This letter from our local hospital ER doc has been circulating on social media in my town. It is applicable for anyone, anywhere, to read and heed. Note “the surge” section – Anthony
Dear Butte County and all the folks who may under the care of Enloe Medical Center,
I am one of your local Emergency Medicine docs at Enloe Medical Center. So I’d like to take a moment to explain Covid-19 and how and why it is impacting our community.
Specifically, I’d like to go through the basics of the illness and (as a consequence) what Enloe Hospital is doing to meet the coming crisis.The first thing I will mention is that the Covid-19 disaster is an extremely dynamic and changing situation.
Every day at the hospital we are meeting constantly and changing policies–directions from world, federal, and state programs change multiple times per day. This is an unheard of pace of change.Here are the basics about the Covid-19 illness. The virus is highly contagious. It is predicted that eventually, nearly everyone will be exposed and been infected.
A very few very lucky people may not develop any symptoms at all. The vast majority of people will get a mild syndrome of variable symptoms including “flu”–fevers, achy-ness, upper respiratory congestion (ie nose and throat symptoms). Then they will get over it. And probably wonder what the big fuss about it was. Younger children may have an even milder syndrome.
However, during the typical 7 days of mild disease and then another 7 days later, all infected patients will be spreading this virus. If you turn up to the Emergency Department with mild illness, you will be screened (important factors such as vital signs and your oxygen saturation percentage), and likely sent home with 2 important instructions: signs of worsening illness, and strict self-quarantining precautions.
However, if you are unlucky, after the initial mild syndrome, instead of getting better, you may get worse. You may develop worse “flu” symptoms and then pneumonia–filling of the lungs with infected fluid.
These are the patients that will be admitted to the hospital for general care and observation. Once again, the majority of these moderately ill patients will get better.
However, if you are very unlucky, over the next day or two, instead of getting better, some patients will turn for the worse and will develop a form of ARDS (Acute Respiratory Distress Syndrome) whereby the lungs will become completely saturated with fluid and will need to be placed on “life-support”, that is a mechanical ventilator. They will be transferred to the ICU (Intensive Care Unit) until their lungs can recover.
A large proportion of these patients will eventually recover, but some will not.There are some clear risk factors for ending up in the ICU. Older age and baseline medical illness (diabetes, chronic heart disease, chronic lung disease) make it much more likely to go on to ICU-requiring Covid-19 illness. However, even perfectly healthy adults can develop serious illness. Fortunately, younger children are almost entirely spared.The overall picture of this sort of illness is NOT new to the medical community. Most of what I have described above (mild/moderate/ICU levels of illness) can be applied to the Influenza virus, which we have been dealing with for years.
The concerning difference is the infectivity of the Covid-19 virus, and mathematics.Using some basic simplified statistics will yield math that is causing everyone in the hospital to enact drastic measures.
Enloe Medical Center covers roughly 300,000 people in Butte and surrounding counties. As I mentioned everyone will get Covid-19. If only 0.5% of patients who get Covid end up in the ICU, that will be 1,500 patients requiring an ICU. Prior to our Covid planning, Enloe had only 20 ICU beds. 1,500 patients will not safely squeeze into 20 beds. This, my friends, is the SURGE. This was what overwhelmed the hospital systems in China and Italy.
Make no mistake the surge is coming.
So pretty much everything we are doing- all this “social distancing”- is to even out this massive surge of patients and spread them out over time, as opposed to having all of them show up at our hospital at once.And the analysis of China and Italy has produced a clear message. The most effective strategy to mitigate the surge is strict quarantining. Not disease testing. Not experimental medications or specific treatments. Quarantining, social distancing, whatever it takes to slow (not stop, not cure) the spread of disease.
So take quarantining and social distancing seriously, because it will save lives.
And it may be hard to take seriously, because as I mentioned the vast majority of people will only get mild illness. And then they may ask themselves, why did I go through so much trouble, not being able to go to my favorite bar.
Even more seriously, the economy is heading downhill and many people are not getting paychecks. For a mild “flu”. Again, the answer is that all of the sacrifices are NOT for the mildly ill, but for the unlucky ICU bound. And that may be you or your loved one. Picture this:
Scenario One–your loved one is developing ICU level pneumonia. The team of doctors, nurses, and care-givers identify this, treat your loved one and move her to the ICU.
Scenario Two–your loved one is developing ICU level pneumonia. But there is no room in the ICU and she is put on a jury-rigged breathing contraption for life support in the hallway outside of the Emergency Department. Next to 60 other patients in the same situation.
And the message from China and Italy and other countries has been specific–the most effective strategy to avoid Scenario 2 is aggressive quarantining of the mildly ill and EVEN asymptomatic.Employing strong individual efforts to prevent contracting Covid-19 will slow the progression and buy time to smooth the ICU surge– and it may also buy time for doctors and scientists to develop and test treatments and vaccinations.Some common questions that I have been asked–Why can’t I be tested for Covid?
Every day, the hospital is attempting to obtain methods for rapid testing of Covid, but as you might imagine the supply of testing materials is a lot more rare and much more expensive than toilet paper.Another common question is: Does it seem that the hospital is over-reacting? The answer is “We hope so!”
And–don’t forget that hospital workers are at highest risk for exposure and spreading the illness. Which is why we are trying to be so meticulous about infection prevention–don’t be surprised if you end up in the Emergency Department, respiratory issues or other standard ER problems, staff are wearing gowns, masks, and greeting you from a distance. If a hospital worker starts to show symptoms of infection, this will remove him or her from a very limited working pool for a long period of time. And we need every hospital worker we have.
Another comment I would like to make: If you have an elderly family member or loved one with advanced illness, please take the time to appreciate them. And then discuss the possibility that they might develop severe Covid-19 illness. No decision at this time has to be final, but it is better to understand where everyone stands prior to the storm hitting.
Here is another question: When? This is a tricky one, because we do not locally have quick testing for Covid-19. The current wait time to get a test result back is over 1 week. Our first official Covid positive test in Butte County was on Saturday March 21. As of today (Mar 25) there are at least 4 documented positive cases in Butte County, though likely there are many more people who are infected but have not been tested, due to the shortage of testing kits and assays. So people in our community are right now progressing through the contagious but mild symptom stages. We anticipate pneumonia and ICU patients declaring themselves within the next few weeks.
Thank you for reading, and thank you for keeping Chico safer,
Ivan Liang

MD FACEP FACMT
https://www.enloe.org/find-a-doctor/find-a-doctor?id=232
New reported cases and deaths fell yesterday in the US. Most of the improvement in new deaths came in NY (down to 82 from 277 the day before). About a quarter of NY’s deaths came in nursing homes.
Day to day data for the US:
March 28: 19,452 new cases; 525 new deaths;
March 29: 18,469 new cases; 264 new deaths.
https://www.worldometers.info/coronavirus/country/us/
Drop in new cases despite increased testing.
Rates of increase are also falling in the UK.
Could be a one-time wonder blip. We’ll see.
But this says 237 deaths in NY Sunday:
https://news.yahoo.com/coronavirus-slowdown-seattle-suggests-restrictions-121913987.html
He forgot scenario 3
Scenario Three – Your loved one is developing ICU level pneumonia. The team of doctors, nurses, and care-givers identify this, treat your loved one and move her to a non ICU – quarantined hospital room with a ventilator and ICU level monitoring because stacking contagious patients in the hall outside Emergency is the surest way to infect the entire hospital
scenario 4…
They start passing out the two malaria drugs like after dinner mints…
….FDA just approved them and so did France
After this is ended, let’s hope they will have learnt something about the need for real, rapid response to real threats. People did it in WWII and we can still do it today when not shackled by bureaucracy. especially with a bit of relatively cheap foresight. No need to reverse the industrial revolution.
Hopefully, sea level rising at 1 to 3 mm per year really will be put in its proper perspective after this.
I would also question his statement about “unproven remedies”. 78/80 in the French study got better quickly with hydroxychloroquine and Azithromycin. That’s 97.5% folks.
As to the statement that testing doesn’t work South Korea would beg to differ.
Maybe he wasn’t aware of these things. I’m sure he is busy.
Been feeding the family tonic water for 10 days in hopes it helps knock the worst edges off it if we get it as we isolate as best possible
Hopefully, sea level rising at 1 to 3 mm per year really will be put in its proper perspective after this.
I doubt it. The “rising sea” scare-moniker is like a drug — they can’t give it up, no matter how ridiculous. Same w/the the sea-ice crap & polar bears.
We in the medical field call it “nosocomial” infection, infections caused by or inside hospitals. We also talk about “iatrogenic” infection, these caused by actions of doctors.
Winter is the coronavirus season. CVs are the second most usual causal agent of what we call the “common cold”. The most usual cause of common colds are rhinoviruses. There are dozens of each of these two types. This is why we can’t have vaccines for the “common cold”.
COVID-19 is a common cold virus. Very contagious, as are most of these (common cold viruses), but very mild compared with influenza viruses, in general. You can tell because these coronas spare children and infants (Thankfully!) who are in danger from flu, because flu gives very high fevers which babies cannot thermoregulate, and these may perish in the early going.
Why the panic, if what I say is true? Because, this is the first time in history that we can 1) identify COVID-19 AND 2) Test for it, AND 3) track it globally. We were able to do these things a little bit beginning with SARS in 2002, then MERS in 2012, but we did not have full global participation then, nor the high capacity for testing.
