Reposted from the Cliff Mass Weather Blog
I think I found something important.
But I will let you be the judge. And I would love to hear from any epidemiologists that read my blog.
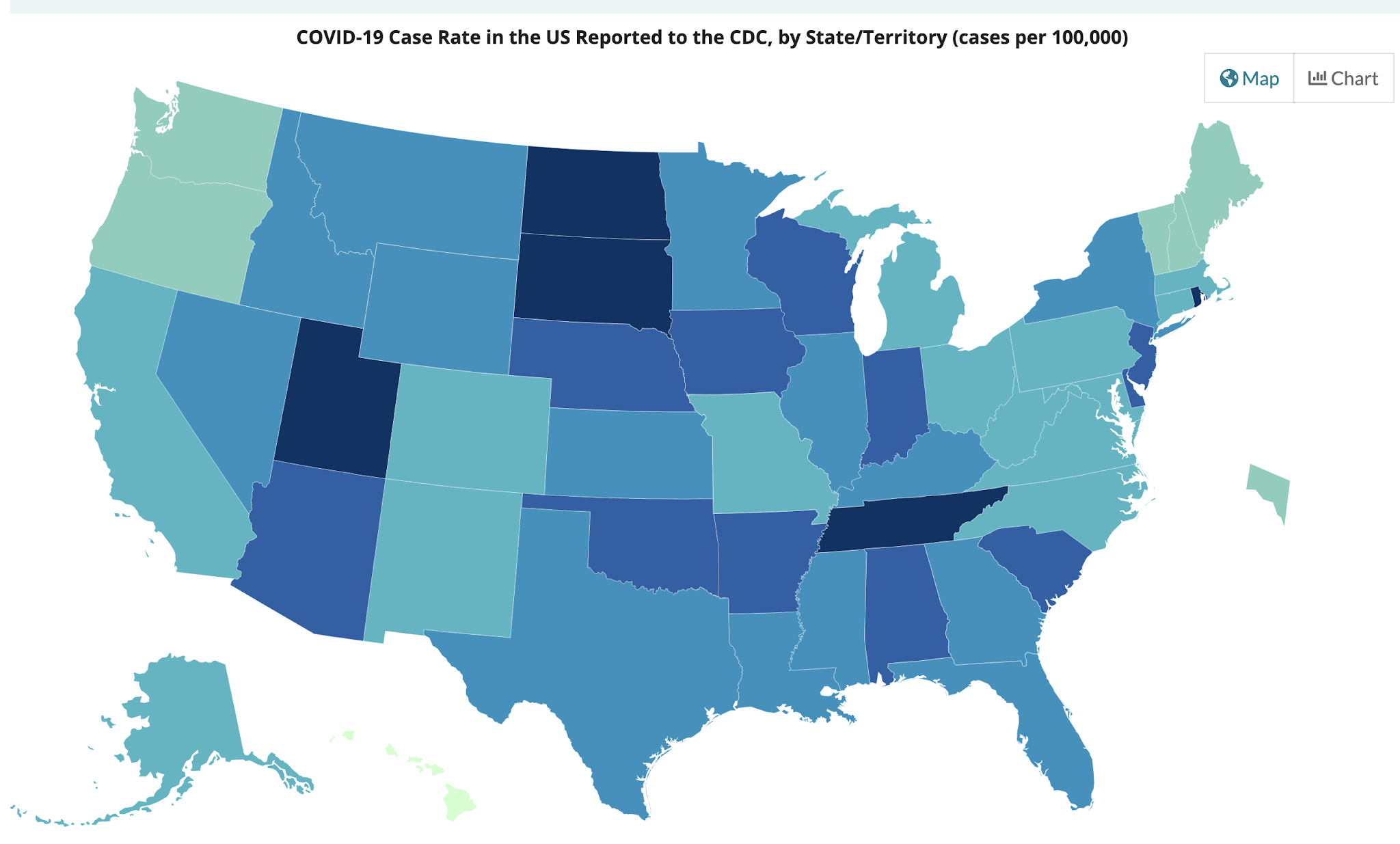
The number of COVID cases is increasing in Oregon and Washington, while most of the other states are seeing declining or stable COVID caseloads. The increases are sufficiently worrying that Governor Inslee may reverse the opening of the State.

{kind=link}
There is a lot of talk about the need to get herd immunity, in which enough of the population will be vaccinated or have had COVID so that the virus lacks sufficient susceptible people for spread. But no one seems to be sure about what percentage of immune individuals is needed. 60%, 80% or 90%. Some scientific papers and media accounts suggest we will never get to herd immunity. But what is the truth?
I am not an epidemiologist, but it seems to me that there should be sufficient information to get some real answers to the above questions. And so I sat down with a cup of coffee (actually several) and the data from the Centers for Disease Control and cranked through the numbers.
And I found something interesting.
For each state, I estimated what percentage of the population is immune to COVID-19 and then I compared that to the change in the number of new cases over the past few weeks.
I found a significant relationship between the two. And I may have discovered the magic herd immunity percentage.
Estimation of the Percent of the Population Immune to COVID-19
First, I started with the percentage of each state’s population that has been reported to have had COVID-19, which ranges from roughly 4 (Oregon) to 14 (Rhode Island) percent.

{kind=link}
There is an extensive literature suggesting the actual numbers of infected people are far higher than the official case numbers, with several research papers suggesting that a factor of three is reasonable. So I started by taking the CDC state case percentages and multiplying by 3.
Then I secured the vaccine data for each state, and based on the CDC numbers of single and double vaccinations, I assigned 60% of the total vaccinations as the number of people that have gotten at least a single shot. I then added this number to the 3 times case percentages noted above, to get a final fraction of immune individuals for each state, with numbers running from .56 (Oregon) to .936 (Rhode Island). This will undoubtedly be a bit of an overestimation because there will be some people that have had COVID that are vaccinated, but that would only shift my estimates of herd immunity by roughly 5-10% at most. In any case, the approach is consistent for all states.
That Change in COVID Cases for April 15-April 28th
My hypothesis is that increasing percentages of antibodies for COVID should be related to declines in COVID case numbers. Sot I next turned to the CDC COVID trends pages.
