UPDATE: A Covid-19 case correlation between malarial and non-malarial countries has been plotted by Dr. Roy Spencer, and the results are stunning – see below.
Encouraging news: three new medical studies show a commonly available anti-malaria drug known as chloroquine aka chloroquine phosphate is showing strong results against COVID-19 infections in both China and South Korea. Excerpts from three studies, including one published in Nature are below.

An Effective Treatment for Coronavirus (COVID-19)
Presented by: James M. Todaro, MD and Gregory J. Rigano, Esq.
In consultation with Stanford University School of Medicine, UAB School of Medicine and National Academy of Sciences researchers.
Translation by: Celia Martínez-Aceves (Yale B.S. Candidate 2021), Martín Martínez (MIT B.S. 2017)
Summary
Recent guidelines from South Korea and China report that chloroquine is an effective antiviral therapeutic treatment against Coronavirus Disease 2019. Use of chloroquine (tablets) is showing favorable outcomes in humans infected with Coronavirus including faster time to recovery and shorter hospital stay. US CDC research shows that chloroquine also has strong potential as a prophylactic (preventative) measure against coronavirus in the lab, while we wait for a vaccine to be developed. Chloroquine is an inexpensive, globally available drug that has been in widespread human use since 1945 against malaria, autoimmune and various other conditions.
Chloroquine: C18H26ClN3
Background
The U.S. CDC and World Health Organization have not published treatment measures against Coronavirus disease 2019 (“COVID-19”). Medical centers are starting to have issues with traditional protocols. Treatments, and ideally a preventative measure, are needed. South Korea and China have had significantly more exposure and time to analyze diagnostic, treatment and preventative options. The U.S., Europe and the rest of the world can learn from their experience. According to former FDA commissioner, board member of Pfizer and Illumina, Scott Gotlieb MD, the world can learn the most about COVID-19 by paying closest attention to the response of countries that have had significant exposure to COVID-19 before the U.S. and Europe.[1]
As per the U.S. CDC, “Chloroquine (also known as chloroquine phosphate) is an antimalarial medicine… Chloroquine is available in the United States by prescription only… Chloroquine can be prescribed for either prevention or treatment of malaria. Chloroquine can be prescribed to adults and children of all ages. It can also be safely taken by pregnant women and nursing mothers.”[2]
CDC research also shows that “chloroquine can affect virus infection in many ways, and the antiviral effect depends in part on the extent to which the virus utilizes endosomes for entry. Chloroquine has been widely used to treat human diseases, such as malaria, amoebiosis, HIV, and autoimmune diseases, without significant detrimental side effects.”[3]
The treatment guidelines of both South Korea and China against COVID-19 are generally consistent, outlining chloroquine as an effective treatment.
Specifically, according to the Korea Biomedical Review, in February 2020 in South Korea, the COVID-19 Central Clinical Task Force, composed of physicians and experts treating patients agreed upon treatment principles for patients with COVID-19.[4] In China, the General Office of the National Health Commission, General Office of the State Administration of Traditional Chinese Medicine as well as a Multi-Center Collaborative Group of Guangdong Provincial Department of Science and Technology and Guangdong Provincial Health Comp and the China National Center for Biotechnology Development have established effective treatment measures based on human studies.[5]
According to their research (reported in Clinical Trials Arena),
“Data from the drug’s [chloroquine] studies showed ‘certain curative effect’ with ‘fairly good efficacy’ … patients treated with chloroquine demonstrated a better drop in fever, improvement of lung CT images, and required a shorter time to recover compared to parallel groups. The percentage of patients with negative viral nucleic acid tests was also higher with the anti-malarial drug… Chloroquine has so far shown no obvious serious adverse reactions in more than 100 participants in the trials… Chloroquine was selected after several screening rounds of thousands of existing drugs. Chloroquine is undergoing further trials in more than ten hospitals in Beijing, Guangdong province and Hunnan province.”[6]
…
Chloroquine as a prophylactic (preventative) measure against COVID-19[11]
According to research by the US CDC, chloroquine has strong antiviral effects on SARS coronavirus, both prophylactically and therapeutically. SARS coronavirus has significant similarities to COVID-19. Specifically, the CDC research was completed in primate cells using chloroquine’s well known function of elevating endosomal pH. The results show that “We have identified chloroquine as an effective antiviral agent for SARS-CoV in cell culture conditions, as evidenced by its inhibitory effect when the drug was added prior to infection or after the initiation and establishment of infection. The fact that chloroquine exerts an antiviral effect during pre- and post-infection conditions suggest that it is likely to have both prophylactic and therapeutic advantages.”