Note that there are about 9-10 years between corona outbreaks, possibly because of some residual immunity among the subtypes in successive generations. Children below 10, therefore, get it, have normal colds from it, then become effective carriers to the elderly.
In coming years, we will have developed quite a lucrative industry in virology. I predict the next “killer” will be a rhinovirus (head cold). It will have a name.
All viruses are killers in managed health care facilities where elderly are warehoused.
The figures are live as reported, on weekends you need to take care they don’t reconcile them until Monday. I noticed it having watched the data for 3 weeks now
The numbers ended up
March 29: 19913 new cases and 363 new deaths
March 30: 20353 new cases and 573 new deaths
Those numbers are meaningless absent the important “total persons tested” metric. 20,000 “new cases”. If you have tested 25,000 people, it’s a catastrophe; if you’ve tested 250,000 people, it’s a concern; if you’ve tested 2.5 million people, it’s less than 1%.
ONLY http://www.cdc.gov has trustworthy numbers.
The article is hysterical nonsense.
The misleading “test” actually tests for ANY “corona virus”, of which there are 19.
And even that is missing the real point.
recommended:
Corona: The Case Number Game:
https://www.lewrockwell.com/2020/03/jon-rappoport/corona-the-case-number-game/
Were did you get the idea that there are 19 corona viruses?
MarkW
Obviously one novel virus per year since the turn of the century! /sarc
Try its name. Co for corona. V for virus. ID. 19
Umm, it’s named for the year it appeared, not the number of species.
COVID-19 is the name of the disease, not the virus.
The CDC recognizes seven species of human coronavirus, counting Wuhan as separate from the SARS virion:
https://www.cdc.gov/coronavirus/types.html
Human Coronavirus Types
Coronaviruses are named for the crown-like spikes on their surface. There are four main sub-groupings of coronaviruses, known as alpha, beta, gamma, and delta.
Human coronaviruses were first identified in the mid-1960s. The seven coronaviruses that can infect people are:
Common human coronaviruses
229E (alpha coronavirus)
NL63 (alpha coronavirus)
OC43 (beta coronavirus)
HKU1 (beta coronavirus)
Other human coronaviruses
MERS-CoV (the beta coronavirus that causes Middle East Respiratory Syndrome, or MERS)
SARS-CoV (the beta coronavirus that causes severe acute respiratory syndrome, or SARS)
SARS-CoV-2 (the novel coronavirus that causes coronavirus disease 2019, or COVID-19)
People around the world commonly get infected with human coronaviruses 229E, NL63, OC43, and HKU1.
Sometimes coronaviruses that infect animals can evolve and make people sick and become a new human coronavirus. Three recent examples of this are 2019-nCoV, SARS-CoV, and MERS-CoV.
Name origin:
CO(rona) VI(rus) D(isease)-(20)19.
Ummm …
It’s named covid 19 because it was discovered in 2019
’19’ Comes from 2019, the first year the virus showed itself: “2019 novel coronavirus”
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it
Richard,
Apparently I misspelled “ummm”…
>> Try its name. Co for corona. V for virus. ID. 19
Now that was funny
Wrong bc57 Co for corona, Vi for virus, D for disease, 19 for 2019.
“Coronavirus” is a family of viruses, of which the virus responsible for COVID19 is only one.
We don’t know how many. I believe CDC has 7 genotyped so far. Very common type of virus (see my other post). Should be hundreds in history, since viruses are known to easily recombined with other RNA to produce a new coating of protein. They don’t “mutate” or “evolve” per se, rather they recombine with pieces of other RNA.
Virus most certainly do mutate and evolve. Many rapidly. Thank God, the WuFlu virus mutates more slowly than most RNA viruses.
But in Iceland alone, 44 mutations have already been detected.
Viruses do indeed combine with others in horizontal transfer of genetic material, ie nucleic acid sequences, but they also mutate and evolve with reckless abandon.
Fundamentalism and creationism k!ll.
I cannot agree that the article is “hysterical nonsense. A lot is made of statistics for “ordinary” flu, but WuFlu has to spread through the population before it can become an “ordinary” flu. Until that has happened, its infection profile is very different to “ordinary” flu. The efforts being made to slow its spread are aimed squarely at preventing it from swamping the hospital system: “all this “social distancing”- is to even out this massive surge of patients and spread them out over time, as opposed to having all of them show up at our hospital at once“. Once that has been achieved, WuFlu can join the family of “ordinary” flus, with a more regular annual incidence modified by a partially successful vaccine. Until that has been achieved, “social distancing” makes a lot of sense.
I do think that the US approach to WuFlu is better than a total shutdown, because it is aimed at having the virus spread at a rate that the hospital system can cope with, rather than trying to prevent its spread altogether. Countries that do the latter risk having the virus re-emerge in an unexposed population and hence putting everyone through the whole thing all over again.
Without a proper antibody test for WuFlu it is impossible to tell where the virus has been. As it is apparently quite infectious, it would move through the population quite quickly. But, we did not really start testing for it until sometime in late February.
In the Wheeling, WV area, many of us are convinced that this virus moved through here in late January, early February, which is when some of us were very ill with all of the listed symptoms. This last month hardly anyone has fallen ill. We have been there and done that.
Only an antibody test will allow us to properly apply epidemiological methods.
So, far we have very radical and over-hyped predictions of deaths from WuFlu, while the actual numbers do not make sense. Why would whole parts of the country seem to not be getting this virus thus far when it is so infectious? Perhaps because it has already passed through earlier in the year. Instead, we have wanton predictions that these areas are going to be ravaged. It makes no sense considering how fast the virus moved around the world and the many people moving between states constantly. Again, the numbers do not add up.
I believe the belief that Corona is “quite infectious” is fake news. Health organizations say it is less contagious than the regular flu.
Which health organizations would that be?
What doesn’t make sense is why you think a virus should affect all parts of a country the size of the US uniformly. Why do you think this?
I think the article is wrong. Many victims need air and ventilation to get them through. Number of days on ventilation for many is 10 days or more. This means entire hospitals are being clogged up with patients filling wards, corridors. The amount of resources needed to look after this many patients is a logistical nightmare. Add the strain on doctors, nurses and support staff. All doing this within an highly infectious environment. It is closing down the health care system.
On a positive, US deaths have remains stable. Self distancing and isolation kicking in, US doctors are using different techniques and treatments or a mixture of both.
I’m no expert nor very knowledgeable on these fields -perhaps that let’s me see Reality in a different and perhaps less biased way?
If what you assert here were the case, the data from an actually closed case, the Diamond Princess cruise, would show much worse numbers. However, zero point five percent fatality ratio, and that being a population prominently of elderly people (stranded and abandoned and being the first live guinea pig of this virus-phobia event watched by the world, but from a distance -with the ensuing trauma, which kills as a virus or perhaps more). That alone tells me a way different story, and also tells me (again, no ‘expert’) that this is no’ new virus’ at all.
What am I missing?
Also, the cases of:
-Taiwan (next to China, great mingling of people for long time until they closed borders, going on since, allegedly, October? November? when the proverbial patient zero should have been already roaming lose)
-Liechtenstein (no “social distancing” orwellian nonsense; no lockdown; no deaths)
-Sweden (no “social distancing” orwellian nonsense; no lockdown; almost no deaths)
Do you know what they all have in common? they all do NOT implement WHO’s totalitarian policies so far. Isn’t it quite the politicized virus? I have a different view on the body-mind-environment though, and I work with it; it’s not just theoretical. And it too comes from Science (see Polyvagal Theory, Stephen Porges).
Furthermore, Gibraltar, with a grand total of ZERO deaths, IS LITERALLY IN SPAIN, which reports up to 10000 deaths and keeps ramping up mass-panic daily for three weeks now, opening the news reports with the fucking number as if that was all there is to it. In here, mainstream media lies and pushes fake-news every single day, it’s crazy. What about this in your country btw? Anyway, high ‘co-mingling’ between Gibraltar and Spain too; so, what is that about?
Ths virus does behave as a highly politicized one to be honest.
Do you see anything wrong here btw? or it’s just me?:
https://health.hawaii.gov/vitalrecords/guidance-for-certifying-covid-19-deaths/
I’m asking honestly.
Wally
Well, you live up to your name OK.
This has nothing to do with numbers reaching pandemic proportions, it’s about stopping it doing so.
It’s the speed at which it propagates, and the ease with which it does so. It may not even be as deadly as flu, but it makes up for that by ruthlessly killing people who show the least weakness.
And whilst the west has sophisticated technology, we have neither prevention nor cure. And our fatal weakness is not even that, it’s the facilities and personnel available to care for the sick. We simply don’t have the beds, nor the ventilators to deal with the number of sick demanding Intensive treatment.
And as the numbers of cases rise, the number of medical staff falls as they succumb to the virus.
I suspect the real threat of this virus is not it’s ability to kill people, but the speed at which it seeks out potential victims. Ripping through our youth virtually undetected, who carry it to adults, undetected.
Maybe we should call it the Xi Flu instead of WuFlu, if it specifically attacks those that show any weakness.
Seems more apt, he goes for the jugular without fail
Six species of coronavirus are known to infect humans, some of which have more than one strain. The number afflicting other mammals and birds is untold.