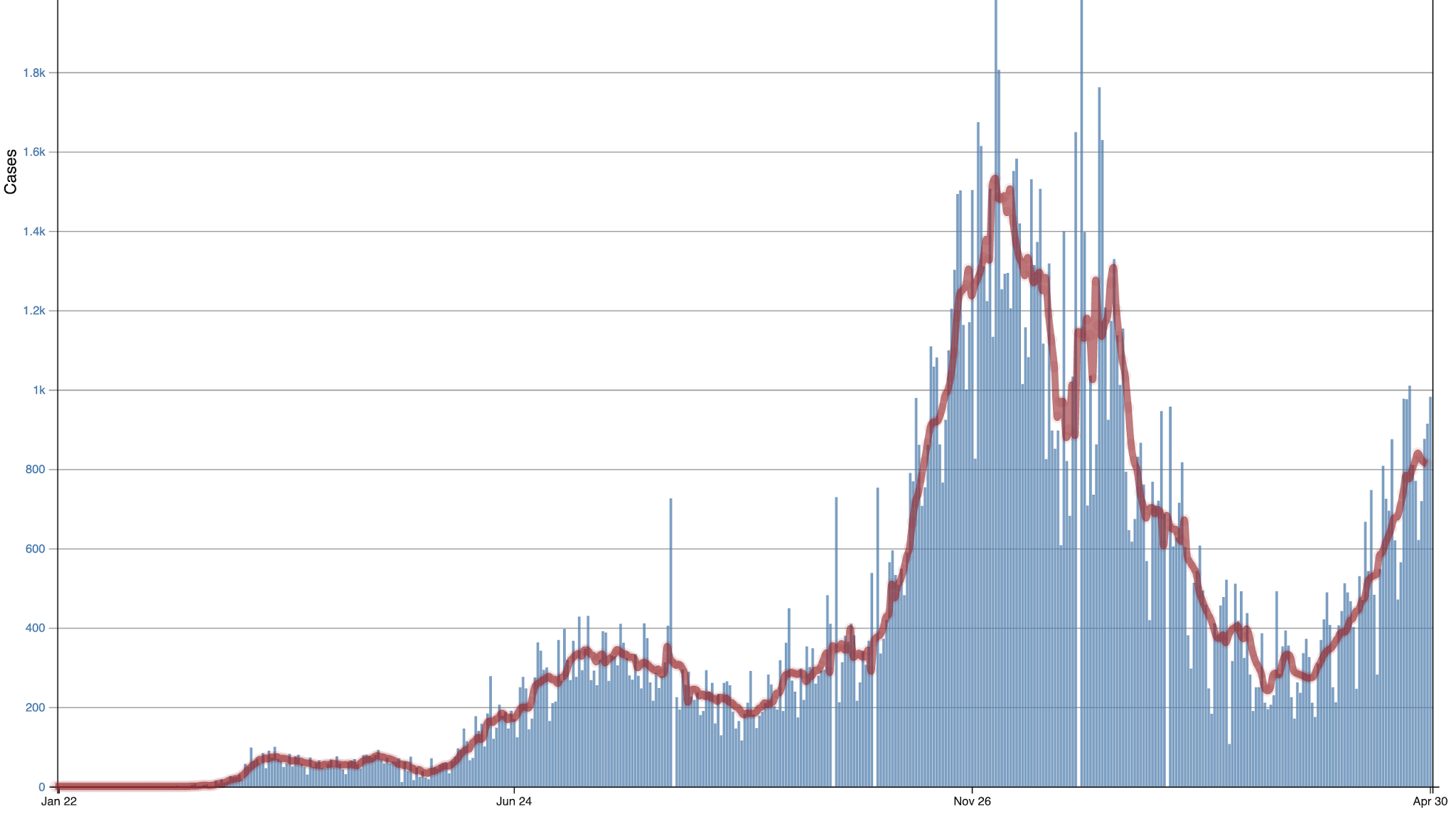
Here is the one for Oregon. Not good. Cases have been rising quite a bit (blue are daily values) and red are 7-day running means).

Oregon
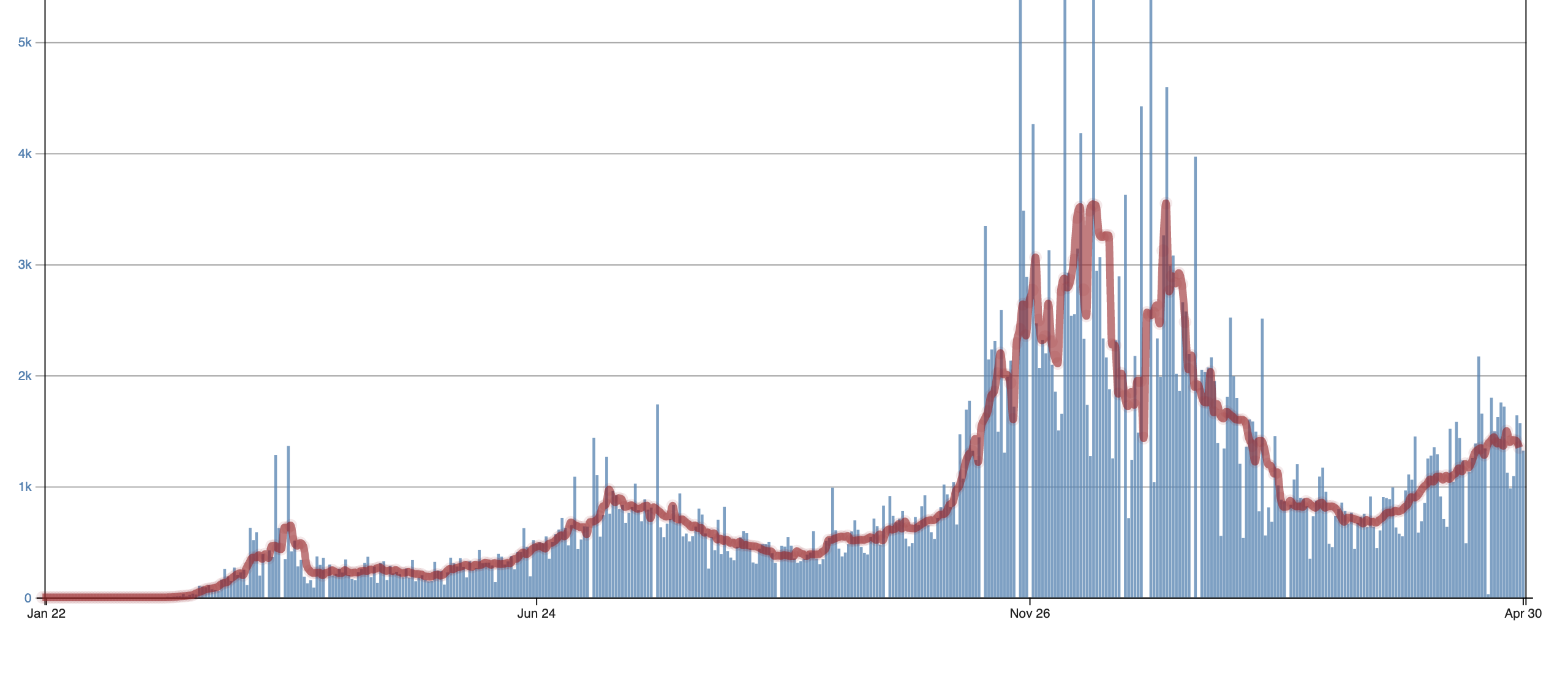
For Washington State, the situation is a little better, but still going the wrong way. This is why Governor Inslee is threatening to clamp down (and I will suggest later that this would be a mistake).
{kind=link}

Washington
On the other hand, Rhode Island and Massachusetts are seeing rapid declines. Can we understand why? I think we can.
Using the CDC trend plots and accompanying numbers, I found the changes in the number of cases for roughly the last two weeks (April 15 to April 28th), using the red lines (running 7-day means) shown for each figure. Then I compared the recent case number trends in each state against the fraction of state citizens that were immune. The results are shown below. And they are exciting and make a lot of sense.
The Y-axis indicates the change in the number of cases per 100K residents and the X-axis is the fraction of state citizens that are immune. Each dot is a state.
The two states with the largest INCREASE in COVID cases for that period are Oregon and Washington! And we are the states with the smallest percentage of immune individuals.
But once you get above .65 there are no significant increases in COVID. But what REALLY is significant is that the big drops in the number of cases start abruptly around .7, at which 70% of individuals are immune. Something very special is happening at .7 and it appears it represents the transition to herd immunity.
{kind=link}

Now you may ask why some states are above .7 but are not showing recent changes. I believe there are several reasons for this. Some of these states made the transition to herd immunity earlier than two weeks ago. Once a state transitions, numbers fall and stabilize. Another possibility is that a major reopening of a state can temporarily maintain current COVID levels.
But there is a clear message from the above. Once you get to .7, the expansion of COVID is over and a collapse of the number of cases is possible.
Now there is a potential message here for Governor Inslee in all this.
Washington State is on the verge of reaching a sufficiently large percentage of immune individuals so that COVID cases will first stabilize and then rapidly decline. At the large rate of vaccination being given in our state (about 60,000 per day according to the WA DOH website) plus the natural spread of the virus, we move from ~.63 today to .7 in roughly a week. Do we need to add restrictions at this point?
