, this is what the more recent and more detailed reports have said…people with the gastro symptoms have a better chance of having a more severe illness.
As a teenager in the early 1950s in Winnipeg my parents sent me and my younger brother to a log cabin built by my father as a summer cottage on a small lake in Ontario on the Canadian National rail mainline. Two neighbors asked if their boys could go with us and off we went by train.
After 3 or 4 days I woke up with a mild fever and stiff muscles, symptoms we had been warned about. We had planned a 3 mi walk to “Mile Post Ten along the tracks, an uninhabited lake with no name, known to have prize Jackfish https://duckduckgo.com/?q=northern+pike&t=samsung&ia=about&iax=about
I told no one and decided this was my last chance to fish in this lake, so I took along aspirins, lunch and fishing tackle and set off guiding brother and friends. There was a scary 200m or so railway tunnel driven through granite that we had to go through, which we did by running as fast as we could. By the time we came out the other end I was sweating profusely and my legs and back were quite painful.
Walking the rest of the way in the rising sunshine I was thoroughly soaked with sweat and and feeling miserable. We got to the lake and we caught a few fish, went swimming and, of course, had to walk back with another sprint through the tunnel in the final half mile.
I was tired but felt better and my legs didn’t hurt. I went to bed early and when I awoke I felt pretty good. Over the next several days the other boys came down with the same symptoms. I told them about my episode and recommended another athletic day for each and all recovered as I had. Was it polio? I’ll never know.
Dr Steele – A well written and thoughtful article. Thank You!
You end by saying the future actions – or not, must be debated. That will certainly happen but I HOPE the debate will be supported by facts and serious statistically sound studies – not the half guesses and rash conclusions so prevalent up to now.
RE: “Flu infections dramatically drop beginning around April. Relative to seasonal warming, a lockdown (on Wuhan virus) may have a minimal effect.”
South east Florida, with temps in the 70s/80s F, is experiencing rapidly increasing infection rates from the
Wuhan virus. New Orleans LA is experiencing similar temps and infection rates. These are summer temperatures typical for much of the USA. The early evidence indicates there is no seasonal effect ‘question’ for Wuhan virus, let alone one that needs to be debated. We will have a great deal more data from direct observation in the next several weeks also, to confirm or deny any ‘seasonality effect’ hypothesis. Florida Gov. Ron DeSantis today issued a ‘stay at home’ order for SE Florida. This may cause a confounding of variables, for analytical purposes.
I speculate the complete lack of immunity or resistance to this ‘new’ virus in 100% of the population is the primary factor. Another grand experiment… and we all get to be test participants this time!
According to data presented on the Atlantic’s website, as of today there have been 53,698 tests and about 10% were positive. However there have only been 63 deaths, which is 0.01% of all tested Floridians and 1.2% of the positive test results. That mortality rate seems very good considering Florida’s high population of elderly that were climate migrants fleeing to warmer weather.
Jim Steele,
RE: “Flu infections dramatically drop beginning around April.”
Your assertion was Wuhan virus infection rates would seasonally diminished like common flu infections. That is what I addressed. You responded with tentative morbidity rates? Are you now shifting to seasonally affected morbidity rates?
Here in the Great NorthWet of Washington State , data from the UW Virology Covid-19 Dashboard shows 37,626 test performed by UW Medicine labs, with 3,401 positive results, for a positive infection rate of 9%. (90% of this data is from the Puget Sound area, though 3/29/20.) This is actually a slightly lower infection rate than your Florida data exhibits, despite the warmer summer-like Florida temps. Our temperatures for the last month have been in the 30s/50s F, with one week in the 40s/60s F. And 3 of the last 4 weeks here have been cold rain, sleet, and more rain, typical for this time of year.
I’m not seeing an inverse correlation of Wuhan virus infection rates with respect to temperature, in the observational data discussed here. Do current temperatures show any correlation with Wuhan virus infection rates in Spain, Italy, France, and Great Britain as compared to New York, Florida, California, and Washington states? Inquiring minds need to know….
And The Grand Experiment continues…. with us all as involuntary test participants. Isn’t observation based science great?!! Learn, survive, adapt, and thrive Y’all!
Data from Chile show few cases and no deaths in the desert north, but disproportionate numbers in the cool, moist south:
https://www.minsal.cl/nuevo-coronavirus-2019-ncov/casos-confirmados-en-chile-covid-19/
Araucania Region (937 K pop) now has as many deaths, four, as Santiago MR (over 7 M).
My central coastal region (Valparaiso) just recorded its first death.
North: 81 cases; 0 deaths (2.2 million population)
Center: 1620 cases; 6 deaths (10.9 million population)
South: 1037; 6 deaths (4.5 million population)
Total 2738 cases; 12 deaths (17.6 million population*)
*As of 2017.
Maybe because the elderly down there aren’t idiots having made enough to retire in Florida and not being idiots they have been staying home.
The flu doesn’t send this many people to the hospital this quickly. I don’t recall reading stories about NY using refrigerator trucks to store bodies during flu season. So, saying this is comparable or may be comparable in severity to the flu defies all logic. “At most, we might have casually noted that flu this season seems to be a bit worse than average.” Printing this as if anyone still thinks this might be true is dangerous. But, then again maybe NY builds temp hospitals in Central Park every bad flu season. /sarcasm /
here you are conflating two different metrics . . . the speed of spread and the morbidity. I guess either of those could be thought to be a comparison of ‘severity’. But they aren’t the same thing.
I did no such thing. I am speaking to saying things and printing old quotes in a fashion that is clearly designed to give a specific false impression while at the same time being “true”. Cherry picking is another word for it. So, if spread and morbidity aren’t the measures of severity of a pandemic then pray tell what is?
Jim, it is far to early to look at a CFR now. It is about ten days on average from symptoms to severe, and plus 4 more days to fatal if death occurs.
It is more accurate to compare completed cases, either cured or dead.
Time will tell, but consider that New York State has a slightly smaller and younger population than Florida and has at this point about 10 times the number of cases and 20 times the number of deaths, though certainly Florida’s population is more widely dispersed.
They have subways, and everyone uses them…plus DeBlasio kept schools open long past when he should have closed them.
Schools are germ factories, and kids are germ fountains.
jMac, My full comment was “it will be difficult to determine how effective a societal lockdown was if COVID 19 behaves like influenza. Flu infections dramatically drop beginning around April. ”
Notice the word IF. I do not know how all strains of COVID 19 will behave but a study from MIT suggested there may be an optimal temperature range for transmission stating ” 90% of the 2019-nCoV cases have been recorded in the same countries within a temperature range of 3 to 17C.”
https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3556998
The world should stop its overreaction to the coronavirus, which can successfully be treated using Hydroxychloroquine, Zinc and Z-Pak.
Mervyn
Do you have a license to provide medical advice? If so, save your advice for paying patients. If not, just save your advice period.
Mervyn,
If by “successfully” you mean…if you swallow some pills, they will go down your throat, then i agree with you.
As for them having any effect, there is none of what is called “evidence” to support that notion.
More info is pending…Film at 11:00.
Since Quinine has been used to treat malaria for a hundred years, if its effect is so apparent, why wouldn’t anyone have noticed its effect on Coronavirus, a member of the common cold virus family, long before now ?
Yeah!
Why didn’t I think of that!
Are there any viruses in places with malaria?
cui bono
1. BIG STORM or “KILLER VIRUS” happens.
2. Some people are seriously harmed. Most are just fine or soon will be.
3. News media by exaggeration and selective reporting creates a HORROR STORY drama loosely based on fact with new twists every day so that people will read/watch all day long.
Reason: money
4. Alarmed public (especially those of the party opposite to the one in power) screams bloody murder for the government to DO SOMETHING. Calmer voices trying to communicate the facts are drowned out by the advertising-money-driven news media (or willfully ignored by politics-driven, anti-administration, “never let a good crisis go to waste,” opportunists)
5. Wanting to ensure re-election, the government does something: THROW A LOT OF MONEY AT IT.
And, so, there you go. $2 trillion.
(Money made necessary largely because of the unjust, unnecessary, and unwise (as Jim Steele and others have so ably shown) economic shut-down)
Two TRILLION.
cui bono
*********
Well done, as usual, Jim Steele! Thank you!
At least one thing is almost surely going on that has not been discussed, at least to my knowledge: The relative strength of an individual’s immune system varies hugely from person to person>
People with very string immune systems get more autoimmune diseases, but less cancers.
And the opposite is true…people with relatively restrained immune systems do not get autoimmune diseases, but are more susceptible to cancers.
It is an evolutionary tug of war.
Our immune system must be able to distinguish self from nonself molecules. But it is like walking a tightrope…too strongly attuned, and we tend to have our immune system attack cells and tissues of our own body, but too weak, and we will not suffer from these very often but we will be less quick to respond to genuine threats.
This cold easily explain, for example, why people with lupus were noted to not be likely to get a symptomatic cases of COVID-19…if indeed there was such a correlation.
This is a little know area within the science of immunology:
https://www.newscientist.com/article/2099313-autoimmune-diseases-may-be-side-effect-of-a-strong-immune-system/
I heard that many of lupus patients in China were taking hydroxychloroquinine and the connection was made that they had less severe COVID-19 cases. Maybe it was only because they had lupus.
It would be interesting if allergy sufferers were less susceptible to COVID-19.
My point exactly, Scissor.
I agree with you. The strength of the immune system makes a big difference . It is strong inn my family and I rarely get cold and the flue but when I do it does hit hard but I recover quickly. Yes I have minor autoimmune issues. However for my sister she has a really bad case of Psoriasis and related joint arthritis. And she is a family practice doctor and is on immune suppressants. Fortunately where she lives there are currently very few cases of COVID 19 . So I worry about her. But for myself I did have 4 days of extreme Fatigue ion late Febuary. No other symptoms. Was that COVID 19? Don’t know. And without a antibody test there is currently no way for me to find out.
Dang typos…I will be glad when we get an edit button back up in here.