The study shows that chloroquine is effective in preventing SARS-CoV infection in cell culture if the drug is added to the cells 24 h prior to infection.
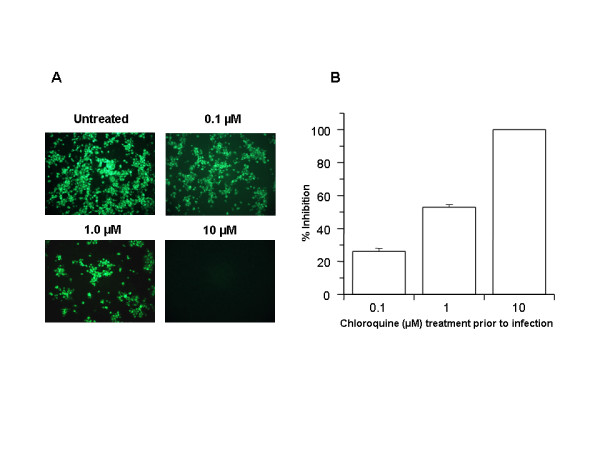
FIGURE 1
Prophylactic effect of chloroquine. Vero E6 cells pre-treated with chloroquine for 20 hrs. Chloroquine-containing media were removed and the cells were washed with phosphate buffered saline before they were infected with SARS-CoV (0.5 multiplicity of infection) for 1 h in the absence of chloroquine. Virus was then removed and the cells were maintained in Opti-MEM (Invitrogen) for 16–18 h in the absence of chloroquine. SARS-CoV antigens were stained with virus-specific HMAF, followed by FITC-conjugated secondary antibodies. (A) The concentration of chloroquine used is indicated on the top of each panel. (B) SARS-CoV antigen-positive cells at three random locations were captured by using a digital camera, the number of antigen-positive cells was determined, and the average inhibition was calculated. Percent inhibition was obtained by considering the untreated control as 0% inhibition. The vertical bars represent the range of SEM.
…
In addition, the study also shows that chloroquine was very effective even when the drug was added 3–5 h after infection, suggesting an antiviral effect even after the establishment of infection.
…
The UK has banned the export of Chloroquine[13]
As of February 26, 2020, the UK government has added chloroquine to the list of medicines that cannot be parallel exported from the UK. Chloroquine was never on this list before. This likely happened because of the growing body of evidence of chloroquine’s effectiveness against coronavirus.
China prioritizes internal use of Active Pharmaceutical Ingredients (APIs) including Chloroquine[14]
In early February, Chongqing Kangle Pharmaceutical was requested by the Ministry of Industry and Information Technology, Consumption Division to promptly increase the manufacturing and production of the active pharmaceutical ingredients chloroquine phosphate despite slowed production during the Chinese New Year.
…
Conclusion
Chloroquine can both both prevent and treat malaria. Chloroquine can prevent and treat coronavirus in primate cells (Figure 1 and Figure 2). According to South Korean and China human treatment guidelines, chloroquine is effective in treating COVID-19. Given chloroquine’s human safety profile and existence, it can be implemented today in the U.S., Europe and the rest of the world. Medical doctors may be reluctant to prescribe chloroquine to treat COVID-19 since it is not FDA approved for this use. The United States of America and other countries should immediately authorize and indemnify medical doctors for prescribing chloroquine to treat COVID-19. We must explore whether chloroquine can safely serve as a preventative measure prior to infection of COVID-19 to stop further spread of this highly contagious virus.
Full study available here
Then there’s this second study:
Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studiesJianjun Gao, Zhenxue Tian, Xu Yang
Abstract
The coronavirus disease 2019 (COVID-19) virus is spreading rapidly, and scientists are endeavoring to discover drugs for its efficacious treatment in China. Chloroquine phosphate, an old drug for treatment of malaria, is shown to have apparent efficacy and acceptable safety against COVID-19 associated pneumonia in multicenter clinical trials conducted in China. The drug is recommended to be included in the next version of the Guidelines for the Prevention, Diagnosis, and Treatment of Pneumonia Caused by COVID-19 issued by the National Health Commission of the People’s Republic of China for treatment of COVID-19 infection in larger populations in the future.