{kind=link}

There are other factors that may well contribute to a major decline in WA state Covid numbers during the next month or so. We are now entering the warm/dry portion of the year, with people spending more time outside and opening their windows. As noted in an earlier blog, outside air is very COVID safe. Second, vaccinations are now available for younger people, exactly those who are contributing much of the transmission of COVID.
Does the above analysis make sense? Why haven’t others done similar number crunching? Let me know if you see any flaws in logic or approach. But it all seems logical and the picture is coherent and self-consistent.
My first reaction is that “herd immunity” should be directly related to R-Naught of the virus. The R-Naught of SARS-CoV-2 is supposedly higher than that of most Flu viruses, so I would expect the herd-immunity to be higher as well. Your results might be affected by your assumptions – more people may be immune then you account for – this would account for the higher R-Naught.
Secondly, there is more than one strain of SARS-CoV-2 being passed about, and some of the newer variants have a higher R-Naught. This will greatly complicate achieving herd-immunity, especially if a person can get the disease more than once (by having different strains). If some states are mostly affected by the first strain, while other states are mostly affected by later strains you will not be able to make accurate predictions – they may behave differently requiring more immunity.
So, you have timing, strain, and actually immunity to estimate as best you can – that’s a lot of chances to introduce error. This is likely why it hasn’t been published – for fear of it being so far off the mark.
Chi-Vi supposedly has R0 of ~2.9 (2.4-3.4) so theoretical herd immunity threshold is 1-1/R0 = 65.5% (58%-71%). So your ciphering seems to fall within expectations, whether by skill or luck..
https://nicholaslewis.org/herd-immunity-to-covid-19-and-pre-existing-immune-responses/
Thanks for that reminder. Herd immunity varies depending upon a lot of assumptions you make about the population.
Apart from the idea the NO ONE had any level of immunity at the start of 2020 and the entire world was naive to the virus, the second largest mistake was to assume trivially simple uniform population distributions.
When dealing with exponential growths, the slightest error in your model initial conditions or assumptions and parameters, quickly leads to meaningless projection.
I hate to point out this we have been here before, with another set of model projections !
Mmm – technically, some people had immunity from something else in their past.
Coronavirus are not new – many cases of the common cold are caused by some, and there was SARSv1.
The perennial killer INFLUENZA is related though not a corona virus.
Superseded by events. Unfortunately totally wrong.
Explain remark please?
I assume Chi-Vi is the strain that came to the US (partially throught Italy too). What are the R0’s for the more contagious strains, e.g. the UK and India strains?
Chi-Vi = China Virus
From blood tests for T-cell 18 years after Sars 1, people were still immune. Moreover they also reacted to the current virus. The previous virus is more than 20% different as to genetic code. The various ‘varients’ are at most 0.3% different from each other.
The above from a now banned utube video by Michael Yeadon.
The varient story is Fear Porn.
The whole concept of R0 implies that you have a population totally naive to the virus. That is the definition of R0. That was one of the biggest false assumptions the “experts” made in analysing the epidemics and why their alarmist estimations were so grossly wrong.
Salute!
Great point, Greg.
Here in Florida our initial cases were old people and recent tourists from Asia.
We did not incur a strong increase in cases that were expected after the spring break (keep in mind it is very hard for the particle to fly in a ten mph breeze on the sunny beach).
Most of us figured we had some degree of resistance from seasonal cold/flu exposure and the annual flu shot. In other words, our populace was not virgin, open for business customers. Then there are folks with strong immune systems that had the ability to fight and beat the virus.
Gums sends…
Florida commendably saw the less on from Italy so acted to quickly and assertively for care residences/nursing homes.
Starting with those facilities having deficiencies in the last review.
(Some care residence chains in Canada acted quickly when they read news of a new illness in Communist China, knowing it would arrive in North America before long. Besides the usual measures they continued to pay aides who were ill and told to stay home. And quizzed/tested aides for at least temperature and illness at the start of each shift.
OTOH gummints like BC, ON, PQ, and NYC did not.
Once it was realized that aides were working in more than one facility, the Fraser Health Authority took over a week to stop that, whereas a private facility that had some subsidized customers this government employees aiding stopped that within 24 hours – hired private nursing.
https://www.ctvnews.ca/health/coronavirus/nobody-died-in-these-nursing-homes-what-did-they-do-right-1.4998204 REF early and aggressive
There’s no issue with accuracy when publishing doom and gloom model studies.
Daily new cases in OR have been falling since April 23.
Oregon COVID: 186,344 Cases and 2,501 Deaths – Worldometer (worldometers.info)
As I said, daily new “cases”, however defined, have fallen since April 23. The peak number of course was in Decmber.
Good analysis and makes sense from a layman’s perspective.
The flip side of this is just who is getting CV at this late stage of the pandemic and are these people at any more danger than just getting the flu? If the people at high risk have been vaccinated and younger, healthy people end up being those behind the rise in infections, does it really matter infections are rising short term in some states?
true that
https://www.worldometers.info/coronavirus/usa/oregon/
OR new daily cases have peaked again now but daily deaths did not seem to increase in this recent wave.
Of course deaths tend to lag 2-3 weeks but so far so good.
It would be interesting if they chart a histogram of ages for the recent new cases and compare it to similar histogram from the larger December wave.
75% of the new cases are college related.
So, death rate will likely be less
That herd is contributing to global warming, but Chinese might have a ‘different’ solution in getting rid of it, no, not another Covid virus, but something more substantial and instant
Huge rocket looks set for uncontrolled reentry following Chinese space station launch
“The Long March 5B, a variant of China’s largest rocket the 22.5-metric-ton Tianhe module was launched from Wenchang on Thursday . Tianhe separated from the core stage of the launcher after 492 seconds of flight, directly entering its planned initial orbit.
….. means the rocket body passes a little farther north than New York, Madrid and Beijing and as far south as southern Chile and Wellington, New Zealand, and could make its reentry at any point within this area. ”
https://spacenews.com/huge-rocket-looks-set-for-uncontrolled-reentry-following-chinese-space-station-launch/
Skylab and Mir all over again. Maybe the best thing that could happen would be for it to land on the Chinese Space Agency building. All in all the chance of it falling on your head is very small, but if it does it will be 100% a bad day.
Cliff is neglecting the fact that multiple studies have shown that, in many places, about 30% of people have existing T-cell immunity to SARS-COV-2 probably from a different pre-pandemic corona virus infection.
We have to keep our eye on the ball. The only two reasons for shutdowns were to lower Covid deaths and prevent hospitals from being overwhelmed. Covid deaths in Washington (and in the US as a whole) have plummeted and hospitals are no longer at risk of being overwhelmed. We’ve already achieved this by vaccinating most of the elderly.
This paper says it’s much higher than that (some preexisting T cell immunity).
https://www.nature.com/articles/s41590-020-00808-x.pdf
Reading between the lines, don’t expect the “vaccines” to help much.
“Vaccines”!
What “vaccines”, mate.
Oh, well, think I, see what you done there, maybe, or maybe not!!
You, you…
👇✌😛
cheers
T cell response does not equate to immunity but rather may make difference between potentially fatal infection versus mild or moderate infection.
The key statement in the abstract:
Unfortunately for the layman it is hard to interpret exactly what this medtech-jargon means. Obviously if 81% are of uninfected are truly “immune” this virus would never have gotten off the ground. If this just means 81% have some response enough to limit health consequences to the trivial then that makes a lot more sense to me.
I have always suspected common cold coronavirus exposure within the past 3 years (which probably constitutes 20-30% of the population) may give sufficient immune response to limit the Chi-vi infection to mild or asymptomatic.
It would have been an interesting experiment, back in early 2020, to simply identify 10,000+ people who had contracted coronavirus type colds and then monitor them to see how they fared with the Chi-vi. I’m not even in medical field and I thought of that idea, surely someone in the field could have thought of that and push for it?