String = strong
Cold = could
Nicholas
You remarked, “The relative strength of an individual’s immune system varies hugely from person to person>” Yes, and an individual’s immune system probably varies over time, depending on nutrition, vitamin D levels, mental state, whether the immune system is actively fighting some infection or toxin, and a host of other environmental influences. There is so much we don’t know in detail. Its not unlike climate.
It is immensely complex.
I think we have only a very rough understanding of the outlines of the processes that occur.
New cytokines are still being discovered, and the ways in which the huge variety of them interact is barely understood.
The same cytokine can have diametrically opposed effects at one time and in one place in the body, as that same molecule at some other time and place.
Even the mental picture most of us likely have can be more deceptive than informative.
We are all used to seeing little diagrams of a cell with a receptor or two and a virion going hither and yon, but in reality the surface of a single cell is complex almost beyond imagining.
Thousands of different receptors, a large variety of TYPES of receptors, and more we have not even discovered (it seems a good bet that when new ones are being elucidated all the time, we have not discovered them all)…
At present, a single T cell is thought to have some 20,000 receptors on it’s surface.
An awful lot of people seem to think there is some detailed understanding of exactly how a given virus, for example, gains entry into a cell, and that since the ACE2 receptor is known to be one of the ways, that it is the only way. But it is known that at least one and very likely two other receptor types are used by the virus to gain entry. Unknown is how many we may have no idea of. The methodology of elucidated this information is so arcane that it rarely is spoken of outside of the research community. It is not like looking at a video from a camera mounted on the side of a house to see how a burglar got into someone’s home, after all.
Looking at a micrograph of a small section of a cell which visualizes virions budding from the cell surface, gives some idea of how much more complex and everything-happening-all-at-once-ish the actual processes are:
https://fineartamerica.com/featured/human-coronavirus-ami-imagesscience-photo-library.html
Here is an article called Historical Review of Cytokines, from 2007. Advances since then are explosive, but it is not paywalled, so…
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3140102/
I think most of us can learn and enjoy the many videos on you tube which use animation to help with understanding some of the basic processes that occur. I suspect there may be some who have not seen even the first ones from Drew Barry, here set to start at the really fun to see stuff:
https://youtu.be/DfB8vQokr0Q?t=201
And along through somewhat more recent lectures from him:
https://youtu.be/s1qfim5awuE
And then the scads of purely educational ones, some very general, some very specific:
6 Major Functions of Cell Membrane Proteins
https://www.youtube.com/watch?v=mD3GmqjmqXQ
Paul E. Turner (Yale) 1: Introduction to Virus Ecology and Evolution
https://www.youtube.com/watch?v=WIEqm4TrHPA
ATP synthase in action
https://youtu.be/kXpzp4RDGJI
I could spend all my time watching this stuff.
All true, Clyde.
I wrote a longer comment in reply which will probably appear in an hour to a day or three.
Nicholas
It only took about 5 hours to show up. 🙂
I’m mystified about the timing. For awhile my comments seemed to be showing up immediately, all the time. Then, they started showing a delay again. Tonight has been a mixed bag with some showing immediately, while others have taken a few minutes.
Some countries which are currently locked down didn’t start that way. Britain, Italy, Iran and China their health systems are on the brink of collapse because they didn’t perform a lockdown, China only stopped trying to conceal the problem after the bodies piled up.
Britain went for herd immunity strategy, they had to change course. And badly affected US cities like NY probably wish they had done an early lockdown.
Mild strains normally emerge because lethal strains of a virus kill so rapidly and brutally they run out of fresh hosts. Covid-19 is not a fast killer, its a chronic disease in the sense that it takes up to 3 weeks of mild symptoms followed by in some cases a rapid deterioration and death, so there is far less selection pressure on Covid-19 to produce mild strains than there would be on a more rapid onset disease like lethal strains of Ebola.
But, Jim Steele makes a good case for the “lockdown” being of those who are likely to be deathly ill (i.e., those medical profile is the same as the patients in the overwhelmed hospitals: very old or young and or with serious underlying health issues).
instead of locking down the rest of us and crippling the economy.
Janice
There is also issues of freedom and self-determination. Those who are most at risk, the elderly with co-morbidities, would rationally want to protect themselves. Society should encourage and support such decisions. However, if they are not a risk to others, they should not be compelled to stay under quarantine. It is only those who are known to be infectious who should be compelled, under threat of punishment, to stay quarantined until they are no longer a threat to others. The world is handling the problem of isolation as though every country was a dictatorship. I read that some European countries were prosecuting people who were not in their homes, even if there was no one around them to catch anything from them. That is over-reaction.
I agree, wholeheartedly, Clyde. I wrote sloppily, above.
I have been saying all along that NO ONE should be under quasi-house arrest.
Self-isolation is the only isolation a free society should have.
My sloppy writing above left out a necessary condition: “Given” a heavy-handed, government, “stay home” order, it should not apply to all.
I envy not in any moods the captive void of noble rage… .
(just FYI, my license plate frame says, “FREEDOM ROCKS!”)
Hope all is well with you.
Take care.
Eric, The Imperial College model originally suggested Great Britain would have 500,000 deaths and would overwhelm hospitals which encouraged the “lockdown solution”. I dont have a link, but last I read, revamped models now expect no more than 20,000 deaths and a far less strain on GB’s medical system. More optimistically the latest data report for United Kingdom lists 22,141 positive cases and only 1,408 deaths which is a 6.3% mortality rate of those testing positive. I would argue the mortality rate for al of GB is much lower knowing there are many asymptomatic cases.
Thx Jim for this post.
It seems to me it’s crucial to always keep an eye on the actual numbers when yet another projection comes out with six figure death numbers – like the current 200,000 being trotted around for the US.
Reality is that as things stand – and discarding the Chinese data, the credibility of which craters ever more as we learn more about developments in all the other countries affected – we have less than 40,000 dead worldwide
The notion that the US on its own is on a trajectory to outdo that global total even as continues to grow, is not credible. For a first perspective, the US numbers should not be held up one or more individual countries, but at 330MM vs. 500MM population, against the EU as a whole – that comparison makes the 200,000 projection pretty unrealistic.
The ‘experts’ have it down to 5700 now which is a big difference to half a million.
A good article as always from Jim. So many mistakes have been made such as allowing free movement of people from China. Taking people with the virus to hospitals where there are sick people was always a bad idea so I can’t see why halls were not commandeered from the start as virus centres. The other article on WUWT from a doctor shows how badly prepared we were having blown billions on global warming there are no stocks of ventilators for something like this. As for trained staff, you only need a few trained staff to oversee a group that have enough knowledge to work the ventilators and monitor them. You don’t need fully trained doctors – look at how mass production is done and was done during the war years.
Makes sense.
Hi Jim, have they corrected for reporting lag? The following Lancet study calculates mortality rate by dividing the cumulative deaths to date by the number of reported cases 2 weeks ago.
https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)30195-X/fulltext
Upper limit 20% mortality rate based on Wuhan.
All good observations, Eric.
And I am not sure if you are referring to this, but there are persistent reports that as many as ten percent of recovered patients continue to test positive for viral RNA.
We know that some viruses can cause what are known as chronic infections…after a period of acute infection, some people are rid of a particular virus, but in other individuals the immune system is not able to eliminate the virus and becomes locked into a perpetual state of viremia. In other instances a virus does not circulate in teh blood, but it becomes dormant in one or more cell types within the body of that individual.
There are many examples of both types of chronic infection.
And often viruses that are closely related behave differently…with some in a family never causing chronic infection, and other very similar virus strains always doing so.
Of course Hepatitis C and HIV are ones that remain in the blood and cause an ongoing viremia. Chicken pox and other herpes viruses become lodged in other types of cells (nerve cells are a common cell type) and become latent, but can reemerge, often decades later.
So it will have to be resolved at some point what is going on with this virus.
Have we witnessed the evolution of a new virus which will become endemic in humans and, separately, will it in some people cause a chronic infection?
Nicholas
Herpes Simplex virus is a well-known example of a pathogen that can hide in the body and reappear periodically when triggered by factors such as hormones or emotional state. I’ve often wondered where the reservoirs for cold viruses are, which allow them to be resurgent when the climate is more conducive to their transmission.
By the time this is over, we’ll have lots of lovely data. When something truly dreadful comes around, we’ll have a better idea of what to do and perhaps we’ll be better prepared.
Rachel Maddow is dreadful.
https://mobile.twitter.com/bennyjohnson/status/1244709560021069825
This is the first time you’ve noticed?
Rachel Madcow has always been like that
I have just listened to the last half of the Dark Horse podcast. link The result is that I have had to concoct a sleeping potion.
Bret and Heather tell us that we have been lied to about the effectiveness of masks. You should wear some kind of face protection if you’re out shopping, etc. If you can’t get a mask, even a bandanna improves your chances of avoiding infection a lot. Safety glasses that prevent droplets from getting to your eyes are important. The podcast is well worth listening to.
I will add my own thing. In the food industry, dilute bleach is used as an effective disinfectant. 1 tsp. of household bleach per quart of water gives you a 200 ppm free chlorine solution that can be used on surfaces. This virus lives for a very long time on impermeable surfaces like stainless steel door handles. We’re making up for a shortage of alcohol based sanitizer by wearing cheap safety gloves (that we don’t care about) and sanitizing those with the aforementioned bleach solution.
commieBob
Another unconventional sanitizer is Bacardi 151 over-proof Rum, if you can find it. It has the advantage that if you don’t use it all by the time the pandemic is over, you can drink what is left.
AS IF Boeing Renton, Seattle, Everett needed to shut down.
********
Nice job, Jim Steele. As usual.
(I wrote a lot more, but, I used the “k” word
aaarggh! it will likely be tomorrow before I am out of moderashun (not sure if that’s one of the words) — when is this site going to be fixed?? wish an engineer were running it….. )
Thanks Janice, Good to hear from you. It has been too long a time.
That graph simply shows warm weather is healthier for humanity in general.
I agree. Our immune system does better during warmer weather. I blogged that on WUWT earlier
https://perhapsallnatural.blogspot.com/2020/03/warming-improves-our-health-part-1.html
Excellent essay. Social distancing may slow the spread and thereby lessen surges that strain hospital capacity, but the virus will infect a large percentage of the population eventually.