CoViD19 stands for Corona Virus Type ‘D’ 2019. Not the 19th Corona Virus.
COVID-19 actually is the name of the disease, not the virus which causes it. The virus which causes the disease is labelled SARS-CoV2, which for short, I call Wuhan virus.
If each bird and mammal species suffers from as many coronaviruses as humans, then there are on the order of 100,000 of them.
Anyone who thinks this “is hysterical nonsense” go down thread and read:
Rud Istvan March 30, 2020 at 12:18 pm
LET’S HAVE SOME PERSPECTIVE:
https://www.livescience.com/56598-deadliest-viruses-on-earth.html perspective
We have doomsday prep group like Mosher on one side, and it isn’t happening and why I am in locked group on other side … there is no perspective it’s just fun to watch.
Probably best to wait before considering any of those as a trend, especially given Italy’s experience.
At about 20 mins he talks about Italy; basically the perfect storm. Also the 40 doctors who died
appear top be taken from an obit page of a medical magazine; includes 90 year olds; not those in hospitals.
Perspectives on the Pandemic: Dealing with Coronavirus, a fiasco in the making? As the coronavirus pandemic takes hold, we are making decisions without reliable data. Dr John P.A. Ioannidis is a professor of medicine and professor of epidemiology and population health, as well as professor by courtesy of biomedical data science at Stanford University School of Medicine, professor by courtesy of statistics at Stanford University School of Humanities and Sciences, and co-director of the Meta-Research Innovation Center at Stanford (METRICS) at Stanford University. See his thoughts in writing here: https://www.statnews.com/2020/03/17/a…
https://www.youtube.com/watch?v=d6MZy-2fcBw
Prof. Dr. med. Sucharit Bhakdi, Facharzt für Mikrobiologie und Infektionsepidemiolgie, leitete 22 Jahre das Institut für Medizinische Mikrobiologie und Hygiene der Universität Mainz. Er hat einen offenen Brief an die Bundeskanzlerin geschrieben mit 5 Fragen, die nach sofortigen Antworten verlangen, um festzustellen, wie begründet die derzeitigen massiven Einschränkungen unserer Grundrechte sind. Das Video erläutert die Fragen und deren Hintergrund. Der ganze Brief im Wortlaut mit den Fragen, Hintergründen und Referenzen kann hier eingesehen werden: https://docdro.id/23IE5dj
Good German compound word:
Panikreaktion!
Italy, for whatever reason, is believed by the NIH to have over reported virus caused death by a factor of about 8x.
The Italian National Institute of Health stated that themselves. 88% of deaths were not caused by coronavirus, though death certificate said they were.
The old “death from” and “death with” difference.
My italian friends say they is a financial incentive for claiming corona deaths. Not sure of the details.
CV19 in a lot of cases becomes an “accelerator” for those with one or more late stage co-morbitities. To me that term makes a lot of sense.
hunter
What about publishing a reliable source for this claim?
J.-P. D.
https://www.telegraph.co.uk/global-health/science-and-disease/have-many-coronavirus-patients-died-italy/
https://www.fort-russ.com/2020/03/italy-only-12-of-covid19-deaths-actually-list-covid19-as-cause/
icisil, RK
https://www.epicentro.iss.it/coronavirus/bollettino/Report-COVID-2019_20_marzo_eng.pdf
Thank you, I will read the stuff, sure it is correct!
J.-P. D.
Italy has:
a poor healthcare system, 7 ICU beds per 100,000,
the 2nd oldest population in the world,
many smokers,
highly social people,
and 300,000 Chinese moved to the Milan area from the Wuhan area in the last decade and who commute regularly from Wuhan (I think 3 flights a day).
So, do I wonder why they got hit fast by the virus? Also, the woke Milan politicians, when the virus scare began, tried to smooth over people avoiding Chinese by starting a “Hug-a-Chinese” campaign. How stupid can you get?
The area afflicted in Italy the worse has some of the highest air pollution in the world, the same was true for China.
The Lombardy region also has the worst air pollution in Europe. The other hotspots, Wuhan, China and Qom, Iran do, have bad air pollution too.
Lesson one to learn from this. When a flu kicks of in another country, stop all flights from that country.
UK update : http://www.vukcevic.co.uk/UK-COVID-19.htm
The divergence from the exponential trend line is still encouraging.
The high and getting higher mortality for cases vs. deaths is still puzzling, however. The U.S. is not showing this, i.e. its ratio of cases to deaths is approximately constant and much lower than that of the U.K.
UK tests only hospitalised patients, although total number of infected is judged to be about 10 x greater. The data shows hospital cases mortality while true overall mortality is assumed to be an order of magnitude smaller i.e. around 0.5%
“although total number of infected is judged to be about 10 x greater”
tal number of infected is guest to be about 10 x greater
As case load increases exponentially, what would you expect to happen to the amount and quality and effectiveness of care received by each patient ?
My guess would be exponential decrease.
Vuk
Those are very good and clear charts. Let us hope this apparent levelling off in deaths continues.
Have you got a similar one for France and Italy and Spain superimposed over the UK?
Tonyb
Hi Tony, I do hope too.
No, I’ve only done the UK’s data
France, cases scaled and lagged 13 days to align with fatalities.
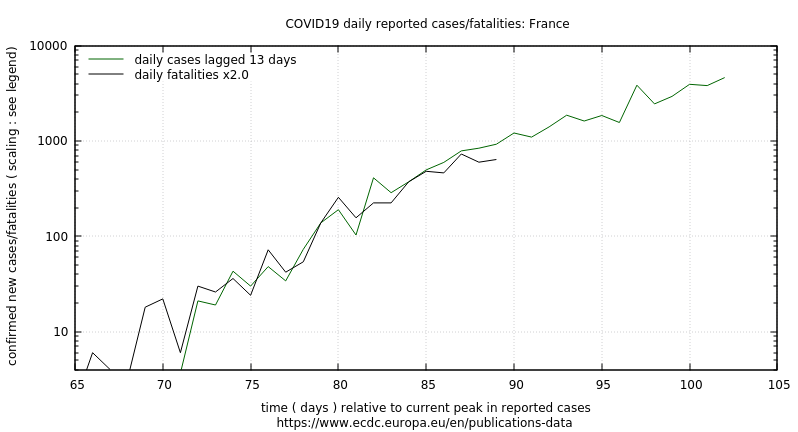
Not sure overlay is very clear. Note each is time shifted to align current peaks.

A similar plot for Italy shows a lag of 5 days and a scaling of 6x.
( previous french graph has incorrect x label: it’s days since Jan 1st )
Since testing availability and policy varies greatly and attribution of “COVID” deaths is defined differently, it is anyone’s guess as to what all this means. Caveat Emptor.
Italy seems to have peaked in new cases about 8 days ago though drop off is very slow at this point.
John Tillman
March 30, 2020 at 9:28 am
(…)
Rates of increase are also falling in the UK.
Here is my plot of deaths up to yesterday (29 March 2020).
New cases have fallen for three days and deaths for one. With under six hours to go today in the UK, cases are up slightly but deaths down again. We’ll see how the day ends.
that is because in the UK the whole country is locked at home, in the US your first amendment and your stupid adherence to its importance will mean many many deaths, I cannot believe that sane intelligent people are trying to second guess facts, just because it goes against what they believe is an inalienable right, people here are showing that they are just as bad as climate alarmists, they ignore the facts because the facts don’t agree with their beliefs. I also note that more people are going to be more sceptical of models from now on. which is a good thing for the climate argument in the future…if there is one.
https://www.worldometers.info/coronavirus/country/uk/
That’s where I got the data for my graph.
The drop in covid cases is due to stopping the spreading of the virus by isolation.
The covid cases will, if we keep isolating, drop to some low number.
How low that number is, will depend on, how effective and long we can keep isolated.
A vaccine I heard was a year away.
I do not believe China has zero internally generated cases.
Anyway, what appears to be good news about covid.
This is more on the anti-malaria medicine hydroxychloroquine which we discussed at here, and Roy Spencer found other evidence, that supports the assertion that it is effective against flu like illness.
A doctor from New York, Dr. Zelenko, appears to have somehow found a breakthrough treatment for Covid-19.
He said he has had (600 patients)
“…100 percent success using a cocktail of drugs: hydroxychloroquine, in combination with azithromycin (Z-Pak), an antibiotic to treat secondary infections, and zinc sulfate. Dr. Zelenko said he saw the symptom of shortness of breath resolved within four to six hours after treatment.”
This is his interview/discussion with Rudy Giuliani.
Apparently, Rudy talked to Trump…
… and now there is a pharmaceutical company that has donated 30 million doses of hydroxychloroquine to the US for emergency distribution.
https://www.youtube.com/watch?v=1TJdjhd_XG8
https://techstartups.com/2020/03/28/dr-vladimir-zelenko-now-treated-699-coronavirus-patients-100-success-using-hydroxychloroquine-sulfate-zinc-z-pak-update/
I did listen to ceo of Regeneron saying that he thinks in 6 months his “magical mice” will produce antibodies for the disease. Very interesting stuff
https://www.c-span.org/video/?470726-103/washington-journal-dr-leonard-schleifer-discusses-developing-covid-19-drug-therapies
Been there, done that. 4-6 months for initial viable antibodies is SOP. But then they have to be Humanized (remove murine bits of the ‘Y’ and add human bits so the immune system doesn’t attack them. Then you have to spool them up in a cho cell bioreactor making the ‘monoclonal antibodies’, and then do clinical testing. Developing a biologic drug is a long haul and very expensive proposition. Lets hope the simple generic drug combo works.