Ok let’s put it this way.
Still, regardless of all known things about
T-cells activity as per means of immunity,
still there is more to it…
cheers
Most adult colds are caused by four coronaviruses, two of which belong to the same genus as the WuWHOFlu virus.
These new vaccines certainly don’t equate to immunity.
no, they dont!
but the amount of over 50s+ here getting the jab this week and thinking they ARE going to be immune is pretty sad
medicos just dont realize recipients feel teflon coated and may well be at risk later on
THe 81% number explains why the Diamond Princess had only a 20% infection rate. I think we have made some huge mistakes dealing with this virus.
But we had the best advice from experts that money could buy! 🙁
Yes, experts that money could buy, what’s that Fauci highest paid guy in the us govt making?
i think about $440,000
throw in the patent payola per vaccine onto that
59% of the crew and passengers of the Antarctic cruise ship tested positive for COVID.
https://thorax.bmj.com/content/75/8/693
After the initial spread grew rapidly, the passengers on the Diamond Princess were isolated in their cabins which helped contain (but didn’t completely stop) the spread.
“I have always suspected common cold coronavirus exposure within the past 3 years (which probably constitutes 20-30% of the population) may give sufficient immune response to limit the Chi-vi infection to mild or asymptomatic”
That is what that section is saying.
last para, yes someone finally DID think of it and it does appear as if common cold fairly recently IS a good protection via immune reminder
of course trying to CATCH a proper cold right now is a big task..unless you have kids
I have not caught once since I started tanking Zinc Quercetin and vitamin D. And I have been around other people with a cold.
You’re right ! What vaccines. It would be better to call them “Brain and myocardial venous thrombosis inducers”. The list of people who have died or had experienced serious side-effects (sometimes permanent damage) is getting longer and longer.
Exactly. Though case rates are important to determine herd immunity, that’s all it’s good for. The data that matters is hospitalization and case fatality rates. When media talking heads breathlessly report the latest new cases, push back and ask about the number of hospitalizations and fatalities which is a small fraction of the new cases. Around 97% of people who get COVID-19 recover, most with relatively mild symptoms. Of the ones who are hospitalized or die, most are elderly and/or obese or are immunocompromised. There is no question about who is at risk. The rest of us? Take off the stupid masks. They do nothing.
Damn You and your common sense and applying the scientific method. Young and Healthy? more likely to die from just about anything other than COVID-19… Variants are just a scare tactic to keep the gravy train rolling for big Pharma and HC industry as a whole. We now know from long term studies Masks are useless, the virus does not live on surfaces as a means of transmission and those who have recovered have near 100% immunity from any related Coronaviruses. Skip the needle , eat healthy and exercise!
I wonder whether it is possible to get a definite answer to that question for another couple of years when it is all over, when the epidemic has finally run its course – and we can sit down and observe the true facts and statistics about Covid 19. We simply do not know enough about this particular virus.
One thing they should look at is, why are the number of “cases” going up, as soon as the “vaccinations” started?
Why are people in nursing homes, who survived the first round,and got both doses starting in December, now dying?
Also, why is it that jurisdictions with the toughest lockdown and masking mandates, keep having increased “cases”?
In Ontario, we got new lockdowns, just as they started mass vaccinations and the “cases” went up. Then they increased the lockdown measures, and the “cases” went even higher. Meanwhile, I still know only one person who got a little bit sick.
In 2003 I had two deaths on my street from SARS, which only killed 44 people in Canada.
Something doesn’t feel right here.
Could this be evidence of antibody dependent enhancement that some have warned us about?
Sorry to spoil it for you;
but by the way, as per the way of your quarie, it could be every way possible there,
as possibly every thing or any other way you ever imagined, in your space and time,
either of it been in a fantasy or fiction sand box environment.
It is weird, yes, I know!
(Not really sure though)
cheers
What do PCR tests detect? What do the mRNA vaccines do?
What do the mRNA vaccines do?
—‘
Provide the ever best ripoff at large platform,
for the ‘smart’ post modern thieves.
Simple as that…
The rest is simply a story told vocally and sensitively, by the victims in the very merit of the prospect of the victims!
Painful, but still jolly!
Hilariously so!
cheers
RT-PCR tests detect diagnostic genetic material, ie viral RNA transcribed into DNA.
https://discoverysedge.mayo.edu/2020/03/27/the-science-behind-the-test-for-the-covid-19-virus/
Reverse transcriptase was discovered by Howard Temin and isolated by David Baltimore in 1970, for which achievement they shared the 1975 Nobel Prize, with Renato Dulbecco.
An mRNA vaccine against COVID-19 delivers the genetic instructions for our cells’ ribosomes to make the ChiCom virus’ spike protein. Our immune system then builds antibodies against this antigenic protein.
The adenovirus vector vaccines use DNA.
The PCR gives many false positives and can even be easily manipulated to give a false positive.
From the inventor of the PCR test.
“…So to start, it is very remarkable that Kary Mullis himself, the inventor of the Polymerase Chain Reaction (PCR) technology, did not think alike. His invention got him the Nobel prize in chemistry in 1993.
Unfortunately, Mullis passed away last year at the age of 74, but there is no doubt that the biochemist regarded the PCR as inappropriate to detect a viral infection.
The reason is that the intended use of the PCR was, and still is, to apply it as a manufacturing technique, being able to replicate DNA sequences millions and billions of times, and not as a diagnostic tool to detect viruses.”
COVID19 PCR Tests are Scientifically Meaningless Though the whole world relies on RT-PCR to “diagnose” Sars-Cov-2 infection, the science is clear: they are not fit for purpose
https://bit.ly/36vkZ7I
Jun 27, 2020
in Aus being run at 40 or more cycles FFS!
35 or so in uk n usa was already way past sane levels from what I read anything over 20cycles you could find anything you wanted
The hospital close to me runs 45 cycles. The Independent lab runs 40 cycles. In Florida the cycle counts are required on the results certificate. They seem to understand the science there rather than science based hysteria!
My reading of this UK report is that, stratified for risk (vaccine tier), the mortality in those who get covid after vaccination are about 25% more likely to die.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/982499/S1208_CO-CIN_report_on_impact_of_vaccination_Apr_21.pdf
I doubt it. This has been a political issue from day 1 and, as such, all the data is being “managed” by political hacks. Were “COVID deaths” really deaths from the Chinese flu? I don’t think that’s anything that we’ll be able to sort out by looking at records that may or may not be accurate. Where “cases” really instances where people had the virus or were there lots of false positives? How do you figure that out after the fact? Where agencies and NGOs who’s grants and funding depended on finding what their benefactors wanted them to find accurately and honestly tendering unbiased data?
There will be plenty of claims in the future, plenty of statistical analysis that “proves” things on both sides, but I doubt we’ll ever really “know”. This has been way to politicized to unclutter it enough to make definitive determinations in my opinion.
Indeed, Sailorcut.
CDC Admits Hospital Incentives Drove Up COVID-19 Deaths
https://bit.ly/3l1aCwP
August 21, 2020
According to Occasional Cortex you can now petition the US government to reclassify deaths as Covid….🤔
Not disagreeing with any numbers or calculations. Just pointing out that there many be different percentages to reach herd immunity in different states based on how spread out the populations are. In a state where most of the population is located in large cities, it would make sense to need a higher percentage for herd immunity. A state with a population that is spread out in small towns and farming communities might need a lower percentage for herd immunity.
Yes, there are several factors, including environmental humidity, temperature and sunshine, in addition to demographic concerns.
Agreed. I think these additional factors (demographic and environmental) have been ignored or severely underestimated in dealing with this virus.