Those people who are infected with the virus but do not die acquire immunity. That immunity can be detected by serological assay — blood tests for antibodies.
Acquired immunity provides a better blockade for epidemic transference than isolation in the long run. A vaccine would also aid in prevention, but an effective and safe vaccine may be many months away.
In the meantime, the most at-risk people should isolate, but others should acquire immunity through mild infection and development of antibodies. Thankfully or hopefully, therapies like HCQ+Zn can save/cure those mildly infected.
Any volunteers?
Note: please see another excellent report ->
https://wattsupwiththat.com/2020/03/28/the-next-frontier-in-coronavirus-testing-identifying-the-full-scope-of-the-pandemic-not-just-individual-infections/
The development of the SAR-CoV-2 vaccine will have to take into very serious consideration the lessons learned from attempts to make a Respiratory Syncytial Virus (RSV) vaccine. RSV is a very common virus that leads to mild, cold-like symptoms in adults and older healthy children. It can be more serious in young babies, especially those in certain high-risk groups.
Right now corona virus makers and the FDA and CDC/NIH vaccines are looking at using messenger virus-like RNA transcripts to elicit both T cell and B cell immunity for SARS-COV-2. But the lessons of using a formalin-fixed RSV vaccine should be deeply cautionary of this approach when developing immunity to a deep lung respiratory virus, which is exactly what this SARS-CoV-2 virus is as well.
The formalin fixed RSV vaccine did induce a potent antibody response, so the vaccine developers thought they had the answer. What it did instead was actually make getting the live wild type RSV infection much more severe because the vaccine failed to develop the proper cytotoxic T-cell response in conjunction with simply making antibodies to virus. Our adaptive immune system works as two coordinated arms, the humoral-B cell- antibody arm and the T-cell cytotoxic /helper arm to clear most viral infections. And achieving long-lasting memory T cell cytotoxic response (one that kills infected cells that antibodies can not) generally requires a live infection. In the RSV vaccine case, that caused an immune dysfunction that amplified the real infection when it happened in children. Some children died directly as a result of getting the vaccine and then the real infection a year or so later.
In the case of the shingles/chicken pox vaccine the virus is live attenuated varicella zoster virus. In the case of the small pox vaccine, a live but much less potent vaccinia-pox virus is scratched into the skin surface to elicit an immune response to a live pox virus that provides almost life long immunity to small pox virus. Live viruses in both cases.
The each of the measles mumps and rubella vaccine components of the MMR trio-vaccine are also ALL inexpensive to make live attenuated virus components. That should tell you something when you hear these companies pitching their latest high tech vaccine analogs.
So the vaccine lessons of RSV and other viruses should geared towards the development of a Live Attenuated Corona Virus (LACV) vaccine to produce the potent immunity against SARS-CoV-2. I would be highly suspicious of any vaccine that doesn’t go that route.
The reality is a Live Attenuated Corona Virus vaccine may not be patent-able and be too easy to copy by others in other countries to avoid paying royalities.
So there is not the economic incentive to develop a LACV vaccine. But a LACV in my opinion is the only one that might actually work. Rather the economics of a pharmaceutical company making big buck s on a RNA or DNA vaccine are driving US vaccine development. That to me is the real scandal.
The annual influenza vaccine is a dead pieces and parts vaccine of 3 differnt influenza viruses grown in eggs that works only to boost antibodies to the latest HA-NA strain. It works ONLY becasuse we all have preexisting T cell immunity to live infection influenza, in which the T cells recognize and respond to highly conserved influenza peptide sequences that provides the cyto-toxic T cell response that the annual Influenza vaccine only marginally boosts along with the novel antibody response to the viral surface protein motifs which are highly glycosylated (sugar costed).
“The fact that many people have tested positive for COVID 19 virus but had no symptoms suggest there are various mild strains that could naturally impart immunity. ”
There are 8 strains. It mutates slowly. All strains appear equally deadly
‘Ioannidis argued, “If we assume that case fatality rate among individuals infected by SARS-CoV-2 is 0.3% in the general population — a mid-range guess from my Diamond Princess analysis — and that 1% of the U.S. population gets infected (about 3.3 million people), this would translate to about 10,000 deaths.”
His diamond princess analysis is DEEPLY FLAWED
A) his quoted CFR is wrong. patients continue to die
B) the CRF for 80+ passengers was 1/51. Which is a 6 sigma outlier.
‘Nonetheless, it will be difficult to determine how effective a societal lockdown was if COVID 19 behaves like influenza.”
Zero evidence that covid does, in fact it doesn’t. see Ecuador, Singapore, Thailand, Malaysia,
Question Jim, are you licensed to give medical advice to folks?
Mosher,
Please provide a link with the evidence that “There are 8 strains. It mutates slowly. All strains appear equally deadly”
““The fact that many people have tested positive for COVID 19 virus but had no symptoms suggest there are various mild strains that could naturally impart immunity. ”
please show how this is even logical.
You have zero business giving out medical advice.
I hope no one changes their behavior on account of your writing
8 strains.
go to the website following the genetics
https://nextstrain.org/
select strains by country.
or see the work by Charles Chiu
You have zero business giving out medical advice.
===≠========
100% nonsense. Actors give out medical advice on TV all the time. They wear a white coat and stethoscope, but they never say they are a doctor, so it is perfectly legal.
What you are not allowed to do is tell people you are a doctor when you are not.
Yeah…he should have his head examined!
Oops!
““The fact that many people have tested positive for COVID 19 virus but had no symptoms suggest there are various mild strains that could naturally impart immunity. ”
WRONG. you make a suggestion based on no genetic evidence.
This suggestion misleads people to their medical detriment.
It’s basically “advice” that suggests they may have less to be concerned about.
Your suggestion pollutes the discourse an informed public should be having.
It’s not a mere suggestion.
“The COVID-19 virus does not mutate very fast. It does so eight to 10 times more slowly than the influenza virus, said Anderson, making its evolution rate similar to other coronaviruses such as Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS).
It’s also not expected to spontaneously evolve into a form more deadly than it already is to humans. The SARS-CoV-2 is so good at transmitting itself between human hosts, said Andersen, it is under no evolutionary pressure to evolve.”
Look at next strain. trace the german strain ( german has a low death rate)
https://nextstrain.org/ncov?f_country=Germany
https://nypost.com/2020/03/29/at-least-8-strains-of-the-coronavirus-are-spreading-across-the-globe/
“These mutations are completely benign and useful as a puzzle piece to uncover how the virus is spreading,” Bedford told the outlet.
He said the various strains allow researchers to see whether community transmission is widespread throughout a region, which can inform whether lockdown measures have been effective.
“We’ll be able to tell how much less transmission we’re seeing and answer the question, ‘Can we take our foot off the gas?’” Bedford said.
https://www.news.com.au/lifestyle/health/health-problems/covid19-mutating-coronavirus-now-has-eight-strains/news-story/e70752f70f7e623c24aa02fbad16c705
““In the literal sense of ‘is it changing genetically?’ the answer is absolutely yes,” Harvard University infectious disease epidemiologist Marc Lipsitch told NPR.
“What is in question is whether there’s been any change that’s important to the course of disease or the transmissibility or other things that we as humans care about.”
The strains emerging are only slightly tweaked, with no variations in lethality, experts said.”
So which wins, your SUGGESTION or what genetics says and what evolution teaches us.
As you quoted, ““What is in question is whether there’s been any change that’s important to the course of disease or the transmissibility or other things that we as humans care about.”
Indeed many mutations are benign medically but useful for tracking transmission. Genetics tell us mutations are random and the one’s that survive and reproduce are maintained. There is typically natural selection against very virulent strains because the kill the patient before the patient sheds more virus.
If we look at the influenza virus CDC characterizes different strain into 4 types and many subtypes. Type A causes the pandemics, Type B was dominant early this season followed by dominance from type A. Type C is less common but is more effective against children. Type D seems not to affect people
There is much evidence to suggest different strains will have a range of effects. The real question how will one strain impart immunity against other strains and for how long?
The other question is why is Mosher ranting just for discussing these possiblities? Those rants or “polluting” civil discussion!
Is this you Steven?
https://www.washingtontimes.com/news/2020/mar/30/china-researchers-isolated-bat-coronaviruses-near-/
‘But Steven W. Mosher, a China specialist with the Population Research Institute, said China for years has been doing research, detailed in scientific journals, on horseshoe bat coronaviruses that could be harmful to humans.
“They write about collecting SARS-like coronaviruses from horseshoe bats and proving that, like the SARS virus itself, some of these other naturally occurring coronaviruses could infect human beings directly,” Mr. Mosher said. “They write about genetically engineering new and deadly viruses capable of infecting human lung tissue — just like the Wuhan flu does.”
Mr. Mosher called the Chinese government to disclose the research to help health officials cope with the coronavirus pandemic.
“China claims that the deadly virus did not escape from its biolab,” Mr. Mosher said. “Fine. Prove it by releasing the research records of the Wuhan lab.”’
That’s a different Steve Mosher
Looks like it is up to nine, according to this:
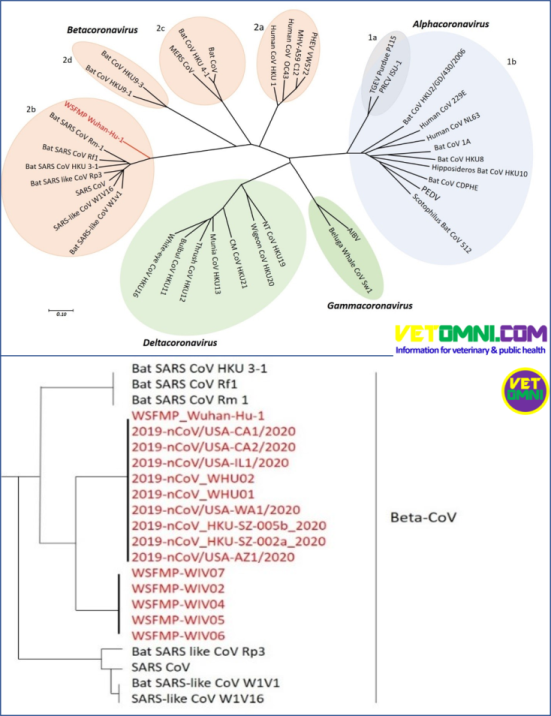 ?x84164
?x84164
https://vetomni.com/what-is-covid-19-how-can-we-win-against-it/
Not vouching for it, just sayin’.