Might not be the best way to go.
Quicker, if possible, to inactive Wuhan’s RNA, then blow the envelope and spikes into people’s noses, so that our immune systems can make antibodies against a harmless virion.
The hard part is figuring out how to render the RNA impotent while leaving enough of the shell to generate antibodies. Could happen sooner rather than later. Or, lamentably, later.
Methods exist for inactivating viral RNA and DNA while still leaving immunogenic envelope proteins and sugars intact:
Psoralen Inactivation of Viruses: A Process for the Safe Manipulation of Viral Antigen and Nucleic Acid
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4664985/
I hope that a vaccine won’t take a year, but in any case, the WuFlu virus appears not to mutate rapidly, so a vaccine could be effective.
Or, better yet, no need to inactivate RNA, but just inject or grow in people’s own cells antibody-generating viral envelope protein, as for instance WuFlu virion’s spike:
https://theconversation.com/labs-are-experimenting-with-new-but-unproven-methods-to-create-a-coronavirus-vaccine-fast-134319
Here’s the link to John Hopkins world map of covid-109. Click on countries randomly to see their confirmed versus deaths versus recovered. Recovered usually under 1% and sometimes 0.
Now click Bahrain. 499 confirmed, 272 recovered? WTF!
They’ve been prescribing chloroquine and hydroxylchloroquine routinely since end of February. according to a few articles I came across. (sorry, I was surfing on another computer, links not handy).
How much more evidence do we need? Normal double blind tests take months to roll out . We don’t have months. For every patient that recovers quickly , there’s one less ventilator required . There’s more than one way to flatten the curve…
The John Hopkins Virus Map is very misleading as it does not give any current data, more or less all accumulated data. And, then, of course, the incoming data is bad. How does California have 6300 cases (which means test positives and not illnesses, or does it, we don’t know), 233, deaths, and 6 recoveries? That makes no sense.
Why do they never mention how many people proved negative? These people might already be immune from exposure earlier in the year.
ALL the compiled information has the same problem. There are no standards for reporting, there are no standards for testing, no one publishes their methodologies with enough detail that a statistician could figure out how to normalize it. Heck, how do you even compare countries when they didn’t even start getting infected at the same time, and they took completely different steps around social distancing and quarantine and border closings… there is no way to get accurate numbers. Worse than climate data by far.
But I still find it interesting that Bahrain has such a high recovery rate, unlike any of their immediate neighbours whom one would think would be similar.
davidmhoffer
+ lots and lots.
Thanks indeed!
But –
“Worse than climate data by far.” – now, that is going the extra mile.
As bad as climate ‘data’?
Well, we’ve seen some – ahem – seriously shoddy, unscientific numbers [not ‘data’], never mind the job-preserving interpretations, so – maybe.
Auto
John Tillman
To say “Rates of increase are also falling in the UK.” is misleading. There are encouraging signs, but there is a lull between people initially contracting the virus, and the establishment of social distancing measures & self isolation, where it’s incubating in many people as we speak.
There will be a surge, that’s why Nightingale units are being established across the country by military personnel.
M*A*S*H is alive and well.
Being prepared is good, better late than never.
However rate on increase in cases and deaths is slowing:
So far today in UK:
Cases 22,141 New +2,619 Deaths 1,408 New +180
Yesterday:
Cases 19,522 New +2,433 Deaths 1,228 New +209
Case increases at least partly due to more testing.
Too soon to call a trend, of course, and we’ll see where today ends up in three and a half hours.
Numbers far too noisy to look at rate of change of rate of change on a daily basis.
You need to do a log plot and fit a linear to log over at least 7 days. log(2)/slope give the doubling time.
There was a change in slope in France but it occurred about 2 or 3 days BEFORE movement restrictions, not five days later as one would expect after median incubation period. Any change after 5d is slightly increasing. Not much indication of the shut down showing any detectable change in the stats.
Maybe Sweden has got the right idea.
Too few data to do a meaningful statistical analysis. Thus, day to day “data” are essentially as meaningful as weekly figures.
So in your version of statistics 2 data points are as good a 8. Where can I learn more about fascinating new field of study? It sounds really powerful.
You and everyone else in the thread need a class in statistics.
Absent “total number tested”, “new cases” means nothing. If you tested 100,000 people day 1, and 110,000 people day 2, then the infection rate actually fell. Why is this fundamental point so difficult for so many to grasp?
Another basic statistical assumption is *the sample is random*. Here, in Ontario anyway, it most definitely is NOT. Only people who manifest some of the symptoms get tested, which means the sample is *skewed towards containing already infected people*. So simply counting “new cases” is bound to overstate the case.
Even with both of those provisos, I’ve run the numbers in Ontario, and from Mar 22-29, the ratio of infected:negative tests has hovered around 4.0%. The total cumulative has been slowly rising to 3.3% If the virus were *increasing*, we’d expect to see that ratio rise rapidly. However, as the number of tests perform each day has risen, we’ve seen the sample ratio converge to the cumulative ratio, and on the last day, when 10,000 of the 50,000 tests were reported, the sample ratio was 3.4%, compared to the overall 3.3%.
Unfortunately, Ontario changed its reporting method on the 30th of March, so it will be a week before I can trend the new format. But if I had to bet, I’d say between 2.5-3.0% of the total population is infected, and if we believe that 80% of those experience no to mild symptoms, we down to .24% of the population who will get some degree of severe sickness, and even then – currently with no proven treatment – 80% recover without going on a respirator. So, now we’re down to .048%, which 1/10th the doctor’s .5%, who end up on an ventilator. That’s 120 cases, spread over some time, vs the 1200 he expects. Again, if I had to bet, I bet that fewer than 200 cases in this county require ventilators when this is all over. We’ll see in a few months.
Testing for Covid-19 is meaningless as the test has never been verified to actually identify this particular virus. The CDC released the test without checking it first. None of the other cobbled up tests have been verified either.
Also, as the flu season is a salad of “flu” viruses (flu and coronaviruses), a person very likely might have more than one or several viruses at a time. The only thing the test indicates is that Covid-19 is present, but it does NOT finger the virus as what is making the patient ill. For all intents and purposes, Covid-19 might be an innocent bystander while another virus does the dirty work.
Covid-19 is indeed very infectious but that does not indicate its virulence. There seems to be an inverse relationship between infectious and virulence. This would explain why we see so many positive tests from asymptomatic people. At the very worst, Covid-19 is 1/10th to 1/100th the virulence of the flu.
It was updated overnight. They are now reporting 19,913 for the 29th. Still, over the last week the rate of increase has been going down. Nationally the doubling time of the disease has increased from about 1.7 days, to almost 4 days. An increase in this measure is good, because it means the rate of acceleration is slowing. We ain’t out of the woods yet, but this is the first clear sign that things are just beginning to slow down. (Nothing is for sure of course, something could happen to make the rate of spread start increasing again, but this is still a good sign)
The daily death rate in the U.K. seems to have reached a plateau (I say seems to because it is only 4 days of plateau and this isn’t long enough to draw any definite conclusions). If we have seen death rates reach their maximum this would mean the U.K. is fairly typical of Europe, while Italy and Spain are outliers. The average daily death rate in the U.K. is roughly 200, and our population is pretty much 20% that of the U.S. so you could expect the death rate to peak at aprox. 1,000 people a day. If the peak lasts for 2-3 weeks then the death toll would be aprox. 25,000 plus maybe as many again dying before or after the peak so I make a very rough estimate of 50,000 deaths for the U.S. Donald Trump said today that 200,000 deaths would be a positive outcome, for once I think that even he is being pessimistic.
Apparently not.. https://www.arcgis.com/apps/opsdashboard/index.html#/f94c3c90da5b4e9f9a0b19484dd4bb14
IT’S A SCAM.
http://gold-silver.us/forum/showthread.php?102096-Heroic-Citizens-Fact-Check-the-LYING-MSM-about-Corona
Heroic Citizens Fact-Check the LYING MSM about Corona
Yep we mounted a coup, trapped you all inside and took over the country and now you can’t even organize mass protest 🙂
Is Ivan Liang, MD FACEP FACMT, familiar with the efficacy of Prof. Didier Raoult and his team’s treatment regimen?
https://www.mediterranee-infection.com/wp-content/uploads/2020/03/COVID-IHU-2-1.pdf
I was shocked by the statement “If you turn up to the Emergency Department with mild illness, you will be screened (important factors such as vital signs and your oxygen saturation percentage), and likely sent home with 2 important instructions: signs of worsening illness, and strict self-quarantining precautions.”
Not even a mention of Aspirin, Vitamin C, or hydroxychloroquine.
re: “Not even a mention of Aspirin, Vitamin C, or hydroxychloroquine.”
Did you perhaps mis-understand? They are (probably) looking for Covid-19 positive patients only (and they do test). IOW do not show up to ER with only stomach ache or the sniffles. I do not recall w/o reviewing that long document where that statement is made …
They may be “looking for Covid-19 positive patients”. Medicine should not be about looking, it should be about treatment. This letter mentions only one treatment, a ventilator.