Karen, that would seem to be a good point and to make sense, except, how then to explain the high numbers of COVID on the Reservations which are largely very rural and have low populations? One might assume that the Native Americans are more susceptible, I suppose, but I wonder if that tells the whole story? I have no idea, just wondering. It is something that should be studied, I think.
Michigan went through a significant spike in the number of cases recently. We were in a partial lockdown with no easing of the lockdown at the time. The weather was not very nice, so it wasn’t due to people getting out and about more. It seems blue states are just places where everyone gets COVID-19.
The Gov. claimed that was because of all the spring breakers coming back from Florida. Funny how only people from Michigan went to Florida (and how nobody from Florida stayed there…)
The Governor of MI. secretly went to Fl. to visit her father and broke her own rules. Maybe she brought it back to Michigan? 🙂
That MI surge was suspiciously confined within the state borders. So, I think that some artifact in testing/counting/etc. that is unique to MI is responsible for the “surge”.
Minnesota had a similar surge. Lower total population so the numbers weren’t as big, but the percentages were similar. No states around Minnesota, including Wisconsin which is located between Michigan and Minnesota, saw a similar jump.
This just in; the CDC has recently said it’s ok to take off your mask at night when you go to bed, and also while in the shower or swimming.
Whew, what a relief.
Jeffrey Toobin has a question.
But Joey B says it is patriotic to wear your mask.
Some observations.
Rud,
To my mind the jury is still out on #4, at least as far as longer term side effects are concerned, but for older people and those with compromised immune systems, the risk seems worth it to me. If I were younger, say under 30, I would probably take a wait and see attitude. People between 30 and 60 have an interesting decision to make and I wouldn’t criticize them either way.
We are going to get the Janssen one shot once it finally becomes available here. Is a known viral vector platform in production for over 10 years: HPV. Uses a modified human cold corona as vector ( cannot multiply in you, only in the cell culture used to grow the virus into which the Coid-19 stuff is added). mRNA is new so without any long term safety data on, for example, the nanolipid encapsulants. We are over 65, thankfully with no comorbidities. The 15 million doses spoiled by the contractor in Baltimore has set back our plans.
My son and daughter in law were able to get the Janssen vax in Chicago last week because both ‘sort of’ (but not really) fit high priority group definitions for those under 50 in Illinois. No problems, not even mild side effects. My daughter and son in law are waiting to be able to get the Janssen vax out in Colorado. No priority group, and otherwise too young. Not available in Colorado yet either.
Paul,
Rud is actually evolving and successfully growing,
even at his old age.
Surprisingly, yes, but still you know, miracles do happen sometimes…
luckily.
This is more like a good sign,
like it not been, an actually definitely ugly one.
Fingers still crossed!
Never knowing, till….
👇✌😛
For the benefit of the all smarties there, trying to figure it out…
The above simply stands as another expression of;
LOL
Oh, well… this:
👇✌
stands for, well… the “42”…
Stop freaking fracking your “time”.
griff, really love you body.
🙂
cheers
A sphincter says what?
whiten,
I can’t tell if you took too many drugs, or not enough, but you aren’t coherent either way.
are you crazy. It is still experimental and unlikely to ever reach efficacy of either 2 dose vaccines.. If you are under 50 , or relatives under 50 pass , this is one big mistake.
What you need to know:
Fauci is a bureaucratic fraud.
HEY! Is that anything to say about a man who has been right about everything?
Of course, he has also been wrong about everything. Pick your day…
Sticks his wet finger up into the breeze to figure out what to say next…
What’s it wet with? If he’s wearing his face mask, which he always does (at least in front of a camera), then he can’t get it in his mouth to wet, so instantly the question becomes, in which orifice did he wet it? *shudder*
A broken clock is correct 2x per day. I’m afraid Dr Fauci record is worse than broken clock 🙁
Speaking of Fauci, et al.
https://news.yahoo.com/unlikely-america-reach-herd-immunity-133326123.html
But WSJ just had an article about the 1957 Asian Flu epidemic, which followed an earlier horrible polio epidemic. I survived both, two classmates in high school died from polio before vaccines. Both handled much, much better than the current one.
WSJ article also covered in last TWTW. https://www.wsj.com/articles/how-a-more-resilient-america-beat-a-midcentury-pandemic-11619794711
I listen to real life and death doctors, not armchair types.
the second item was written BY the dud Ferguson…did you realize that?
Besides the ad hominem “dud”, do you have any arguments about the contents of the article?
Carlo, I disagree about Fauci. He’s a great bureaucrat but he’s a colossal scientific fraud.
The variants aren’t doing much to T cell response. I have found at least 5 or 6 papers that confirm as much…here is the latest.
https://www.technologynetworks.com/immunology/news/sars-cov-2-variants-still-recognized-by-t-cells-347278
“It was a Fauci induced mistake to ‘quarantine’ everybody—the young and healthy—rather than only the elderly and those with known comorbidities of obesity and diabetes.”
Amen, Rud! It was, also, a mistake to not encourage Vit D for people with dark skin above, I think, the 34th or 35th parallel. There seems to be good evidence for it’s benefits in protecting people, esp., darker skinned people who have difficuty absorbing Vit. D, esp., when in Norther latitudes. The Scandinavian countries all supplement their citizens with Vit. D.
Interestingly, I discovered Medicare will not pay for Vit. D level testing. Given what we know now, that seems to be a mistake and very short-sighted and not just in regard to COVID.
Once again eveyone seems to be tiptoeing around the elephant in the room!
Why are therapeutics like ivermectin and HCQ not readily available for suppressing the symptoms of the ChiCom virus while allowing individuals to develope immunity? The latest meta analysis of ivermectin that I read showed an 80% reduction in fatalities when taken early in the illness, and an 85% reduction when taken as a prophylactic!
The estimates of lives saved by using therapeutics worldwide is over 1 1/2 MILLION!
In the US that would be somewhere in the 200,000-250,000 fatality range!
I know that the virus served a higher purpose by helping get Trump out of office, but the sainted Tony Fauxi needs to be grilled long and hard about the gain of function experiments he helped YOU pay for and the connections he has to the pharmaceutical companies who are making big bucks due to the “lack of effective treatments!”
The cowards in our media and political circles are allowing the CCP to get away with a devastating act of war by killing millions and destroying economies without bullets or bombs!
Great question, and even vitamin D supplementation would have a significant benefit.
Perhaps the best therapeutic yet – Leronlimab, aka PRO 140 or Vyrologix – has shown both incredible efficacy and safety (no significant side effects), yet the FDA will not grant an EUA. The company that makes Leronlimab is in Vancouver, WA, and they are now trying to get approval to sell in Canada, the UK, the Philippines, Brazil, etc. The FDA has approved horrible drugs (see Remdesivir) with little efficacy and significant adverse side effects because they are produced by big pharma companies…and big pharma companies pay between 40% and 70% of the FDA’s bills (and frequently swap personnel).
Bottom line, if anyone gets a bad case of COVID 19, work with your Dr to try and get approval to receive Leronlimab, it has saved many at death’s door.
That’s easy to answer. Under FDA guidelines none of the vaccines could have been granted EUAs if there were likely treatments already existing. They had to be dissed and marginalised.Fauci has known since 2005 that HCQ worked on corona viruses.
But without an EUA, no kaching!!
Yes! I don’t have the link but I believe someone on here referred to a vid with Dr. Peter McCullough to the texas health board? where he states that he believes 400,000 could have been saved. Sooner or later someone with the MSM or the ‘right’ cridentials will go after this.
Cliff, what test is being used in Oregon and Washington? A Positive test is not the same as a case but this is frequently used to multiply numbers and make it look worse. You might want to review some of Dr. Sebastian Rushworth’s essays, he has been writing quite a lot about Covid. https://sebastianrushworth.com/
Good question. It is mostly a PCR test. However, Oregon Health goes deaf when people ask how many iterations are used in the PCR test that Oregon uses. It is impossible to get an answer. Some consider that it is likely that Oregon runs the tests for a far higher number of cycles than is reasonable, in order to generate a lot of false positive results.