44 according to this company and they appear to know what they are talking about.
https://frettatiminn.is/nordmenn-aetla-ad-rannsaka-covid-19-a-sama-hatt-og-islendingar/?fbclid=IwAR1Nd0CGhWWmr0g7bng4aKUg6-88DWotbirSQTo7tx1CNB5Fz2dfvby9zYU
https://www.decode.com/management/
The 44 individual mutations found in Iceland aren’t the same as strains.
Nine strains have been identified in Wuhan, Hong Kong, Washington, Arizona, California and Illinois, as per Nicholas’ link.
I knew there were several strains, what I was asking for is a link describing that they were known to all be equally deadly.
And it is totally logical to state, ““The fact that many people have tested positive for COVID 19 virus but had no symptoms suggest there are various mild strains that could naturally impart immunity. ”
Why is that not a good inference? Or are you just doing your typical Mosher sniping
I can answer that: Because there are numerous instances where a person with mild or no symptoms spread the virus to people who then developed severe illness.
This seems like fairly straightforward and convincing evidence that it is how people respond that is varying widely, not (necessarily) a mild strain infecting some people and a more virulent strain infecting others.
I am agnostic on the question of if there may be some variation in virulence between known strains of the virus, but I do not think it is changing in virulence from one person to the next in a chain of transmission.
If it was due to different strains, would we not be seeing some areas with everyone getting mild illness, and others with everyone getting severe illness, rather than what we see, which is that in each area, some people are asymptomatic, some are having mild symptoms or only feeling crappy for a day or two, and others are getting viral pneumonia and some of them dying?
This question is what I was asking you about in this comment:
https://wattsupwiththat.com/2020/03/30/unintended-consequences-polio-and-covid-19/#comment-2951498
NIcholas, The number of mild or asymptomatic cases can be explained by 1) differences in people health/immune system, 2) The strain with which someone is infected or 3) a combination of both, which I believe to be the case.
What about the extreme disparity in children being affected?
Children are generally more susceptible to diseases, having not had much time to acquire a suit of antibodies and memory cells from getting sick and then getting over it.
Children get tons of colds.
Babies are in a lot of danger from influenza.
But so far…the youngest age groups appear to be nearly immune to this one.
Besides for the two factors you mention, I have seen references to the amount of virus…the infective dose…at the time a person is first infected, as perhaps playing a larger role in disease severity than what we are used to seeing.
I do not know if anyone could have any clear answers to this at the present time.
As for less virulent strains…I am gonna pass on offering an opinion on that…I do not have any specific information to go on.
I am trying not to jump to conclusions.
This virus seems to have numerous peculiarities that are unexpected and not typical.
It does not seem to match up with what other viruses do when we get them.
What about the extreme disparity in children being affected?
Children are generally more susceptible to diseases, having not had much time to acquire a suit of antibodies and memory cells from getting sick and then getting over it.
Children get tons of colds.
Babies are in a lot of danger from influenza.
But so far…the youngest age groups appear to be nearly immune to this one.
Besides for the two factors you mention, I have seen references to the amount of virus…the infective dose…at the time a person is first infected, as perhaps playing a larger role in disease severity than what we are used to seeing.
I do not know if anyone could have any clear answers to this at the present time.
As for less virulent strains…I am gonna pass on offering an opinion on that…I do not have any specific information to go on.
I am trying not to jump to conclusions.
This virus seems to have numerous peculiarities that are unexpected and not typical.
It does not seem to match up with what other viruses do when we get them.
I am sure we will have more information as time goes by.
Jim, I value your opinion.
You are one of the writers here that I always seem to be in agreement with, so I know you must be very smart.
In your question to me at the top of the page, you seemed to be saying that we can choose to get a mild strain, or maybe you meant by avoiding it for as long as possible, the more deadly strains will become more prevalent and so that is not a good plan.
I seriously want to know more.
What should people do?
Should we find someone who has a mild strain and go hang out with them?
I do not think I have ever been worried about catching a bug going around before…but I am worried about this one, and I would like to not have to worry.
Just pointing out that there are at least nine strains, not eight.
That is not sniping, although he often deserves it if it was.
In the absence of any other information, what you ask would seem to be a perfectly logical possibility.
And there may well be variations in virulence emerging.
At least one report a while back seemed to be making a case for that to have occurred…a branching early on into more and less virulent strains.
I was going to get on Steven’s case for the tone of his response to you, especially that last part in which he was rather rude and snippy when he could have just been matter of fact, but it was late and why bother anyway…he does not give a crap about anything I say.
But separate from all of that…there are large numbers of cases of direct transmission in which the various individuals had widely varying response to becoming infected.
Jim, I am not criticizing you or your essay.
I want to exchange information, to share what I have read and hear what others think or may have inferred or read about.
If there are strains that confer immunity and only cause mild illness, that would be the best news I have heard about this whole thing to date.
I was mostly serious above when I said I would be very interested to know how I could get a mild case of the disease.
In my first comment up top, you responded (thank you for that…I do appreciate it and I forgot to say so) with a nod and then a question, and I tried to give a thoughtful reply.
LOL
Steve Mosher says “are you licensed to give medical advice to folks?’
No. But Mosher’s reply seems to be a bogus attempt to minimize any debate. I have never offered medical advice, only an overall analysis of the infection spread and its consequences.
So back at you Mosher, “are you licensed to give medical advice”?
I am pretty sure Steven is not licensed to regulate who is permitted, neither.
@jim Steele:
That SM, a known pro-AGW pusher of fabricated surface temperature data and notorious teller of half truths with no bona fide science credentials at all is attacking you is a good thing:
it is STRONG evidence that your position is correct.
******
“medical advice.” lol
Mosher; expert miner (Bitcoin). Climate scientist (Good with Excel). And now a medical expert? I’d value a second opinion, I’ll go and talk to some plants as HRH Ponce Chucky was famous for.
Patrick,
And vitamin D supercharged bon vivant.
You forgot vitamin D supercharged bon vivant!
Question Jim, are you licensed to give medical advice to folks?
Pot, kettle, you know the rest.
John
Yes, Mosher seems unable to recognize that he is behaving in the same way for which he is castigating Jim.
Now, the people who are actually giving “medical advice” are those who recommend HCQ+ without justification or citations, and do so in a tone that implies they know what they are talking about.
Jim wrote, “Perhaps by inhibiting the spread of a natural immunity, we may be setting the stage for another big wave of COVID 19 next year. These are questions must be debated.”
Indeed, the second wave of Spanish Flu in the Fall of 1918 presented with much greater pathology/sequelae than the first wave in the Spring of 1918.
So avoid infection now with SARS-CoV-2 with “shelter in place”, and you may be setting yourself up for a worse infection down the road when it’s evolved twin returns/if it returns. And in my estimation it will likely return in the Fall-Winter 2020 as herd immunity will still not be high enough to stop another epidemic. And any vaccine is still 18 months away from approval-availability.
Why we’re not permitted to catch this currently in the warmer months currently in Australia I have no idea.
It’s not going to be pleasant when winter hits and Covid-19 goes through the roof.
Wouldn’t it then be nice if we all caught it while the weather was warmer, spread was less, and hence “#flattenthecurve”.
Lockdowns currently in Australia does prickle my BS-senses.
It’s WAYYY OTT! 6 months jail and/or AU$11,000 fine if “out and about” with nothing essential to do???! Really?!
“and that 1% of the U.S. population gets infected (about 3.3 million people)”
This is a terrible assumption, IMHO. The correct model to use would be a flu model… and we have an average of 50 million cases per year in the U.S.. The current mortality rate, globally, is hovering around 4%. Nations with more thorough testing are closer to 1%.
That means 500,000 to 2,000,000 deaths per year in the U.S. without drastic measures. With the hospitals being overwhelmed without intervention we would edge to the high side of that range without a doubt… we are struggling already with just 165,000 cases – imagine what would happen if we had millions of cases at the same time?
Now, sure, we are in some ways only delaying the inevitable, but that means the hospitals will be able to better assist the people they have to assist and researchers will have more time to find effective treatments. Vulnerable populations will likely need to stay isolated until a vaccine is in widespread use or treatments or preventative medicines prove very effective. This means our overall mortality rate will drop even if the overall number of cases remains the same.
And, critically, let’s not forget that the more people who get infected the higher the probability of mutation. This is an RNA virus which can mutate very quickly… if we’re lucky we will find one mutant variety that causes minor to no illness and results in cross immunity. The SARS vaccine is being evaluated for possible cross-immunity – if we’re lucky that will prove true as that vaccine could be made available in just a few months.
Dear Loon,
According to the Worldometer there are 1,439,323,776 people in China. That’s 4.36 times the US population.
So using your model, China will experience 2.18 million to 8.72 million deaths per year “without drastic measures.”
Also according to the Worldometer, to date China has had 3,305 deaths from their virus. So they have a ways to go. It could be China is lying about their death rate. Or maybe Communist China really knows how to unleash “drastic measures.”
Or your model could be wrong.
China is lying about their death rate. Or
+====+!!!!!
All that is required to stop people from dying of C-19 is to stop testing for C-19.
If you don’t test, then they die of pneumonia. WHO labels you a success.
“China is lying”
Yeah, maybe. But we don’t have any clear evidence for it.
And don’t reference the images of urns; do you have any idea how many thousands they need every day in their provinces when everything is normal?
They need 220 urns per day on average, IIRC. Each location is seeing lines hundreds deep every day… We’re definitely talking about China having had tens of thousands dead and are covering it up.
You can use their crematory capacity and operational times to come to the same morbid conclusion.