Might be worth considering this as a second opinion… https://forbetterscience.com/2020/03/26/chloroquine-genius-didier-raoult-to-save-the-world-from-covid-19/
T
re: “Might be worth considering this as a second opinion…”
Did you do you homework to see that that looks to be the earlier study (day late – dollar short)? Are you aware this is a dynamic situation with clinical (treatment) work ongoing even now?
The new study is 80 individuals? Are you aware also this is not an individual effort by Raoult? Have you looked at the list of co-authors and their affiliations? No?
Summary: You are behind the curve … recommend “get up to speed.”
Jim, the point is that the study would have shown that something very different had not six patients in the treated group been removed from the study because they died, or were transferred to ICU or stopped treatment because they could not tolerate the drug. This may just be the way the French do science today, but it is possible this drug did more harm than good.
Hydroxychloroquine for COVID-19: What’s the Evidence?
F. Perry Wilson, MD, MSCE
https://www.medscape.com/viewarticle/927342
Exactly. Poorly done study (nasal swabs have been shown to give false negative results >60% of the time) on only a few pts.
Along the lines of the classic–“In the experiment, 3 dogs got better…The 4th dog ran away.”
Plaquenil has been around a long time. It affects Plasmodium metabolism in a way unrelated to it’s anti-inflammatory effect in humans. It is not innocuous, having fairly high rates of serious retinal, cardiac & neurological side effects….It may or may not actually be efficacious, but is dangerous enough to deserve more serious study before it’s shot-gunned out on a desperate public.
The “study” alluded to in “Forbetterscience” involves a very unscientific “cocktail.” It reminds me of Moe calling for more Annakannapannistan to be poured into the rubber boot. I’m just surprised he didn’t add Echinacea dust also.
_Jim
You unfortunately do not know very much about what you are presenting here.
No valuable study of Raoult’s trial (hydroxychloroquine + azithromycin) has ever been presented. No double-blind tests.
Nonetheless, the French government decided to allow tests in a wider range. This can turn into a big problem for the politicians having taken the decision.
What, do you think, will Raoult tell you if his ‘cure’ gets off control?
He will tell you: ‘I never told that it would be free of danger’.
And that is the major problem, especially in the US where whole lawyer regiments wait for such an opportunity.
It is not enough to drive an 80-person test when introducing such an unknown medical combination for a huge amount of patients.
You need much more security.
This is exactly the reason why you yourself might one day be hiring a law firm if the medication is causing you chaos instead of healing.
J.-P. Dehottay
re: “You unfortunately do not know very much about what you are presenting here.
No valuable study of Raoult’s trial (hydroxychloroquine + azithromycin) has ever been presented. No double-blind tests.”
Idiot. People’s LIVES are at stake here – this isn’t some ABSTRACT statistical exercise done for your intellectual benefit!!! This isn’t an improved acne skin cream being tested for efficacy!! MAYBE you would like to perform Tuskegee Experiment again and _not_ treat those afflicted JUST to satisfy your cold, morbid ‘sciency’ appetite for ‘data’?
Must you be FORCE FED this info, and background surrounding these events, apparently yes, because you cannot figure them out yourself! HERE IS a Twitter dispatch from Dr. Raoult a couple days ago in reference to this study (he desires to show compassion for those suffering Covid-19 that might possibly die w/o treatment):
March 28 Update: In a Twitter post day, Prof. Raoult said: “Our study concerns 80 patients, without a control group because we offer our protocol to all patients with no contraindication. This is what the Hippocratic Oath that we have taken dictates to us.”
Side question: If you present symptoms, will you volunteer for ‘control’ group OR do you want to be treated? HAVE you ever had pneumonia before? Would you like to die that way?
“Idiot.”
Thank you very much for your insult.
And it is typical for people like you to feel the need for teaching others.
You did not understand even a bit of what I tried to explain…
J.-P. D.
Not that you don’t feel the need to teach others, usually in the typical German manner to show and express that only you know all much better than the rest of the world.
It’s mortifying, and you know it.
You are an idiot.
Let me answer for him. I am a retired doctor. I have experienced acute asthma, acute laryngospasm and whooping cough.If admitted to hospital with difficulty in breathing secondary to COVID 19 pneumonia, I would request admission to a double blind controlled clinical trial of active drug versus placebo, because this is the only way we will find the answer when dealing with a disease with a spontaneous recovery rate somewhere between 0.5% and 10%. I hope that’s clear enough for you.
re: “If admitted to hospital with difficulty in breathing secondary to COVID 19 pneumonia, I would request admission to a double blind controlled clinical trial of active drug versus placebo, because this is the only way …”
No, I don’t believe you. You say this now, without the element of ‘passion’ (emotions) being involved in the picture for decision-making. No one wants to die, or face death.
Not for your wife or mother either, IF a treatment is KNOWN by you to be available, because we ARE at that stage. To admit otherwise is, stupidity. Yes, on your part. Well, either stupidity, or you are NOT as well informed on this as you THINK you are. GO READ the continuing work in this area. To do otherwise, is, stupid, or resource challenged (IOW, you do not know where to ‘look’, yes, ‘physician’. Logic and common sense would not seem to be your strong suit.)
https://www.sciencedirect.com/journal/international-journal-of-antimicrobial-agents/special-issue/10V3JMBH9GZ
Notice the results here, ‘physician’, for daily hydroxychloroquine and azithromycine results in France:
https://www.mediterranee-infection.com/covid-19/
re: “If admitted to hospital with … I would request admission to a double blind controlled clinical trial of active drug versus placebo …”
John Cherry, let me say this to you: Your words sound as hollow as is your head (on this) WHEN we have on-the-ground experience as the following from such as Dr. William Grace, at Lenox Hill Hospital in New York City:
“Everybody’s using it [chloroquine] now off-label. We have a surge of coronavirus-19 patients throughout the metropolitan area of New York. And the problem is these patients are coming in quite sick. And when they get to a very difficult respiratory status, doctors are using hydroxychloroquine [an “analog” of chloroquine] with or without a drug called Zithromax or azithromycin. And that’s showing tremendous activity, and we have not had a death in our hospital.
We have probably close to 100 patients and not had any deaths. But I’ve talked to my colleagues at other hospitals in New York, and they are using hydroxychloroquine although the supplies are running down. So any kind of supplements to those supplies would be much appreciated…. In the trenches, we’re all using it especially for desperately ill people…. We’re not using it on everybody, but we’re using it on those people who show major respiratory compromise…
We think it works in two ways. As you know, the death rate goes up as the age goes up. And what I think is that the more mature your immune response, the more likely you are to have what we call a cytokine storm, which means that people with viral pneumonia die because their lungs fill up with fluids largely from an immune response. And this drug works not only inhibiting virus replication but also inhibits the immune response.”
Video of interview: https://youtu.be/sPRuCqINYh0
.
You think a combination of a weak antibiotic and a cure for malaria will hurt people?
How? It’s like saying mixing Advil and Tylenol will give you cirrhosis.
In one of Raoults papers was explained that ECG is necessary and why it is necessary – if I remember well.
Both drugs prolong the Q-T interval on the ECG. This risks the development of a potentially lethal tachyarrhythmia, a form of ventricular tachycardia called torsade de pointes. This then leads to death in ventricular fibrillation. Do try to ascertain facts before making foolish remarks. John Cherry, M.B., B.S., F.R.C.S.
FWIW, everyone in the chain, from manufacturer to doctor, is immune from liability concerning chloroquine treatments.
Quite right JP, it’s all well and good that it works in practice, but does it work in theory? That’s the vital question, isn’t it?
We need those old people to just die because the therapy hasn’t been proven yet in a double-blind study. It would be a tragedy if we let people survive prematurely, wouldn’t it?
Why do I have the nagging feeling that some are hoping that HCQ doesn’t work, for fear that the Beast (Trump) might get some credit for a positive action?
This is not Thalamide. It has been used for decades to first treat malaria and now Rheumatoid Arthritis and Lupus. The side effects are all well known. All a properly run double blind will tell you is if some of the claimed successes would have occurred without the drug. In the mean time if it can help people as it appears to do us.
> No double-blind tests.
Are you going be a volounteer for a test?
Please, everyone should read this paper by Dr. Gautret.
Yes, _Jim, Dr Liang has NOT read the paper. Left a message with his emergency dept. operator for him to please read the paper.
Just so that everyone knows that hydrochloroquine nor chloroquine nor azithromycin are anti-viral. The hydrochloroquine acts as an ionophone allowing zinc to enter the INFECTED human cell membrane. Zn+2 then blocks the replicase RdRP, which stops the production of viral RNA and thus viral particles.
MedCram episode 32 on youtube is a great refresher in viral replication.
Thanks to everyone here.
I was very happy that one of the CV sites I follow showed the daily deaths dropping for 3/29.
However, they have a note at the bottom today that reporting from NY state was incomplete on 3/29. There has been an update, but the data for NY may still be incomplete.
That would account for the discrepancy. But even if the figure cited in the news story link be correct, that’s a decline for deaths in NY. As you note, however, that number too might still be incomplete.
Yesterday’s stats have been updated to 363 US deaths and 180 in NY, which are still declines, but less pronounced.
https://www.worldometers.info/coronavirus/country/us/
The difference between midnight GMT and EDT matters.