This may well be true if you look at the number of hospitalized cases, actual numbers rather than percentage of beds available – a lot of available beds seem to have just evaporated recently, and the percentage of beds occupied is reported higher, mostly because of the “loss” of beds rather than more cases being hospitalized. Compare the actual numbers of hospital cases to the reported case count, and it looks like many fewer people are actually getting sick and dying from COVID-19.
These inflated numbers allow the governor to maintain her “state of emergency”, and get more money from the federal government.
Unexpected detection of SARS-CoV-2 antibodies in the prepandemic period in Italy – Giovanni Apolone, Emanuele Montomoli, Alessandro Manenti, Mattia Boeri, Federica Sabia, Inesa Hyseni, Livia Mazzini, Donata Martinuzzi, Laura Cantone, Gianluca Milanese, Stefano Sestini, Paola Suatoni, Alfonso Marchianò, Valentina Bollati, Gabriella Sozzi, Ugo Pastorino, 2020 (sagepub.com)
Covid 19 antibodies found in blood samples taken as early as September 2019(Italy)
Covid 19 likely to have arrived in Europe during the late summer of 2019.
I heard there was a fair bit of flu during the winter of 2019/20
Yep and there is guy on Twitter that has some reasonably compelling arguments that it all started in 2018/2019 in China with lots of immunity conferred to Oceana, Asia, and Africa based on their proximity to Chinese citizens. Even tracks a significant reduction in CO2 in 2018 in China that was similar in magnitude to the drop in CO2 during 2020.
https://twitter.com/EthicalSkeptic/status/1389271873142366210?s=20
This was a calculation I had done way back in February of 2020… if there had already been enough cases to notice a trend in “sticky pneumonia(?)” and visit enough patients to obtain enough virus for a DNA analysis/mapping by mid-January, that the ChiComs ordered destroyed and locked up on about January 30(?), then patient zero was at least 6 weeks before the collection of similar cases became apparent. I’m thinking it took at least 6 weeks of research to be able to map the DNA. Do that arithmetic and 6 weeks before mid-January is early December, 6 weeks before that was mid-October… That’s the conservative estimate, the Wuhan Flu (I refuse to be PC, I’ll call it the Wuhan Flu if I damn well wanna) had to have been in existence and spreading before mid-October 2019. Another data point, I can’t find the link now, but news came out of California(?) that a death that occurred there in early December 2019 had tested positive for Wuhan Flu.
I would need to see more facts to back it up, if the Wuhan Flu already existed in the wild in Italy as early as Sep 2019, there may be something to the Chinese claim that they got it from somewhere else, but I wouldn’t bet any money on it. The commercial link between China and Italy was already well-known before Trump banned any flights from China, so it’s highly more likely that the Italy cases, even the earliest one(s), came from China where it originated, rather than the other way around.
The first traces in Italy had much earlier manifestation in sewage plantsin spring 2019 or evenearlier, don’t remember exactly
absolute stonker of a flu or two going round Aus in the march and october 2019 remember the months cos i had either both or the same on twice(unlikely) and it was savage pneumonia both times.
actually got a pneumo vax in march 20 because of that and its rare I ever accept a vaccine. ive Had most of the bugs they hand em out for anyway;-/
I do not want or mean to spoil it for the herd immunity lot… dummies.
It,
herd immunity does not really care or depend on your opinion.
Was there as a matter of fact, long before you all silly lot, were even born or conceived… and still there, it is,
regardless of all silliness and stupidity at large out there.
Grow up.
Sorry, is just what it is.
(side note to the self…
“please, please, for goodness sake, stop;
“dwinking and twyping””, you
“fool twoat!”)
🙄
cheers
What a load of gibberish.
Yes, true.
And I love it.
You in the other hand,
keep crossing you fingers, and really believe in your own skill of literacy!
Thank you… appreciated!
Can’t do cheers though, to your lot.
Weally sowry, Pwetorian.
bye now,
hopefully, fingers cwossed…
…no need to come back…
please stay a way… will definitely not be missed… assure you…
believe it or not…
it is truth!
“God, for the sake of goodness, save us from the imbeciles and the literate stupids… whatever that means…
please if it is not too much to ask!”
Please take your medication and head back to bed, sir.
Tom, with all fairness,
how sure are you that somehow I am in medication treatment?
You using the best of your mental brilliance to somehow figure that out,
isn’t it Tom in Towonto.
Sorry to break it to you
Tomy in Twonto…
am not in any medical treatment yet Tomy boy in Towonto.
No any physical or otherwise problems up to now for me Tom in Towonto.
What about you Tomy,
how much it hurts for you Tom in Towonto?
Do not lie to your self, “boy”!
cheers
I think someone needs to do a wellness check on whiten.
I have fracking wasted years of my lifetime,
for the sole purpose that somehow I get a fair check on my wellness.
Can’t blame Anthony though.
But thanks for bringing it up, lost soul…
Oh well you believe not on soul matter… or silly things like that!
Sorry my bad to you, lost one…
obvioulsly a lot of waste of time…there,
but you see, I can afford it.
Can you?…
really!!!
cheers
Hmm. Alcohol and typing certainly don’t mix.
Really?
Yes
I think a lot of the people that have had covid are taking the vaccine. I am in a group of people that got hit hard with no deaths a year ago. Thankfully. Of the people that know they had covid 4 out of 10 have taken the vaccine. Out of people who think they probably got covid but are not sure 5 out of 5 have taken the vaccine. And of those that know they didnt get the wuhan covid 4 out of 9 have taken the vaccine. I suspect at least 50% to 66% that had the wuhan covid are going to take the vaccine in wa state. They will do this because
1) There is a lot of propaganda encouraging this.
2) Their employer is pressuring them
3) Even if you had it you can still test negative to antibodies so you dont have proof
4) You didn’t show symptoms.
5) You were sick but it could have been a cold.
Lowell,
It is a violation of the Nuremberg Code to force people to take experimental medications! The federal government cannot legally require it (although they’d love to,) but they can pressure businesses and corporations and schools to mandate these “vaccines” for all without breaking the letter of the law!
We are currently in the midst of the biggest government promoted medical experiment since the Psychedelic Era was kicked off by CIA agents turning Leary and others on to LSD! Why these drugs are so important is an interesting topic, but my spidey senses always kick in when the government seems intent on getting vast swathes of the public to do ANYTHING!
I hope that there are no long term problems from them, but the number of blood clotting problems and other adverse reactions make me wonder if Operation Warp Speed may not turn out to be the biggest blunder of Trump’s career!
There was NEVER any reason to rush the vaccine development EXCEPT that use of effective therapeutics to quickly attain herd immunity could have been seen as a win for Trump!
A number of universities in Colorado will require all students and faculty have the WuFlu jab before fall semester.
One can submit a form for a religious or medical disability exemption. At the university of Colorado, I understand that the form is under development.
Personally, I don’t understand why one would need an exemption to get out of taking an experimental therapy as this would mean that the university is requiring a “vaccine” not merely recommending one.
Very little of any of this whole virus deal makes any sense.
You’ve just got to look at it through the right lens!
The CCP got to get rid of Trump, who was punishing them for bad behavior, they got to cripple the Western economies and make them even MORE dependent on China and it’s slave labor system, and they were finally able to crush the rebellion in Hong Kong with little international censure!
The DemoKKKrats got rid of Trump, stole a tiny majority in the Senate as well, destroyed thousands of small businesses that bridle at government regulations, and killed off tens of thousands of older Americans who tend to vote more conservatively!
What’s not to like about the benefits provided by ChiCom-19?