Of course, I wouldn’t put it past the CCP to have simply killed everyone with symptoms. If the U.S. has, so far, nearly 200,000 cases despite the general cleanliness and comparative isolation of Americans, then China had WAY WAY more… and their lack of data sharing (first true data shared on January 30, IIRC) is why so many global cases occurred in the first place.
Please don’t tell me you even remotely trust China’s data.
We don’t even have flu data for China, so we would need a model of flu in China in order to see how this would spread naturally through their population. China also locked down their entire country almost overnight to stop the spread so using data from SARS-CoV-2 in China would be a useless comparison – even if the data was accurate.
>The current mortality rate, globally, is hovering around 4%. Nations with more thorough testing are >closer to 1%.
Pardon me for being pedantic, but I think this use of language is worth correcting.
We do not know the mortality/infection rate. Period.
4% is an ESTIMATE of the rate, based on known inadequate and faulty data.
1% is an ESTIMATE of the rate, based on known, but slightly less, inadequate and faulty data.
The only places I think have good data are South Korea and Singapore, but it’s not clear how useful their experience is to other places.
Iceland appears to have better data
“and that 1% of the U.S. population gets infected (about 3.3 million people)”.
This also seemed to me to be the weakest assumption (apparently it is Ionnin Ioannidis hypothesized scenario. The overall post is mixing various more optimistic scenarios and thoughts on policies of lighter lockdown. That is certainly important thinking but I think the idea of positing a low morbidity rate based on the idea of many asymptomatic or mild infections that aren’t tested at this point runs counter to the idea of a low infection rate!
The whole point is that there could be a very high infection rate but a very low morbidity rate and this squares with refrigerator truck morgues but the idea that the disease is not inherently more deadly than flu.
In any event, to validate these hypotheses you need random testing and we don’t even have testing for all folks who are mildly symptomatic nevermined randomized population testing.
Heads should have rolled over the testing screw up and Trump should have been straightforward about that screw up. It wasn’t his screwup, but he owns the coverup.
I respect his optimism and other contrarian voices on policy emerging but that should not insulate any from criticism.
There was no coverup of the CDC testing issue. I knew about it the day it happened – the CDC had already sent out new reagents by the time it hit the news. What wasn’t publicized is that it took a couple weeks for the labs to validate the tests afterwards and this testing is just the confirmatory testing and not the front line tests.
The delay only caused a delay in the official numbers, it changed no health prognosis or treatment. Doctors use symptoms to diagnose first and foremost – negative flu test and fly symptoms? Assume it’s COVID19, treat accordingly.
The delay diverted early track and trace approaches. We can’t rerun the counterfactual to see if the early IDs would have been effective. But it wasn’t just the delay, it was the bureaucratic field clearing that the CDC effected until finally having to get out of the way. The coverup is this idea that the federal government is doing a good job.
Show me the press conference where trump said the CDC is incompetent, i want academic and private labs bringing tests forward. Instead what he said on March 6th “if you want a test you can get a test” which is utter stupidity and politics. This could be Trump’s version of “If you want to keep your doctor you can keep your doctor”.
I like trump, i like his optimism, I like that he understand precaution can be overdone. But of course he should be called out when he is wrong. You can’t get a test 3 weeks later on that an if you ‘want’ one basis, nevermind testing resources for randomized sampling that would be the only valid way to check the varioius premises about this disease. To me testing is a complete and utter failure so far and he should acknowledge that and maybe focus resources on random sampling rather than checkups for every hypochondriac in the country. So when I saw coverup, I don’t mean that we didn’t learn realtively quickly of the failure of the CDC effort. But he didn’t dismiss the head of the CDC. He doesn’t appear to have taken control of and directed a positive outcome for testing. And his comments instead are along the lines of we’re doing fine on testing. That is a classic coverup. I’m no fan of politifact but I can’t see where they have got this one wrong.d
“https://www.politifact.com/factchecks/2020/mar/11/donald-trump/donald-trumps-wrong-claim-anybody-can-get-tested-c/
The CDC has a page for that:
https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/testing-in-us.html
You can see the timeline of testing – CDC labs were performing testing since January 17, the delay came well afterward, in February, when bringing on “public health labs” for the potential increase in workload. That delay happened in early February, so CDC labs were handling the entire workload. Still, certain labs developed their own tests and reported findings to the CDC which the CDC verified.
January 17 transcripts from CDC COVID19 teleconference:
https://www.cdc.gov/media/releases/2020/t0117-coronavirus-screening.html
Note: China stated they only had 45 cases on that date… understanding the timeline is critical to understanding why people reacted they way they did and why resources weren’t allocated as aggressively early on. You can blame China for that – it took Hubei whistle blowers to let us know just how bad it was.
On January 30 the very first epidemiological study came out of China that examined, IIRC, the first 99 cases. This was the very first hint we had of human to human transmission and a potential for a significant contagion risk… but it was also only 99 cases. Trump issued the China travel ban and declared a public health emergency the next day. He was lambasted by Democrats, including Joe Biden, and called racist and xenophobic. Many even thought he was overreacting for declaring a public health emergency. Only now do we know he wasn’t.
At this point in time the nations outside of China had only very few cases… travelers who picked up the virus would need a week or two to show symptoms and most would just assume they had a somewhat bad case of the flu unless they got seriously ill. With 80% or more of cases being rather mild you needed to wait until you started having serious cases before we could get real data from uncensored nations… and 30% or so of cases being completely asymptomatic further complicated matters.
The virus has a long incubation period and getting information to hospitals and doctors about how to get testing performed isn’t always the easiest… and you need to have those protocols established. The CDC continually issued guidance on symptom based diagnosis, which is always the first means, and had a test available for other labs on February 3. That’s a very short turn around for something so complex.
Throughout February, however, the U.S. had hints that we had contained the virus within our borders… the numbers of daily new cases were declining. http://files.looncraz.net/sars2_cdc_feb_daily_new_cases.png
It wasn’t until March 11 that the WHO declared a pandemic – and Trump declared a national emergency. Using whatever data was available at the time is the only way to make policy decisions.
I take your point that some tracking from presumptive cases might have been appropriate and that the CDC was always testing from the 4th week in January, but of the first 500 tests sent to the CDC only 12 were positive. So I don’t imagine that we would anticipate the same level of effort per case to be expended on 500 cases that got tested that could be expended on 12 positives. There is just no question that the lack of a public health test was a significant set back, not only in the number of tests performed but the transit time to Atlanta for samples and now that the notion of widespread asymptomic infection is a theory, it has crippled the capacity for randomized testing that would validate the extent to which this is so.
And your response studiously avoids what you think of the president’s statement on March 6th: “if you want a test you can get a test”. That is not a wise thing to say in the midst of a testing fiasco if its not true.
I’m not big fan of the New Yorker but with some limited snide comments about the President which they are simply unable to avoid, I don’t think the rest of this article is fake news. Yes coverup might have been an exaggeration, what i mean is lack of leadership and transparency. When you have to read the New Yorker to find out how other tests got approved, the fact that CDC posted their test results is not transparency. The president should have been the source of the timeline in the New Yorker article and explained who got fired and who was elevated to clear the way for more widespread testing.
https://www.newyorker.com/news/news-desk/what-went-wrong-with-coronavirus-testing-in-the-us
It was January 21st when the CDC perfected its in house test. it was 15 days after that on Feb. 5th that it shipped the reagents some of which could not be confirmed leading them to pull certification for the entire shipment. But by Feb 21st, a full month after they developed their test they still had no replacement reagent to disperse to public health labs for broader testing with quicker results. That’s 2 more weeks and a full month since they developed their test without widespread testing. The failed shipment was to have provided 50,000 tests that were to have been available from early February. Finally the President
On Feb. 24 the Association of Public Health Laboratories filed a for a regulatory waiver to create their own test. On Feb. 26th the FDA suggested the APHL use an obscure waiver request (EUA) to get its test approved. It also finally allowed the public labs that had been able to confirm the first set of reagants sent to use those to construct tests. That’s 3 weeks wasted. On Feb. 28th the State of New York, whose public health lab had not been able to confirm any of the reagents sent filed for an EUA for a test created in state at the Wadsworth Center. And finally on Feb. 29th the FDA said essentially any health lab certified in high complexity testing could run its own COVID tests (which means that these various tests that were being given EUA waivers did not have to be certified for use in each separate setting).
There are various indications, including the University of Washington conducting about 300 tests that could not be communicated to the clinical setting that the disease was not rampantly spreading beyond clusters in Washington during some of this delay. And some cases were being confirmed by the CDC. The evidence is less clear as to whether the lack of more widespread testing may have lead to failure to early apprehend the more widespread community transmission in New York.
It is simply an unknown counterfactual whether earlier public health response might have reduced the ultimate severity of effect or perhaps better timed it across the country so as not to shut everywhere at once. South Korea is a a telling example, although like talking about how great trains are in europe, it is simply a different culture so testing, while important, is also buttressed by more cooperation of citizens in isolating themselves when recommended such that the entire economy has not been shut down in Korea yet they have vastly limited the spread.
So the President adverts to the attention on Korea by saying on March 24th that we tested more people in 8 days than South Korea did in 8 weeks. Much fodder is made of this but the numbers are pretty close, but not quite what he says. 351,000 for South Korea in 8 weeks to 339,000 fothe US in 8 days. This demonstrates the advent of private testing finally by that latter half of march. But that still has not satisfied the earlier proclamation: “if you want a test you can get a test”.
Most importantly, even with the approval mid-march of March of various private lab tests that vastly ramp our capacity, this doesn’t address the utility if those results were available earlier and we still haven’t focused our capacity on randomized testing which is the only way to confirm the hypothesis that many optimists are developing that the disease is more widespread than understood and thus less less virulent in effect.
In a regime where limited tests have been reserved to symptomatic cases and high risk cohorts such as health care providers and where the president’s benchmark statement of early March that anyone who wants a test can get a test is still not true, and where that metric, in any event, is not the widespread randomized testing needed, noone can look at the management of the testing regime and say it was well handled and it wasn’t a failure of the administration on day 1 but it is a failure of the administration by day 70.