The numbers dipped last Sunday as well. Though not by this much.
Good point about Sundays.
Still, glimmers of hope for flattening curve sooner rather than later.
However, even if reported new deaths are up again today, the rate of increase is dropping, after a big jump last week.
Yep you have noticed it, I have been watching the counts for about 3 weeks happens every Sunday. They seem to reconcile the numbers on Monday morning.
So how about WUWT keep track of his surge ? Update in , say every three days ? Looking for 1200 people in three weeks. Our local hospital is also looking for surge in three weeks. (VA). The hospital ship, Comfort . Last used as transportation to ….. GITMO ??? BARS on windows?
Here at WUWT, we know all about the wisdom of “experts”.
The ER doctor is talking about epidemiology. That is about as far away as you can get from his actual expertise and still be discussing medicine.
I have no idea if he is right, but on the other hand, he is projecting doom – and he has no idea if he is right.
As of right now, most of the rural counties that are being hit hard have an epicenter of rich, international travelers, such as ski resorts.
I had to laugh at the Rhode Island cops trying to stop New York license plates folks from entering Rhode Island without a quarantine order being given them. The rich just flew in on their private jets to Martha’s Vineyard. The cops are only stopping the Deplorables, you and me. The Rich elitists have their jets and private homes to bypass and fly high above all that nonsense, powered of course with fossil fuels. Just like the climate scam wants to impose.
Martha’s Vineyard is not in Rhode Island.
At a Rhode Island airport, pilot who flew in from NY was told they were not allowed to leave the airport grounds.
Epidemiology is my field. I made my living doing it until I retired. I assure you he’s right. There are two caveats. 1) Social distancing my be working. 2) There is a new emerging treatment namely hydroxychloroquine + zithromax + zinc sulphate being in New York with what appeasements to be very great success. If those two things work his assessment and predictions will be wrong.
If you have an hour, this is a Doc who does CV triage at Weill Cornell in NYC. He has seen a majority of the CV patients coming through their door, which means he has probably some of the most experience with it certainly in the US.
Very common sense and answers some good questions. Puts you at ease. Basically almost all transmission is your hand to your face. Stop touching your face and your chances go waaay down. Casual contact is not an issue (unless they sneeze or cough on you).
re: “Very common sense and answers some good questions. Puts you at ease. Basically almost all transmission is your hand to your face.”
Maybe time to shave the mustache off completely … first time in – multiple decades.
You can trim it and then apply vaseline to make it seal with the mask.
Works on trimmed beards as well.
It seems to me that a box of disposable gloves outside the door of any retail store or restaurant would take care of 90% of the transmission danger.
The problem Pat is “fomites.”
A fomite (or fomes) is any inanimate object that, when contaminated with or exposed to infectious agents (such as pathogenic bacteria, viruses or fungi), can transfer disease to a new host.
your cell phone is a fomite. your wallet/purse and credit card is a fomite. Hard currency Money is a fomite. Your car key is a fomite. Handle those with contaminated, gloved hands, take the gloves off, then handle them again without thoroughly cleaning them…useless gloves. Wash your hands, frequently, clean your smart phone with sanitizer too.
put a condom on your smart fome. 😉
If you are wearing gloves and touch something contaminated, and then touch your face, you will still transmit the virus to yourself.
Yes, gloves are relevant for a till girl handling money all day.
If they provide them at the entrance , they are all contaminated before you get them.
Best thing is to wash you hands as soon as you get home and leave that box of fomites you just purchased in the garage for a couple of days.
I see disposable gloves littering the ground outside of my local grocery store. When the rubber meets the road (no pun intended), no one cares about environmental causes.
Nevertheless, Joel, one puts gloves on going in, and takes them off and throws them away going out. Much of the transmission opportunity is mitigated.
I agree cash money is a problem. Credit cards generally not, given chip readers.
That’s the one. He’s the second doctor to recommend these rational and reasonable steps to limit infection, respond to disease, and mitigate collateral damage (e.g. economic, food distribution).
Are there any CONFIRMED cases of getting Covid from a surface? If so, how many? If not several, why are we so paranoid? I have searched and the only way this seems to be passed is person to person. Yet, we disinfect boxes from Amazon, etc. It’s a free-for-all panic session, as far as I can see.
Not touching your face and washing your hands are prudent in any flu or other outbreak. You’d think people would do this as a matter of course, not just in a pandemic. Of course, restrooms in stores have to tell employees to wash hands before returning to work and how to do so. How helpless we have become.
Exactly. The viruses and other pathogens are out there, they never leave us, we should always take rational and practical, prudent and bold, steps, to limit infection, disease progression, spreading social contagion, and mitigate collateral damage.
baggage handlers in SA 6 confirmed and the other staff to be tested planes diverted and cancellled this arvo in Aus. prior baggage handlers il in usa too
our media says all flights in prior to wipe luggage down
bit(LOT) late
and the diagnosed 18 usa tourists infected the barossa area and to be quarantined? 2 did a runner back home, so the transport to airport the plane n staff n handlers etc plus all your people on ground wherever the ran to..are at risk.
where the hell our so called state of the art screening passports bio id etc went to ?
nobody pulled em up at any stage as they bolted
This article would seem to dispute both you and the doctor. The facts presented are the clearest evidence I have seen to date about how contagious this virus is., and how it is transmitted.
Everyone who went to the practice was aware of COVID19, good hygiene was promoted, no handshakes or hugs. Yet the vast majority of those who attended got COVID 19. Airborne transmission is much easier than most realize.
https://www.latimes.com/world-nation/story/2020-03-29/coronavirus-choir-outbreak
UK Covid-19 Monday update here:
http://www.vukcevic.co.uk/UK-COVID-19.htm
Empowering and protecting your family during the COVID19 pandemic
– Dr. David Price, Weill Cornell Medical Center
* social distancing (3 ft)
* hand to face hygiene
* coexisting with people (especially in close proximity) who are infected, who have the disease
* when to visit the hospital (e.g. resource management), and triage (e.g. telemedical services)
Bottom-line: We don’t have to shut down the country. We should avoid spreading a social contagion. There are rational and reasonable steps to take in order to mitigate infection, respond to disease, to manage resources, and to mitigate collateral damage.
“* social distancing (3 ft)”
Clearly, 97% of Medical Scientists don’t agree about this, or the UK requirement wouldn’t be 2 metres (6′ 6″)…
Same 2m separation requirement in Canada. Of course, it’s easy to measure here, as we all carry hockey sticks. 🙂
Has the death rate by hockey stick spiked yet 🙂
To make it easier for people to understand, 2 meters would be 1 Darth Vader.
I saw this the other day. It would be interesting if somebody could weigh in…
https://www.citizenfreepress.com/breaking/er-doctor-offers-lessons-on-treating-covid-19-patients-cheat-sheet-for-physicians-excellent-read/
“A very few very lucky people may not develop any symptoms at all.”
There was an article on the Diamond Princess stats published here the other day; 80% of passengers didn’t even test positive for the virus and, of those that did, 50% were asymptomatic. It may be that the lock down on the Diamond Princess was very, very effective, but the suggestion from its experience is that the “very few very lucky people” may be better phrased as “very few very unlucky people will develop symptoms, and even fewer may die”.
In the UK, as of today (from the UK government website) “As of 9am on 30 March 2020, a total of 134,946 people have been tested, of which 112,805 were confirmed negative and 22,141 were confirmed positive.” Now, given that there is, as far as I’m aware no random testing going on, the suggestion is that the 135k people who’ve been tested have more than likely been exposed to the virus somehow to the extent it was felt necessary to test them, yet 83% of those were negative.
It’s all very, very interesting.
as far as I’m aware no random testing going on, the suggestion is that the 135k people who’ve been tested have more than likely been exposed to the virus somehow to the extent it was felt necessary to test them,
Or they were exhibiting symptoms that turned out to not be Wuhan virus related (IE they had the flu or other common cold instead).
Yes John I agree. We are unaware of the outcome for the 112,805 confirmed negative. How many had symptoms? How many subsequently died? It is only with these data that we can make a comparative assessment of the additional danger associated with being tested positive.
This is not “interesting”. Every word of this letter is important to your life.
“Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV2)”
https://science.sciencemag.org/content/early/2020/03/24/science.abb322
My summary: those researchers estimated that 5 of 6 (86%) infected individuals from the initial spread of the SARS-CoV-2 out of Wuhan China went undetected, likely because of low/no symptoms.
It is everywhere now.
Corrected URL:
https://science.sciencemag.org/content/early/2020/03/24/science.abb3221
John, you say ” It may be that the lock down on the Diamond Princess was very, very effective”. You may be right except the lockdown did not happen for at least 10 days. The ship left port on Jan 20 with the virus on board. The first case to test positive was on Feb 1. Locking down started after that date and I suspect not completely and immediately. .5% of 300,000 county residents may not be a bad number though. Worldometer shows 10 deaths and 15 serious cases from the 3700 Diamond. I don’t now if deaths and serious numbers are separate or should be totaled. It also shows first case as of Feb 4 which conflicts with other reports. Lots of sloppy info out there.