A number of Republican governors and legislatures are forbidding that any institution or business require the vaccine. I hope more states do that. They have also put the kabash on vaccine passports.
Once you are “immune” to a virus, after you have had it or been successfully vaccinated, who ever said you wont get it again?
Do you think that creates a bubble where the virus cant enter your body or get going enough to produce a positive test result? It just means you skip the phase where your body has to over do the inflammation stage, to allow time for the antibody research phase to complete. Antibodies don’t kill the virus, they simply muzzle its connection capability to give your body time to create the killer cells which will clean it from your system.
Everyone’s immune system runs at a different rate and each day each person’s immune system ebbs and flows in strength based on sleep, hydration, nutrition etc.
Once 50-90% of people can have the virus in their system with little to no effect, little to no symptomatic effect, that is what herd immunity is. What a great CON we have witnessed.
Covid-19, a virus to which 99% of the world was already “immune” from the start, especially children.
The data is even worse for mutations.
The usual trend is for pathogens to get more contagious but less lethal. More infective mutants will drive out less infectious strains. More deadly strains OTOH run the risk of wiping out their hosts, ie victims. The more fatal European mutant that struck the eastern US may have succumbed in this manner.
Evolution 101.
Evolution 101, except when you give that more deadly strain a new evolutionary future by vaccinating with a ‘leaky’ vaccine.
https://www.pbs.org/newshour/science/tthis-chicken-vaccine-makes-virus-dangerous
Read this and understand.
I’m familiar with leaky vaccines and their risk of evolving more virulent strains. The only leaky human vaccine of which I know is for whooping cough, which is caused by a highly contagious bacterium. In that case, the pathogen doesn’t seem to have developed greater virulence. There could well be others about which I don’t know.
oh crap!
Bird flu isn’t alone. The world’s first vaccine for malaria, which was recently approved by European Medicines Agency, is also leaky. Vaccines for HPV and whooping cough can leak too; however it is unknown if this scenario creates more dangerous viruses for each of these diseases.
dunno why
I wouldnt bet my life that they DO!
European mutant?
What the freaking frack is that, body?
You suppose to be better than that, body!
You suppose to be smart, shall you not, John, the well versed John!
cheers
The strain that apparently arose in Germany, but hammered Lombardy early in the epizootic..
Since when a guy like you will consider strains as same as mutations?
John, please tell me that I am posing a wrong question
to you now!
cheers
John
New strains evolve via mutations.
I would have thought that that was obvious.
Yet more gibberish.
You really must be too young…
like a baby at the least, or very least,
isn’t it!
Learn to be patient, if you can, that is, if at the very least you can read this!
Can you really, read!
cheers
I think you would find your comments to be more effective if you weren’t so cryptic. You are getting a lot of down-votes, probably because a lot of bright people don’t understand what you are trying to communicate. The failure would seem to be on your end! Maybe if you come back when you are sober, you can make some contributions.
Clyde,
What makes you think that I, or even you or anyone else for that matter,
do ever engage in communication,
because simply the others have to listen or being subjected to our bright or otherwise thoughts?
In there and then, just like that,
is not much of a feedback!
Hopefully this not too messy or cryptic.
cheers
Your syntax is akin to a drunk. You can’t communicate at all. Your prose is also trash.
How in the hell do you not self-reflect on that?
Just a few weeks ago I heard someone say that the Chinese saw early case fatality rates of ~10%. That’s not what the U. S. has seen, where it seems to be much closer to 0.25% (I didn’t go look that one up, so anyone who did can correct me if they so choose.). Assuming either of those data points are correct, why? The Chinese did not even test for Wuhan Flu until the patient was already good and truly sick, so that they detected only 1 out of 400 actual cases of the virus? Or the U. S. test is so hyper-tuned that we’re seeing as much as 90% false-positive cases? If neither is the case, if those numbers are anywhere near correct, then what the Chinese faced is not the same thing as what the U. S. faced. Or is the actual number somewhere in the middle of all 3 of these reasons?
There were lots of “leaked” news reports and photos supposedly smuggled out of Wuhan about people dying in the streets, locked in apartment buildings, and bulldozed roadblocks out of the city. Disinformation?
That certainly would not be a factor for Chi-vi with ~0.5% fatality.
Even the 35% deadly MERS (thank goodness not very infectious) still comes back multiple years (45 cases in 2020). In my mind, I kind of joke that Arab tradition of kissing their prized camels keeps it going.
The probability of a mutation making an already deadly virus to be somehow more deadly is very small. The overwhelming outcome of any mutation is that it will be no more or less deadly per capita infected (even if it might happen to become more infectious).
John, Farr’s laws
William Farr
https://en.wikipedia.org/wiki/William_Farr
Law of epidemics[edit]
Main article: Farr’s laws
In 1840, Farr submitted a letter to the Annual Report of the Registrar General of Births, Deaths and Marriages in England. In that letter, he applied mathematics to the records of deaths during a recent smallpox epidemic, proposing that:
“If the latent cause of epidemics cannot be discovered, the mode in which it operates may be investigated. The laws of its action may be determined by observation, as well as the circumstances in which epidemics arise, or by which they may be controlled.”[10]
He showed that during the smallpox epidemic, a plot of the number of deaths per quarter followed a roughly bell-shaped or “normal curve”,[11][12] and that recent epidemics of other diseases had followed a similar pattern….[13]
No, the hype is worse, the data suggests otherwise.
During the Spanish Flu, SF had a resurgence after celebrating in the streets over success in fighting what turned out to be the first wave. In Oregon, they turn out in the streets to celebrate violence.
The Flu in San Francisco | American Experience | Official Site | PBS
A note to the author of this article.
No matter how you think about herd immunity towards covid,
even when in this point in time, a year after at least,
and you yourself at a positive stand now,
still you completely non immune to stupidity about of it all.
No much chance of any herd immunity there, towards the stupidity shown or exercised.
No much chance of receptive immunity of the herd there, to contemplate.
Really sorry, but that’s how sometimes it happens to be.
Nature, life, sometimes happens to be a real bitch… “”””” and squarely.
cheers
not
Give it a rest.
In your case you are lucky.
For best of me can’t make out your given “name” there.
Too hard for me… it makes me feel weally illitewate…
Thank you any way, for your time and effort.
cheers
For goodness sake,
stop laughing mikebawtnz.
🙃
cheers
Sober up
Still hammered, then? Maybe sober up a bit if you want to make a coherent reply.
Some cases, perhaps quite a significant number, are lab confirmed but not actually sick people. We are still testing some 15,000 per week who have no symptoms. If one ever expects to get to zero cases without considering the false positive rate — well that person is a fool. If a person hopes to control an epidemic with lab tests without considering false negatives, then person is a fool too. This epitomizes most of our public health folks.
hospitalization rates are a better indicator but unfortunately hard to get those stats
to clarify, if your goal is “keep hospitals from being overwhelmed” then hospitalization rates not new cases is what you should keep your eyes on
It’s a sad situation indeed. The link below says that hospitals are charging from $20 to $1419 per covid test. If labs are able to get someone to pay about $1400 for a test that probably costs less than $20 to perform, I can see why they would never want to stop providing that “service.”
https://www.healthsystemtracker.org/brief/covid-19-test-prices-and-payment-policy/
I live in Yuma, AZ – a small town with a agriculture/military-based economy. We also host a huge number of “snowbirds” for 5-6 months out of every year – and they have been leaving in droves in recent weeks as the warm summer temps are returning.
When these snowbirds first came down back in October/November, Yuma County showed up on the ‘covid hot-spot’ map, and the NYT wrote a wonderful hit piece on how Yuma County was surging with covid cases – an article designed to harm our economy as punishment for its overwhelming support for Trump (most winter produce for the country comes from here, and Imperial County, CA).