Failure of reagents is not an unknown problem and certainly not the President’s fault. But if he was going to walk softly and carry a big stick, he should have took checked that his stick wasn’t rotten. This is the guy who is laying waste to the regulatory quagmire, this would have been the place to start. Some might say that it is herculean that the FDA went as far as it did in the weeks following the reagent failure to consider waivers for tests from other than the CDC. But it did not invite those. Indeed were it not for the uninvited intiative of the APHL and the under the radar activities of the University of Washington we would have had no expansion of testing until private tests hit in mid March.
The FDA should not have taken 3 weeks to give authorization for the use of the portions of the initial shipment that were confirmed to be used. A bad test would not be helpful, but a decent test vs. next to no testing capacity is a reasonable tradeoff (just what bureaucracies can’t figure out). This was delayed by almost a month. If one had simply used the reagents that could be confirmed from the initial batch as a screen and sending positive samples (or particularly suspicious negative samples) to the CDC for final determination, this could have focused prevention and quarantine efforts when the numbers were still relatively small. And the lack of the administration engaging labs with alternative tests at best is poor engagement and at worst is poitics because those tests were developed in states that are not supportive of the president. I don’t think that had as much to do with slow walking new tests but you can’t even risk that appearance.
This history is simply unacceptable. It is not the President’s fault that things started in the wrong direction but it’s his responsbility that they didn’t correct course more quickly. If indeed there was a lack of responsiveness to his demand that testing be available to anyone who wants it, he needs to show how he cut through the bureaucratic clutter to make it happen.
But Trump insisted on March 6th, “if you want a test you can get one”. Your reminder of aspects that were working does not address this. He should not have said that if he could not deliver. Further, it is clear now that may have been a populist goal but it was not the right goal for reopening the economy which is of greater populist import in the long run. We should instead focus a serious portion of capacity on randomized testing as that is where the information to allow opening the economy will come from. But the administration has not said this.
Of course anyone who exhibits symptoms or who has had likely exposure or is at high risk of exposure should get a a test for clinical purposes and, apparently, can at this point. But skepticism of the President’s handling of testing (which is to say as the boss of the agencies that are supposed to handle it) increased during March due to anecdotal cases of patients whose presentation was thought to be marginal were refused tests and who turned out to be COVID some of whom actually died. It doesn’t mean they didn’t get appropriate care, although the question of monitoring contacts is up in the air and these are the perfect vessel for skepticism of the President–that folks who have the disease couldn’t get a test after he implied that virtually anybody could get the test.
He should put to rest the controversy about “if you want a test you can get a test”. As I said, that will otherwise be seen in the same light as “if you want to keep your doctor you can keep your doctor”. I respect some of his instincts and leadership here. I’m not a detractor of the President in any general sense, but he is doing himself and his relection no favors right now.
and I feel like I’m in good company. I find that Tom Cotton is more or less saying the same thing as I am:
“The CDC should not have acted like know-it-all bureaucrats who had the only medical and scientific expertise to develop tests. We have lots and lots of very capable labs all around the country,” Cotton says. “The FDA should not put all of its eggs in the CDC basket. . . . They were slow to use their emergency-use authorization.” In a January 26 appearance on Face the Nation, Cotton called on the FDA to expedite approval for testing to state and local governments.
“The bureaucracy just didn’t move as fast as it could have,” he says. “Dr. Fauci said it’s not the president’s fault. It would have happened to any other president. But it was a lost opportunity, given the time the president bought everyone with the travel [restriction].”
Does the president ultimately bear responsibility for the failures at the CDC and FDA? “He is the president, and it’s always the president’s job to push the bureaucracy when they’re moving too slowly,” Cotton says. “But sometimes you have to push very, very hard.”
and i feel somewhat vindicated that i find I am on the same page as Tom Cotton:
https://www.nationalreview.com/2020/03/the-senator-who-saw-the-coronavirus-coming/
“The CDC should not have acted like know-it-all bureaucrats who had the only medical and scientific expertise to develop tests. We have lots and lots of very capable labs all around the country,” Cotton says. “The FDA should not put all of its eggs in the CDC basket. . . . They were slow to use their emergency-use authorization.” In a January 26 appearance on Face the Nation, Cotton called on the FDA to expedite approval for testing to state and local governments.
“The bureaucracy just didn’t move as fast as it could have,” he says. “Dr. Fauci said it’s not the president’s fault. It would have happened to any other president. But it was a lost opportunity, given the time the president bought everyone with the travel [restriction].”
Does the president ultimately bear responsibility for the failures at the CDC and FDA? “He is the president, and it’s always the president’s job to push the bureaucracy when they’re moving too slowly,” Cotton says. “But sometimes you have to push very, very hard.”
and i feel somewhat vindicated that i find I am on the same page as Tom Cotton:
https://www.nationalreview.com/2020/03/the-senator-who-saw-the-coronavirus-coming/
“The CDC should not have acted like know-it-all bureaucrats who had the only medical and scientific expertise to develop tests. We have lots and lots of very capable labs all around the country,” Cotton says. “The FDA should not put all of its eggs in the CDC basket. . . . They were slow to use their emergency-use authorization.” In a January 26 appearance on Face the Nation, Cotton called on the FDA to expedite approval for testing to state and local governments.
“The bureaucracy just didn’t move as fast as it could have,” he says. “Dr. Fauci said it’s not the president’s fault. It would have happened to any other president. But it was a lost opportunity, given the time the president bought everyone with the travel [restriction].”
Does the president ultimately bear responsibility for the failures at the CDC and FDA? “He is the president, and it’s always the president’s job to push the bureaucracy when they’re moving too slowly,” Cotton says. “But sometimes you have to push very, very hard.”
And in most places, even with increased capacity you cannot get a test if you want a test. you can only get it with a prescription:
https://wwjnewsradio.radio.com/articles/news/detroiters-denied-coronavirus-testing-without-prescriptions
same is true in Rhode Island where i live.
…there seem to be strong correlation between severity of Covid-19 outbreaks in Europe and the adoption and duration of the Calmette vaccination (tuberculosis) program.
Germany and Austria kept on for a long time – and have the fewest problems now. Italy and Nederlands apparently never had the program. Neither did the US.
Most european contries stopped in the 80ths meaning people over 40 have protection. Spain is the odd one out here – bur was the program really effective under the Franco regime?
Another strange thing has been that the Covid outbreaks never really started in Africa and India as otherwise expected – but most of those contries still have a Calmette program going.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3062527/
The US doesn’t have the BCG vaccine for a very good reason. Because BCG (1) frequently doesn’t provide protective immunity, and (2) produces a life long positive skin test for the tuberculin antigen used in the TBT test. This BCG vaccinated populations then makes monitoring for spread and containing TB outbreaks very much more difficult as the simple screening method TBT fails, and only more problematic xrays and biopsies can diagnose TB infections. It is very slow growing but nasty bacterial critter for still the most cases in the West respond to frontline antibiotics, although MDR and very deadly XDR TB strains are slowly spreading out of Africa.
…however I can see that doctors in Denmark have had the suspicion that the rise of asthma and allergy diagnosis among children might be explained by the cancellation of the Calmette program. Hence have started a research project – but probably not with results yet.
So the thought that the vaccine could strengthen the immune system against a variety of diseases not related to TB has been there before Covid.
Also TB is fairly rare in the US and Canada, IIRC.
The organism is around, but few get chronically infected with it here.
Those who get it here in the brought it back with them as they’ve almost always spent substantial time in some place like South Africa or South Asia.
Mods,
My comment #2951607 stuck in moderation because I used the “K” word in regards to vaccine and viruses.
Thanks.
Joel
I played outside every day as a child, worked outside every day, accidentally gulped (alcohol was involved) the fetid waters of the Fox river in Illinois.
I’m pretty sure I’ll survive Her latest attempt at my life.
From what I have read of the 1918 epidemic this flu killed a disproportionate number of younger people. Whether this was because of large groupings of the young as the demob after WW1 was happening is speculative. Another oddity was some deaths occurred very rapidly after the onset of symptoms, on occassion within 24 hours and manifested with an Ebola like bleed out. There has been speculation this was caused by overdosing on aspirin which had just been synthesised and there was little knowledge of appropriate doses.
have a look
http://www.healthdata.org/covid/updates
Thanks. How do we see the past predictions? Will those remain published as well?
“Nationwide, a total of 83,967 COVID-19 deaths (range of 36,614 to 152,582)”
The tell of poor modeling and statistical reasoning is precision like this. It’s absurd.
There are similarities which makes a review of polio worthwhile. Both are viruses, too small to see, both have incubation periods, and people without symptoms can spread the disease. And for both, there is a lot that we do not know. There are differences too. Polio was endemic for centuries before it became an epidemic. The consensus is that it had something to do with improved sanitation.
(quote from the WUWT post of Dr. Krause, 1992)
“Before the introduction of modern sanitation, polio infection was acquired during infancy, at which time it seldom caused paralysis but provided lifelong immunity against subsequent polio infection and paralysis in later life.”
This is expanded upon in more recent detailed article (Sophie Ochmann and Max Roser (2020) – “Polio”)
https://ourworldindata.org/polio
The only strong argument I can find to avoid infection is the prospect of improved treatment down the road. Otherwise we are doomed to remain in lockdown.
There is no good reason to lockdown families with everyone under the age of 40, once we are past the peak and hospitals have spare capacity. These families should form the basis of our herd immunity.
These young people could restart the economy and with money in their hands bars and restaurants would soon be back as people celebrate.
Once we have herd immunity, everyone else can come out of isolation. Perhaps by age group, 50, 60, 70+ to match hospital capacity.
It is the under 40 group that does a lot of the spending in the economy. And this would provide a lot of opportunity for on the job training.
They under 40 are our future and this is being taken away from them, the longer the lockdown continues. At some point they will wake up to this fact.
They have my permission.
We had lessons posted in the mail. It took about 1 hour to complete the day’s work after which we rushed outside to play with all the kids in the neighbourhood! We didn’t get polio.
I’m actually surprised that the government can legally quarantine healthy people. This would appear to be a violation of due process among other things. I’d be surprised if this survived a court challenge.