The country that is performing the most random tests in the world is Iceland. Take a look at their updated data at https://www.covid.is/data. Most other countries are only testing people who are showing very likely cases so we have little idea the effects of COVID-19 on the general population. According to Icelandic data – 1086 people have the virus, 30 people are hospitalized, 10 in the ICU and 2 have died. This shows less than 3% of the population have a severe case and COVID-19 is lethal in less than 1%. If these are the true statistics of the virus in the general population then most governments are overestimating the impact from the virus. Icelandic projections do not anticipate anyone under 55 will end up in the ICU https://covid.hi.is/english/. Perhaps Icelanders are on average healthier than the general population, however this is perhaps the best data to work from that is available.
Have you bothered to look at Germany’s test rate?
Diamond Princess was full of relatively healthy older people, and the “lockdown” didn’t happen anywhere near as soon as it should have. Even so, only 20% of the occupants were infected? And only 50% of those were symptomatic? 10% of the occupants were symptomatic?
Everytime I see statistics for Corona, it becomes more obvious that this is nothing than a typical flu.
Average Flu mortality rate 0.1%, Princess Diamond mortality rate 1.3% with Quarantine.
When was the last time you were quarantined for flu?
Excellent article.
I would debate 2 points, however. Will almost “everyone” be exposed? Maybe not. And over how long a period will it take for this exposure? Certainly, if 300,000 people were exposed simultaneously, you would see a mass run on ICU treatment. One hopes it is spread out over an extended period, giving time for beds to clear as new cases come in. It would be interesting to hear how long a bed is occupied during a patient’s ICU period.
Hopefully the “bow-wave” will not be as dire as predicted, but certainly must be taken into consideration for any preparations that can be made for an “educated” estimate of demand and resource preparation. It would be nice if we could be resourced for the very worst, but that is not always possible.
Time will tell.
Why don’t you look at the data yourself, some of the Princess Diamond patients are still in ICU over a month later.
You, me, everyone,… we’re all going to get SAR-CoV-2 infection… if you haven’t already (and recovered). Period.
This virus is widespread and circulating right now everywhere except maybe the most isolated villages or closed communities.
Any tested/safe/ effective/approved vaccine will arrive too late with the 100’s of millions of doses needed to stop this now through our communities. It won’t be available for at least 16-18 months, and then it will be a relatively moot point. It’ll be moot issue because it will be too late to be of any use today or through the next-Fall-Winter cold and flu season.
All we are doing now is flattening the time-response demand curve for ICUs and ventilators.
The problem we are faced with, as both individuals and as a society, is … Choice.
I’ll let the Architect explain the in his eloquence.
You think the Architect could afford large flat panel displays.
Joel O’Bryan
Thank you / Danke / Merci.
J.-P. Dehottay
“Even more seriously, the economy is heading downhill and many people are not getting paychecks.”
At least he acknowledges the economy.
Still, he doesn’t do anything beyond acknowledging it. Yeah, the absolute worst-case-if-we-do-nothing-not-even-wash-our-hands predictions show some hospitals might get surges. But shutting down the global economy indefinitely has repercussions, too, which are a lot more severe than “people not getting paychecks”.
This is the whole problem with minimaxing things like this. You get near 0 deaths from the coronavirus in exchange for death and destruction and tyranny worldwide indefinitely. But hey! The coronavirus didn’t kill those people or ruin their lives! Declare victory, I guess.
We need finger prick blood test for Covod-19 antibodies YESTERDAY!
Just go hang out at Walmart and push random shopping carts around without any gloves, surgical mask, and touch your face, wipe your nose. Then isolate for 2 weeks. If you didn’t have the corona virus already and protective immunity, you will after that in 2 weeks. Just have enough stuff to stay isolated for 14 days.
I have already been to Whole Foods, Target, and Walmart multiple times since this whole thing started.
Because the only truth the doctor stated was:
“The virus is highly contagious. It is predicted that eventually, nearly everyone will be exposed and been infected. ”
Gloves and mask in the general public are at best false security, like Linus and his blanket from the Peanuts comics.
If you are not matching the mask to the size of the particle you trying to exclude you are not doing thing but going through the motions. If you touch your glove on something not sterile even if you have sterilized, sanitized, disinfected the glove then it immediately becomes contaminated. The outside world is not free of viruses or bacteria, it is on every square mm inside and outside of a human being. I have even heard that the seed of nearly every single snowflake that falls from the sky is some form a bacteria.
The human body is a learning a machine in multiple ways all concurrently. Herd immunity will be way faster then any vaccine we will develop.
Are you sure you did not read that on a Trivial Persuits card ?
I would have thought that aircraft exhaust is a significant source of condensation nuclei to judge by contrial formation and persistence under suitable conditions.
BTW, bacteria is the plural: a bacterium.
Even better, Abbott Labs has an approved molecular tester which does it in 5 – 13 minutes.
https://www.abbott.com/corpnewsroom/product-and-innovation/detect-covid-19-in-as-little-as-5-minutes.html.html
Joe Diffie Releases Statement
NASHVILLE, Tenn. – GRAMMY®-winning country music legend Joe Diffie has tested positive for coronavirus (COVID-19) and has released the following statement:
“I am under the care of medical professionals and currently receiving treatment. My family and I are asking for privacy at this time. We want to remind the public and all my fans to be vigilant, cautious and careful during this pandemic.”
–Joe Diffie
https://edition.cnn.com/2020/03/29/us/joe-diffie-coronavirus-death-trnd/index.html
He died.
A downer for Pickup Man. He should have lost about a hundred pounds, long ago.
Two days after his statement.
“U.S. deaths from the coronavirus doubled over the weekend…” USA Today, 3/30/20
No, they didn’t you lying weasels!!!
Per the attached graphic based on UCDC data cases and deaths just stepped off a cliff!
I expected by now to see satellite images of Chinese CoVid apocalypse bodies stacked by the tens of thousands in city squares, bulldozers pushing them into mass graves then covered with lime.
According to ECDC and WHO the CoVid death toll for China is about 3,300. A mortality rate once in double digits has fallen to 4.0%.
The US at 2,500 will surpass that shortly.
Where is the footage of CoVid apocalypse zombies staggering across hospital parking lots, storming ERs and hallways?
Not there – so far. Mostly just isolated anecdotal tear jerkers.
This lying, fact free, fake news MSM’s fake pandemic is as fake as fake dying polar bears, fake rising sea levels, fake melting ice caps, fake man caused climate change.
President Trump should bring the full weight of the Federal Government to bear, sue the fake news MSM for crying “Wolf,” for yelling “Fire!” in our crowded theater, make them pick up that 2.2 trillion dollar tab.
Rights have responsibilities. Yeah, weird notion.
Trump should burn the fake news media to the ground and when/if it rises from the ashes maybe it will understand what honest, balanced, objective, responsible journalism means.
BTW looks like US cases and deaths just fell over a cliff. An uptick this large makes headline news. We’ll see if it stays that way.
Nick Schroeder
Your aggressive comment shows how good ignorance and arrogance can fit together in one crank brain.
The day isn’t at end yet, and we have over 800 deaths in Italy, over 500 in Spain, over 400 in France. Every day, the ration ‘death toll per cases’ increases.
And you stay behind your notebook and cowardly write “fake pandemic”…
You should be sent by law right tomorrow in the morning to one of these hospitals in Italy, Spain, France, where permanently stressed and totally tired staff tries – at their own risk – to keep patients alive.
In Italy, over 50 of them died until now: because they could not obtain masks let alone protection clothes!
My personal meaning: people like you are simply disgusting.
J.-P. Dehottay
re: “Your aggressive comment shows how good ignorance and arrogance can fit together in one crank brain.
The day isn’t at end yet, and we have over 800 deaths in Italy, over 500 in Spain, over 400 in France. Every day, the ration ‘death toll per cases’ increases.”
This is the same poster who decries the methods and means of Dr. Raoult (AND do not forget his team and associates in the medical and research fields!) who is working towards an effective treatment? How can one man’s brain entertain such divergence of thought w/o locking up with veritable cognitive dissonance? One is driven to as the question: Whose side are you on – the virus or humanity?
See my reply to your insulting comment, and… start thinking instead of writing unnecessary, aggressive stuff.
J.-P. D.
“Your aggressive comment shows how good ignorance and arrogance can fit together in one crank brain.”
Pot. Kettle. Black.
That is what you will get if you are silly enough to compare today’s fatalities to today’s cases. There is a lag between diagnosis and death.
French data shows a lag of 13d in stats with a scaling factor of 50%.
The exponential of fatalities is dropping marginally quicker than new cases and this could become quite significant in 14 days time. ie we are probably not on course to see half the current daily case load die in 13 days.
New cases is probably heavily dependent on availability of test kits and administration policy at any point in time. Extreme caution is required before drawing any conclusions from such poorly sample and poorly documented data.
BTW Italy , Spain and Germany new daily cases all seem to have peaked now.
Greg
” That is what you will get if you are silly enough to compare today’s fatalities to today’s cases. There is a lag between diagnosis and death. ”
Merci beaucoup, Monsieur l’instituteur!
As you should have imagined, I’m not at all interested in the comparison as such, but only in how it develops over time. The lag then is of no interest, because it is an invariant.
” BTW Italy , Spain and Germany new daily cases all seem to have peaked now. ”
Yes. ‘seem’ indeed is the right word, especially for… Spain:
6368, 6922, 7457, 8271, 7933, 7516, 6875, 7846
I think I’ll wait for a couple of days before speaking of ‘peaked now’.