The vast majority of our snowbirds come from Washington, Oregon, and Canada (BC). They apparently brought the Covid surge with them when they came, and are apparently taking it back to the Pacific Northwest as they leave.
These ‘surges’ are not difficult to understand when you understand the ‘migration patterns’ of this select group of travelers – unless you are a “science” writer for the NYT….
Richard, I live in Arizona, too. There was a definite connection between COVID and the migration pattern of the Snowbirds. Farther north, we see a fair number from the upper Mid-western states. Florida seems to get their Snowbirds mostly from New England states. One would think some enterprising soul would have studied that pattern but no one has, as far as I know.
Yeah, but such a study might interfere with the narrative, so it would be escorted quietly out of the discussion 😉
Per CDC data 80% of the C-19 CASES were among those UNDER 65 years.
80% of DEATHS were among those OVER 65 years.
30% of C-19 DEATHS were among those OVER 85 years at 2% of the population.
30% of C-19 deaths occurred in nursing homes, hospice or residence.
The HERD was already immune. C-19 was just culling the HERD of the too many, too sick, too old, too crammed together in contagious badly run (BLUE) elder care facilities.
The lying, fact free, fake news MSM coup d’etat propaganda machine rebranded the annual influenza as C-19 to stampede the sheeple into foregoing due process and civil liberties and to depose Trump.
We now know how easy it would be to line the sheeple up for cattle car trips to zyklon showers.
Nick,
The lying, fact free, fake news MSM is also complicit along with their High Tech Nazi buddies for many of the fatalities that occurred! By suppressing information about ivermectin and HCQ, and cancelling anyone who tried to promote the use of therapeutics, they helped kill at least 200,000 Americans! That makes them mass murderers; just like the original Nazis they try so hard to emulate!
And we can’t let the CCP and the WHO off the hook either! The early coverups and lies from the ChiComs and their puppet lead to a great deal of misinformation and deaths as well!
Speaking of governments and tech giants, I just came across this recently. I was never for vaccine passports as a matter of civil liberties but this gives a chilling and even more important reason to oppose them.
I have been shocked to learn how many American companies aided the Nazis, some even after WWII started, like Coca-cola and IBM.
How IBM Helped The Nazis Carry Out The Holocaust
https://allthatsinteresting.com/ibm-nazis-ww2
This is accurate enough I want to up-vote it, but depressing enough (because it’s too close to true) that I won’t.
277 youngsters (0-17 years of age) have died of C-19 in the U.S. since the pandemic began. There are apparently about 22 million within this age group. Less than 1% of this group have been fully vaccinated but there have been about 10 deaths associated with the vaccines. At least one, a 2 year old, was part of the Pfizer trial.
I was not able to find the number of C-19 cases in this age group, but it appears that death rates from vaccination are on the same order of magnitude as death from C-19.
Without a doubt, there will be survivors of C-19 in this age group that will succumb to vaccination death. Throw in the unknowns of long-term effects and this drive for their vaccination borders on insanity.
Scopes is saying that the purported death of a 2 year old being part of a Pfizer clinical trial is “unproven.” I can’t imagine that a 2 year old would be part of a trial at this point. So, I would question this claim also.
Given that when Snopes says “unproven” it typically means they don’t agree with the story but didn’t look for any evidence one way or the other and that there are parents who are willing to have puberty blocking drugs given to their 9 year old because they (the kids) want to be a different “gender”, I would not be surprised at all that some paranoid parents would allow their 2 year old to be part of a trial for an experimental medication to possibly “save” them from a non-existent threat.
Community immunity implies reduced transmission paths, which mitigates but does not preclude exponential blooms.
Don’t be “naughty” now.
🙂
One factor that is greatly overlooked when discussing COVID is the change in the World Health Organization’s recommended number of cycles in their testing procedures, which decreased from 40 to 25 on January 20, 2021, which just happened to (probably intentionally) coincide with Joe Biden’s inauguration as president.
Each cycle concentrates the virus particles (or fragments thereof) by a factor of about 2, so that 40 cycles concentrates the particles by a factor of over a trillion (2^40 = 1.1*10^12) over the original swab. The newer 25-cycle tests base the diagnosis on a concentration of 2^15 = about 32,000 times lower than the earlier 40-cycle test.
This means that the 40-cycle (Trump era) tests were detecting lots of false positives (from virus fragments, not entire viruses) among asymptomatic people who needlessly quarantined themselves and never got infected. If the test detected fragments of the virus but they never got sick, these people were probably already naturally immune–they were exposed to the COVID virus (or a similar virus) but their bodies destroyed it.
With the 25-cycle (Biden era) tests eliminating most of the false positives, people who were exposed to the virus but never showed symptoms now test negative, but are equally naturally immune, but are not counted among those exposed to the virus, so that natural immunity might be higher than previously thought. Add to that the fact that children seem to be naturally immune, and the total immune fraction may be even closer to “herd immunity”.
Didn’t they also change the definition of a “case” to require TWO positive tests? I recall reading something about that.
There were people who applied the 40-cycle test to non-human materials (like orange juice) and got positive results.
Make sure to use a 6 foot long straw.
And an N-95 mask.
Steve Z makes an important point. It seems different health authorities can set the Cycle Threshold (Ct) as they see fit. The most current recommendation from the CDC is to set the Ct to less than or equal to 28. I’ve seen others recommend keeping Ct between 20 and 25. Comparing “case counts” between jurisdictions might not be valid unless the Ct (and other testing factors) are known.
Steve Z,
Zerohedge has a good article on that here.
Right On Cue For Biden, WHO Admits High-Cycle PCR Tests Produce COVID False Positives
Jan 21, 2021 –
https://bit.ly/3iL13lD
Also, these are interesting.
http://bit.ly/3uEt9o1
and, here.
COVID19 PCR Tests are Scientifically Meaningless Though the whole world relies on RT-PCR to “diagnose” Sars-Cov-2 infection, the science is clear: they are not fit for purpose
https://bit.ly/36vkZ7I
In the UK press HI theory has been described as “discredited”, a narrative designed to strengthen the case for locking down.
The Lancet in its zeal to be anti Trump published and then retracted a dodgy paper on Hydroxychloroquine
Getting good (unbiased) information is nigh on impossible – I’m willing to bet the UK has immunity now. Will they give up control?
Unlikely
Due to the EU being a dangerous neighbour and a bad actor, we’re having some difficulty getting a second dose of the vaccines. So, although we might have fair to middling immunity from the first dose it isn’t by any means certain that this will be enough to block this third wave that the EU seems to be experiencing. Let’s just hope that one dose is enough and that Ursula VDL isn’t trying to harm the population of the UK by her stupidity and incompetence.
On the data I have reviewed, one dose of either mRNA vax suffices. Not quite as good as the 1 dose Janssen viral vector.
Let me explain. Vax is intended both to prevent symptoms and lessen their severity. Neither mRNA vax are fully effective at preventing ‘breakthrough’ infections, unlike cowpox for smallpox.
So, compare one shot mRNA to Janssen adeno viral vector. One shot about the same at preventing any symptoms, and about the same at preventing hospitalizations. The two shot is admittedly better at preventing any symptoms, but that is a false 2x$ message.
Depending on where the report originated and which company they were shilling for, a single dose should give something like 65-80% protection. Hopefully that will be good enough.
Rud, pardon my ignorance but could you explain further. I’m 78 and am holding off getting jabbed. I live in a safe spot, very low risk and have been waiting for the powers that be to get their act together re vaccines. Presently 4 month wait for 2nd jab.Also hoping for new breakthroughs for vacs ie. novavax is one I think and a so called supervac that treats all variants by impacting a different ‘leg’ of the spike.
regards, doug
Probably a good thing. See Dr Been’s tedious video with a guy translating an Israeli report in Hebrew. Second dose + more serious side effects.