Quarantine laws were written to lock away sick people to protect the healthy. They were never intended to be used to lock away healthy people.
that’s why there is no lockdown in Germany but only a “group-gathering” prohibition. I saw about 100 people (in groups of one or two) walking in the park in one hour. Exactly 1 (one) had a mask on.
ferdberple
I agree with you that, strictly speaking, enforcing a quarantine is illegal for those who are not infectious. However, I think that most people can see the wisdom of minimizing their exposure and are going along with it for the time being. That is to say, there isn’t a strong incentive to challenge the legality when people think it is in their best interest to comply, and the government is attempting to compensate those who are unemployed. However, I don’t think that they can keep the lid on the pot for more than a couple of months before Americans start acting like Frenchmen.
Has anyone mentioned the test for antibodies which is mentioned in the newsmedia. I should like to have such a test as I think I had symptoms of this viral infection just about the time of Chinese New Year when tourists came in large numbers to New Zealand and were in shops and supermarkets . According to MedCram Dr Seheult a lot of infected but not sick people without symptoms.left China innocently before the borders of Wuhan were closed. The same may have been true of pilgrims and technicians setting up electronic equipment and services.especially in Northern Italy.
“Perhaps designating one hospital to specialize on COVID and another for non-COVID medical care is a good strategy.”
Good suggestion but this only addresses part of the needed response. I have the highest regard for the good work done in hospices caring for and helping to relieve the pain of those who are dying. Quickly setting up modified hospices for those dying of coronavirus could really help with large numbers for which hospitals are not designed. They would allow people to die sooner without briefly prolonging their suffering by costly interventions.
Full agreement.
Let the virus spread.
It wipes elderly and sick out of the population.
It would certainly compensate for the imbalance forced by one-child over there, selective-child here, and other wicked… dysfunctional choices. Still, despite our established [secular] religion, neither planned parenthood nor parent are favored by other than a minority of the People and our Posterity.
thanks ! I,ll take that personally,shall I. And you are a complete stranger too. Tut!
What is the official explanation for the strong decrease of polio (whatever that is) after WWI?
It seems to me you are not familiar with the situation. Polio was a still a scourge after WWI — vanished some years only to reappear as a plague in others, such as 1951. If it had not been a serious issue than how would you explain the private funding of multiple research groups working on different sorts of vaccines? If my mother was any indication, the approach of summer was a time of dread pre-Salk.
I’m familiar with the official data on the so called “polio”. I sank after WWI. Why?
The usual nonsense from the antivaxer troll, as Kevin points out polio was still a scourge after WWI, there was a major outbreak in 1916 and then multiple outbreaks in the summers following growing steadily until the worst case in 1955. FDR caught it in 1920, my father in 1919.
https://tinyurl.com/qwfeest
What the hell is “antivaxer”, NPC?
Do you admit that you can’t answer my simple question, NPC?
Why do you make up lies about FDR having polio, NPC?
You so funny!
niceguy March 31, 2020 at 9:08 pm
Do you admit that you can’t answer my simple question, NPC?
I answered it, it’s based on the false premise that there was a “strong decrease of polio (whatever that is) after WWI?”
As the data I posted showed there was no such decrease.
Why do you make up lies about FDR having polio, NPC?
What lie,in August 1921 he was permanently paralyzed from the waist down following a fever.
The pro vax propaganda graphics posted everywhere show a spike after WWI then a decrease.
Do you oppose pro vaxxism, NPC?
Do you deny the explosion of polio in India, NPC?
Do you deny the many recent cases in the US?
niceguy April 2, 2020 at 4:16 pm
The pro vax propaganda graphics posted everywhere show a spike after WWI then a decrease.
No the data shows a spike during WWI (1916) followed by a gradual growth through the 20s and 30s until the largest outbreak in 1955, not a decrease.
Do you oppose pro vaxxism, NPC?
Do you deny the explosion of polio in India, NPC?
Yes, there haven’t been any cases there in the last 5 years, not an explosion in my book! Used to be over 500 cases per day.
Do you deny the many recent cases in the US?
Define recent, last case in 1979.
OK NPC, show your graphics; all graphics published by vaxxer show a decline after the post war spike.
Regarding India, there was an explosion of paralysis cases, it was widely reported, denier.
“Define recent, last case in 1979.”
Tens of cases last year as reported by all medias.
Stop the denial, denier.
1) Nicholas, unless you developed a cure for “polio” (whatever that is), you don’t have the right to comment here. YOUR RULES.
2) Please provide the documentary evidence someone had polio.
Jim Steele’s point is welcome. Perhaps we are traveling a path that leads to terrible unintended consequences. It is worth debating anyway.
A couple of other observations:
A health care system does not work if it is overburdened, yet the health care system is not likely to work well if the economy falters. Man does not live by hospital beds and masks alone, after all. Right now I don’t see much debate in some circle, but rather just a cry to save lives whatever the cost.
This current pandemic shares so many things with flu epidemics of the 20th century; for example, the interaction between the flu and pneumonia producing bacteria seems to be a common feature, and one related to the highest of mortalities. What is the actual cause of death?
We have short memories — not many people recall the 1968 pandemic, though it was quite deadly in the U.S. and around the world. What seems new is the sense of entitlement that the world can be made safe for all with just the right mix of spending and government policy.
If one reads about these earlier pandemics what one soon realizes is that these spread around the world, albeit a bit more slowly, even before the age of globalization.
Numbers from China are likely worthless for all purposes other than CCP propaganda.
K says “the health care system is not likely to work well if the economy falters. ”
Indeed. After SARS in 2005 the California had started to stockpile ventilators and masks and had 4 portable hospitals, but economic woes encouraged the government to stop maintaining that stockpile when the economy faltered.
“to stop maintaining that stockpile when the economy faltered.”
Which reminds us to never put the country economy in the hands of the medical establishment.
My almost lethal case of Asian Flu apparently immunized me and many others against the Hong Kong Flu, which was less deadly than the Asian Flu pandemic worldwide, perhaps in part from the immunity imparted by the 1957 pandemic.
The H2N2 Asian Flu virus mutated by antigenic shift into H3N2 for the Hong Kong Flu, but seems to have retained had enough surface similarity for the antibodies to work.
95% of the US cases are asymptomatic, don’t require hospitalization or result in death.
That natural immunity is already there.
This lying, fact free, fake news MSM’s fake pandemic is as fake as fake dying polar bears, fake rising sea levels, fake melting ice caps, fake man caused climate change.
President Trump should bring the full weight of the Federal Government to bear, sue the fake news MSM for crying “Wolf,” for yelling “Fire!” in our crowded theater, make them pick up that 2.2 trillion dollar tab.
Or it may be that being exposed to a small amount of the virus at once allows the body to react properly, and usually have no serious issue.
But doctors, who were healthy and not specially old, but who have been exposed to many highly contagious hospitalized persons don’t had time to fight the virus, as in China (although air pollution was probably also an important factor), were often ill.
About 8000 people die on a normal day in the US per CDC numbers.
If this was a real crisis, authorities would be showing us excess deaths above the normal amount of deaths. They aren’t.
If this was a real crisis, would be able to distinguish between a flu death and a death from covid-19 –they can’t.
I encourage anyone reading this to do some research on how medical examiners determine cause of death and what things they never put on a death report. Perhaps we the people will understand the medical system is, in fact, a human farming system and very little else.
My impression was that our medical system was more like a whole lot of people who train and study for many years, and then are waiting and ready with all manner of potions and machinery, to save the lives of complete strangers, no questions asked, if and whenever those strangers drop in after being injured or become ill.
At least, that is how it has seemed to me personally several different time, such as when I was crushed like a grape in a car wreck, and had my life saved when I was moments from dying or internal injuries and severe internal bleeding from my smushed liver, fractured spleen, ruptured diaphragm, hemothorax, 13 broken ribs (and a elbow turned to sand and a leg splintered into shards), duodenal hematoma, and all the rest of it.
I do not recall seeing any crops being tended, just a lot of people who did not know me who somehow knew exactly how to cut me open and fix me up enough to allow me to struggle back to the land of the living.
Nicholas
Are you sure you are the same person you were before the accident and you aren’t just a collection of spare parts? 🙂
I have a secret reality check from something that happened when I was about 1 or 2 years old: Back then there was a device called a fountain pen, which had a very sharp stylus, and a method of ink delivery far different from what is seen in a ball point pen.
Anywho…I recall vivividly, one day, picking up one of those pens and writing on my wrist with it…it immediately cut through the skin and left a line of ink. A self tattoo, old school style.
Still got it…so…still me, same reality plane as Center City Philly in early 1960s, pre-Summer of Love…no matrix, red pill please.
My dad caught polio in Puerto Rico after the war, during which he flew Corsairs. There was an epidemic, but the government told no one.
He died aged 92 from post-polio syndrome.
Maybe all those vegetables my mom tried to get me to eat when I was a kid will kill me yet, eh?
Some of them were no doubt loaded with zinc.
Sorry about your dad.
How ironic we are all gonna die of the vaccine.
I have to dispute Mr. Steele here.
Looking at deaths per 10M – COVID-19 mortality is already clearly above normal flu season levels (1000 to 2000 per 10M) even if only 2% of the affected populations in Italy and Spain. This implies a 50x increased mortality – not at all clear this is a minor effect. Note that confirmed cases as a percent of population is far lower: 0.4% or so – the 2% number comes from extrapolating upwards from the mortality using what is believed about the nCOV epidemiological mix: 200 contract, 100 asymptomatic, 20 serious, 10 hospital, 5 critical of which 1/3 to 1/2 die.
The US is showing low numbers overall (109 per 10M), but New York mortality is already 797 per 10M and still increasing.
Lastly, I would note that part of the rationale for lockdowns (which I don’t actually think are the major factor) is to elongate the infection curve, giving time both for hospital capacity to not be exceeded and for a vaccine to be developed and tested.
c1ue,
Where did you get “1000 to 2000 deaths per 10 million?
According to Worldometer they now report 5.4 per million or just 54 per 10 million globally
https://www.worldometers.info/coronavirus/#countries
I think he’s referring to Italy and Spain, although not made clear.