J.-P. D.
“The lag then is of no interest, because it is an invariant.”
The lag is invariant but you are looking at exponential growth in both cases and deaths where rate of change is also exponential . If you had two linear relationships you could argue that the instantaneous ratio was valid estimation of the death toll.
Both cases and fatalities are growing roughly exponentially , say exp(c*t) and exp(f*t). The ratio F/C is exp((f-c)*t) , also an exponential !
Shock horror: it is currently “developing over time” because it is exponential. Later it will fall, quite dramatically. That is why you cannot calculate the death toll until you are nearing the end of the epidemic.
Not only are you too ignorant of the maths to see what you are doing is meaningless , you are too pigheaded to realise it when it is explained to you.
Despite apparently posting from Germany, you are obviously French not German. Germans tend to very sure of their opinions too but usually because they know what they are talking about , or else they have the sense to shut up.
Eh ben, dis donc.
I’m glad you agree that “seem” is the right word. That is why I used it.
Je suis absolutment d’accord, mon brave. Continuez, je vous en prie, avec vos observations rationnelles. Ce sont beaucoup rare ici. Apologies for not knowing how to put in a circumflex accent or a cedilla on this keyboard.
The coronavirus deaths just in the Wuhan area are estimated at 35,000-60,000 simply based on what is known about Wuhan crematorium and their delivery of urns. That number is > 10x what the official Communist Chinese press is reporting.
Other data also show the extent of ChiCom regime’s lying, such as huge drop in cell phone contracts.
https://www.bloomberg.com/news/articles/2020-03-23/china-s-mobile-carriers-lose-15-million-users-as-virus-bites
Some of the 21 million lost users might be closed businesses, but the bloody tyrants have to be covering up blatantly the extent of death and disease. Yet their shills in Western media tout the great success of Communism in combating the plague their lack of honesty allowed to spread around the world.
I think the CCP used this as an opportunity to purge political opponents.
Nick Schroeder
“President Trump should bring the full weight of the Federal Government to bear, sue the fake news MSM for crying “Wolf,” for yelling “Fire”
Except Trump is the one yelling fire the loudest now. He was talking about the “potential” for 2.2 million deaths in the US at yesterdays briefing.
Simon I can see that you and Trump are on the same page.
You want the borders closed and Boom he closed them.
You wanted flights from China stopped and Boom he stopped them.
You wanted Social Distancing and Boom he asked for social distancing
You wanted more testing and Boom he orders more testing.
You wanted to shut down most of the economy and Boom he shut most of it down
You wanted monetary relief for those impacted by the shut down and Boom your relief is on its way.
You wanted more deaths predicted and Boom he predicts more death.
Birds of a feather flock together.
Derg
I know you think you are psychic, but….
You want the borders closed and Boom he closed them. Yep
You wanted flights from China stopped and Boom he stopped them. Yep and other places.
You wanted Social Distancing and Boom he asked for social distancing Yep
You wanted more testing and Boom he orders more testing. Yep
You wanted to shut down most of the economy and Boom he shut most of it down. Nope. I’d rather we didn’t shut any of it down.
You wanted monetary relief for those impacted by the shut down and Boom your relief is on its way. I don’t want any money but I get that those at risk do.
You wanted more deaths predicted and Boom he predicts more death. I want honesty and to listen to the experts.
We are pretty close in agreement. It’s a funny thing about listening to experts, at one time experts thought giving antacids to people with ulcers. Settled science is what they would have said back in the day.
Experts indeed.
You wanted more deaths predicted and Boom he predicts more death. I want honesty and to listen to the experts.
Eh? You are complaining about Trump talking about “potential” for 2.2 million deaths in the US . Trump got that number *FROM* listening to the experts. Admit it, no matter what Trump does, you’ll find fault even when he does the very things you claim to want.
It’s a funny thing about listening to experts,…
Indeed. and who are the experts that decide which experts are the experts worth listening to and which are the ones not worth listening to? The fact is you can find experts with impeccable credentials that completely disagree with other experts with equally impeccable credentials.
This fake report is totally bogus scare-mongering false news.
Total US cases:
Thursday: 68,211
Friday: 104,126; +35,915
Saturday: 123,578; +19,452
Sunday: 143,491; +19,913
The only way that they could claim doubling was by adding up new cases Sat and Sun and comparing with new cases on Friday!
Proper reporting would have been to say that the daily increase was almost cut in half, despite more testing.
US has basically stabilized 20K new cases per day.
Please leave the statistics alone. Only the time will come. If you want to keep your family healthy, ask your doctor what is the situation in your area. Ask how many doctors are in quarantine. This doctor will tell you the truth about this disease.
Ren, I appreciate your comments. One of my physicians recently cancelled a long-standing appointment (not for anything critical) to take a two-week vacation or break. His office remains open, though with precautions in place. I can only speculate that he may have been exposed.
The only two statistics that matter to me are (1) excess deaths over other causes and (2) excess ICU cases. The number of infected and projections based on that are just lying with statistics at this point. The death numbers are even tainted by the fact that most had other conditions and might have died from regular flu just as easily. Same for ICU numbers – regular flu and other underlying conditions would have put people in ICU as well. The important statistics are excess related to COVID-19 only, which are hard to even measure let alone report our by scientifically illiterate press.
The sooner we get to a blood test to find those post-infected and immune for this season the better. Then we get quit the draconian quarantining of everyone and concentrate on those most at risk.
Here in Alberta we have less than 0.5 hospitalizations per hospital. 0.13 ICU admissions per hospital. Those healthcare workers must be overloaded!
I work as an infectious disease doctor here in Calgary. You have accurately described the low impact at present. All the panic is around the expected future surge. I go to work presently and have a much smaller roster of patients to care for than usual. What will the surge look like? No one knows. Modelling can make almost any prediction one can imagine especially when the models never undergo validation.
Worldometers is tardy on that stat. JH shows 177 recovered:
https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6
But it agrees with Worldometers on UK deaths.
“A very few very lucky“
How do they know unless we can test people that have had COVID and did not show symptoms or showed symptoms and never bothered to see a Dr?
This site has daily interactive projections for all US states:
https://covid19.healthdata.org/projections
The Institute for Health Metrics and Evaluation (IHME) is an independent global health research center at the University of Washington.
It looks like “The Surge” will occur at different times and levels for many states.
The projections include ICU beds needed as well as ventilators and deaths per day.
The US total deaths by Aug 4 is 82,141. Most places will level off by the beginning of June.
Here in Vermont they expect that to occur in the beginning of May.
We shall see.
Or, if you prefer, The Lancet:
https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)30120-1/fulltext
Whatever. In Lexington, KY where I practice virtually all healthcare workers are losing hours. I’ve had to change jobs to keep from being called off. Any ‘surge’ will be handled easily just as we handle influenza every year.
I refuse to change my daily habits any more than I am forced to because of a manufactured panic. When Covid numbers start to resemble those of influenza then I’ll consider taking real notice.
Kentucky has one of the lowest rates in the country.
You should be glad you don’t live elseware.
Count your blessings!
https://covid19.healthdata.org/projections
We do have a lower infection rate but deaths aren’t all that lower than in states with higher infection rates (don’t have the numbers handy, sorry). But at what cost?
I am in contact with a computer savvy friend who sent me these 2 links in answer to my question, ‘who is reporting all the figures to the John Hopkins University dashboard?’
*********
John Hopkins answer your questions here:
https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6
see bottom centre, and then this link
https://systems.jhu.edu/research/public-health/ncov/
**********
From my reading of the JHU figures I still dont have an answer. They are reported almost in real time so JHU must be obtaining information from someone. Who is it? The WHO or each countries’ health agencies? How was the system set up and how did they know to report to the JHU database?
The UK government appears to be basing its public order restrictions on the JHU figures. Are they accurate enough for the resulting disruption to have been implemented? Can the reported figures be confirmed? Does Covid-19 appear on the death certificates of those who have died from it?
There appears to be a link between John Hopkins University and Event 201, held in Oct 2019, where many imminent scientists from numerous world renowned organisations assembled to discuss the implications for a world wide virus pandemic. Excellent timing, so what was proposed?
The UK government will almost certainly have it’s own figures … ask someone in UK.
John Hopkins University had the database setup to run simulations for the event you describe. Individuals possibly those who attended and knew it existed have joined with it to collate the data. That is why not every country has individual links, many are just black entries from official country figures. In almost all cases the number reported is just as reported by the government and they seem to audit the data back to official government figures.
So you have it backwards countries are feeding data to John Hopkins University not the other way around.
Thanks for your observations about the UK govt’s reporting. I have asked, no-one knows where the UK figures come from. So my original question remains unanswered. Who reports the UK figures to the JHU dashboard? How are they collated? Does Covid-19 appear on any death certificates being included as being deaths caused by this virus?
I have assumed that all countries do their own reporting to the JHU database. So who exactly does the reporting? Are they accurate enough for the political descisions being made at such huge cost to us all?
The testing regime introduced by the UK govt has signally failed; they have not got the kits with which to carry out reliable tests. The NHS workers who are a priority are still waitng to be told where to go to be tested.
It is a complete shambles, but fortunately us Brits are so used to that we just get on with life and ignore the noise. When this virus is all that is being reported on every TV channel I do wonder what else is happening we are not being told about. Anyone?