Hyper-politicization of climate science is now being matched by a similar reaction to this flu pandemic.
The 2009 Swine-Flu epidemic killed almost 13,000 Americans, but imposed no shut down of the country. Of that number, 10,000 had died before a vaccine became widely available. That epidemic weighed heavily on children…too young and innocent to realize the threat to them.
This Wuhan virus has a different epidemiological profile with a predilection for adults who are most aware and sensitive to the threat to their lives, and are obviously willing to do anything to protect themselves. This imbalance brings to mind Orwell’s Animal Farm: “All animals are equal, but some animals are more equal than others.”
Looking at just the USA for COVID (worldometer data) vs influenza deaths (CDC data https://www.cdc.gov/flu/about/burden/preliminary-in-season-estimates.htm) using 327 million Americans
3,756 COVID deaths = 114 deaths per 10 million
24,000 – 62,000 flu deaths = 733 to 1896 per 10 million
Worldometer includes Puerto Rico and other island territories in its US data, so over 330 million population, not that it matters much. There are also probably tens of millions of illegal immigrants.
John, You are right he is only referring to Italy and Spain which are the outliers.
Unless you throw in tiny San Marino and Andorra!
But still outliers.
Deaths per million:
San Marino 732
Italy 206
Spain 181
Andorra 155
Belgium 61
Netherlands 61
France 54
Switzerland 50
Luxembourg 37
Iran 35
UK 26
St. Martin 26
Monaco 25
Sweden 18
Channel Islands 17
Portugal 16
Denmark 16
Cayman Islands 15
Austria 14
Ireland 14
USA 11
At present 79 deaths per million, NY State would lie between Andorra and Belgium. Without NY, US death rate is 7 per million, rather than close to 12 in latest figures.
Who knows how comparable different countries’ methods are?
And in USA, NY is an outlier.
Sweden has attributed 18 deaths per million to the WuFlu virus, vs. 206 in Italy and 181 Spain.
Yet its antiviral measures have been far less draconian than other European nations.
https://www.cnbc.com/2020/03/30/sweden-coronavirus-approach-is-very-different-from-the-rest-of-europe.html
Reported deaths per million population:
San Marino 766
Italy 206
Spain 181
Andorra 155
Belgium 61
Netherlands 61
France 54
Switzerland 50
Luxembourg 37
Iran 35
UK 26
Iran’s number is not credible, and even in Europe different countries differ in death attribution methods.
US: 11
NY: 79
US, less NY: 7
CA: 4
FL: 3
TX: 1
What would be the effect of infecting someone with a single “live” virus envelope, as an alternative to a vaccine? Has this been investigates?
Would this allow the immune system enough time to develop immunity before the virus develops the critical mass to successfully incubate?
A single one, or even several thousand, would not likely do it.
There are many layers to our innate immune system that have to be penetrated for a virus to gain entry into cells, and there are only a few types of cells capable of capturing virions (or anything else), and performing the function called “antigen presentation” to another type of cell, which then must find from a near infinite multitude of possible antibody molecule configurations for one (or, more commonly, ones) that can effectively bind to, immobilize, and mark for destruction other virions as well as infected cells, which are displaying that same antigen that was used to select the antibody or antibodies.
There is a multistep and highly repeating process involved which is iterative, only generating an antibody response which is in some proportion to the size of the threat…IOW to the number of invading particles. There is then a process of amplification of the response (or dampening of it) and production of memory cells, which are what remains behind when circulating antibodies eventually wear out or become degraded.
Because the process which captures an invading microbe for the antigen presentation (A.P.) is only carried out by one small part of the overall innate immune system, most virions will be killed or digested or degraded before one of the few cell types that carry out antigen presentation can catch up with one.
Exactly what the proportions (of total virions killed to the ones captured for A.P.)are is very likely one of the highly variable parts of the immune system between different individuals, different conditions (dry mucous membranes vs moist and sticky ones, amount of antimicrobial enzymes in one’s mucous, etc), and various microbes.
Also, it takes some time for the antigen presenting cells to make their way to the site of an invasion of an infectious organism, which occurs in response to cytokines released by the first types of immune cells on the scene. And this too is proportion to the size of the threat.
I first raised these concerns and questions over a month ago, hoping maybe some researchers would see my posts on this issue both here and at other sites, and pick up the ball.
Here… I am reposting a paper which gives some info on infectious doses for typical respiratory viruses after some discussion of the subject. See table one, and note that the unit used is not virions, but what is called “tissue culture infective dose (TCID)sub50”.
This is a unit of virus inoculum sufficient to produce infection is 50% of tissue cultures so inoculated.
But no one really knows exactly how many virions are in one such unit. Estimates cited vary hugely, and they vary not just from one type of virus to another, but from one strain of a virus to another, often by several orders of mangitude.
And then often zero infections resulted, or infection but zero illnesses.
I encourage anyone who wishes to consider themselves informed on this subject to read this and other materials from start to finish, as the conclusions and summaries often contain insight one would not get from having a quick look:
The reason I mention this is that I had myself overlooked a passage near the end of this attached paper, that said this:
“In the case of norovirus and HAV, it is possible that a single virus particle is able to initiate in infection. It is, however, important to note that relatively few investigations reported the infective dose in the form of number of infective particles. A high percentage of morphologically identical viral particles in a sample, as determined by electron microscopy, will typically be non-infectious for any known cell system.”
Which directly contradicts my previous understanding of MID’s, though it is hardly conclusive that one virion can make anyone sick.
And for respiratory viruses like influenza, nothing like numbers that low was seen, with some infective does well into the millions still only making some percentage of people get infected.
Also very interesting was this comment:
“When patients acutely infected with influenza A sneeze or cough, their respiratory secretions containing high virus titer will be aerosolized. The viral titer measured in nasopharyngeal washes culminates on approximately day 2 or 3 after infection and can reach up to 107 TCID50/ml (Douglas 1975; Murphy et al. 1973). It is thought that between 103 and 107 virions fit into aerosolized influenza droplets with diameters between 1 and 10 μm (Weber and Stilianakis 2008). Considering that the airborne infectious dose of influenza is approximately 0.67 TCID50 for virus reaching the respiratory epithelium (Atkinson and Wein 2008), this shows that the influenza HID50 could easily fit into one aerosolized droplet (Weber and Stilianakis 2008).”
One aerosol droplet, between one and 10 microns in diameter, can easily contain enough virus to infect 50% of people…if it reaches the respiratory epithelium.
Reading through such literature, which contains extensive references to studies using human volunteers and live animals, wild virus types and cultures virus strains…there are no hard and fast rules.
What is true for one person and one virus is false for another person, or another virus.
Also note it is common to find people who become infected with a virus in volunteer trials of healthy adults, and yet do not become ill.
Sometimes a percentage do, and sometimes all do.
Also note, relevant to several comments here and on other threads, that it is commonly found in tests involving inoculating human volunteers, vaccinated and unvaccinated but tested to have serum antibodies, that some viruses will cause infection despite a person having circulating antibodies.
Sometimes it has been found that a far larger infective dose is required to cause infection when a person has antibodies, or the infection will cause only milder illness.
But with some other tests of other viruses, such as norovirus, there was no protective effect seen from having antibodies, or from previously being infected and clearing the same virus.
In some cases having antibodies was associated with more severe illness!
This one paper contains a large number of references to tests involving human volunteers, including some in which people were injected with blood from people with hepatitis A, and people who had 01 grams of virus infected stool delivered orally!
So there is no shortage of testing done over the years involving some brave and I would hope well compensated volunteers.
This is in direct contradiction to antivaxers here who have claimed no tests are ever done on vaccines and such.
Clinicaltrials.gov contains hundreds of thousands of records of trials, many thousands of them involving vaccines.
The paper I referenced above:
https://link.springer.com/article/10.1007/s12560-011-9056-7#Tab1
And a recent article in New Scientist with a discussion of infective dose of SARS Co-V-2:
https://www.newscientist.com/article/2238819-does-a-high-viral-load-or-infectious-dose-make-covid-19-worse/
To rephrase, would a sub-clinical innoculum of wuflu confer immunity? That would explain asymptomatic infections. People that are infected by a very small viral load.
Why not test this on volunteers?
That is a very intelligent question and observation!
Mods, I have one or a few comments waiting for moderation, for using the K word or for multiple included links.
Thanks,
and i feel somewhat vindicated that i find I am on the same page as Tom Cotton:
https://www.nationalreview.com/2020/03/the-senator-who-saw-the-coronavirus-coming/
“The CDC should not have acted like know-it-all bureaucrats who had the only medical and scientific expertise to develop tests. We have lots and lots of very capable labs all around the country,” Cotton says. “The FDA should not put all of its eggs in the CDC basket. . . . They were slow to use their emergency-use authorization.” In a January 26 appearance on Face the Nation, Cotton called on the FDA to expedite approval for testing to state and local governments.
“The bureaucracy just didn’t move as fast as it could have,” he says. “Dr. Fauci said it’s not the president’s fault. It would have happened to any other president. But it was a lost opportunity, given the time the president bought everyone with the travel [restriction].”
Does the president ultimately bear responsibility for the failures at the CDC and FDA? “He is the president, and it’s always the president’s job to push the bureaucracy when they’re moving too slowly,” Cotton says. “But sometimes you have to push very, very hard.”
Polio may not have been around for thousands of years. The first documented cases are in the 1700s. Much like TB it seems to have gotten worse over time, although the reasons aren’t clear, notwithstanding your arguments above.
An alternative reason might be that for some viruses it takes time to evolve into a more efficient killer, or maimer.
Here’s an image a polio victim from Egypt in the 18th dynasty, mummies have also been discovered which show signs of polio.
Thingadonta
I’m not sure that TB has become more virulent. It, like many other bacteria, has become resistant to most antibiotics. That is not the same as getting “worse.”
I really enjoyed this post! I too used to work at a day care. I worked at 2 of them actually and it’s definitely not easy. I applaud everyone out there right now who is still making it possible for us to go out and do certain things. Thank you!