https://www.jstage.jst.go.jp/article/bst/14/1/14_2020.01047/_article
Finally, there’s a new study in the prestigious journal Nature:
Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro
Excerpt:
Chloroquine, a widely-used anti-malarial and autoimmune disease drug, has recently been reported as a potential broad-spectrum antiviral drug.8,9 Chloroquine is known to block virus infection by increasing endosomal pH required for virus/cell fusion, as well as interfering with the glycosylation of cellular receptors of SARS-CoV.10 Our time-of-addition assay demonstrated that chloroquine functioned at both entry, and at post-entry stages of the 2019-nCoV infection in Vero E6 cells (Fig. 1c, d). Besides its antiviral activity, chloroquine has an immune-modulating activity, which may synergistically enhance its antiviral effect in vivo. Chloroquine is widely distributed in the whole body, including lung, after oral administration. The EC90 value of chloroquine against the 2019-nCoV in Vero E6 cells was 6.90 μM, which can be clinically achievable as demonstrated in the plasma of rheumatoid arthritis patients who received 500 mg administration.11 Chloroquine is a cheap and a safe drug that has been used for more than 70 years and, therefore, it is potentially clinically applicable against the 2019-nCoV.
Our findings reveal that remdesivir and chloroquine are highly effective in the control of 2019-nCoV infection in vitro. Since these compounds have been used in human patients with a safety track record and shown to be effective against various ailments, we suggest that they should be assessed in human patients suffering from the novel coronavirus disease.
A commonly available over-the-counter quinine source exists in Margosa Tree Bark and Cinchona succirubra, Peruvian Bark


Tablets of bark extract are widely available in tablet form, from many sources, including Amazon.com here.
There’s also quinine in Tonic Water, which is available just about anywhere at any grocery or liquor store and also at Amazon:
Tonic water is a soft drink containing quinine, which gives it a bitter taste. Quinine is a common treatment for malaria. Quinine comes from the bark of the cinchona tree.
UPDATE:
From Facebook, Dr. Roy Spencer adds this new information.- Anthony
On the subject of using antimalarial drugs for COVID-19 treatment, I’ve compared COVID-19 cases versus malaria incidence by country….
This is amazing. I downloaded all of the data for 234 countries, incidence of total COVID-19 cases (as of 3/17/2020) versus the incidence of malaria in those countries (various sources, kinda messy matching everything up in Excel).
RESULTS, Multi-country average malaria cases per thousand, COVID-19 cases per million, in three classes of countries based on malaria incidence:
- Top 40 Malaria countries: 212 malaria = 0.2 COVID-19;
- Next 40 Malaria countries: 7.3 malaria = 10.1 COVID-19
- Remaining (81-234) countries: 0.00 malaria = 68.7 COVID-19
Again, the units are Malaria cases per thousand “population at risk”, and COVID-19 cases per million total population.
In all my years of data analysis I have never seen such a stark and strong relationship: Countries with malaria basically have no COVID-19 cases (at least not yet).
Additional support for antimalarial drugs for COVID-19 treatment comes from this investigation linked below.
The map says it all: COVID-19 is where Malaria is not.

Discover more from Watts Up With That?
Subscribe to get the latest posts sent to your email.
Does the coronavirus exist?
https://www.greenmedinfo.com/blog/does-2019-coronavirus-exist
In other news close to me multiple gas stations selling gas for $1.49 / gallon.
One gas station in USA was selling for 99 cents / gallon. Though this could be marketing ploy to get in the news.
I got today’s data from https://www.worldometers.info/coronavirus/ and sorted it by “Cases per million population” descending.
The top 10, in order, were: San Marino, Faeroe Islands, Vatican City, Iceland, Andorra, Luxembourg, Liechtenstein, Italy, Switzerland, Spain. The top seven are all small countries. (BTW, San Marino is an enclave within Italy.) So, small countries tend to report more cases per head than large ones? Seems a bit odd. Are small countries better at counting cases than large ones? Or does the virus spread more easily within a smaller culture?
Adding a column for deaths per million population, sorting by that, and discounting countries which have only reported 1 death, the top 10 are now: San Marino, Italy, Spain, Iran, Luxembourg, France, Switzerland, Netherlands, China, UK. That gives some idea of the geographical spread. But I wouldn’t be surprised if Chinese and Iranian deaths have been under-reported.
If I just sort by deaths per case, and again exclude those with only 1 death, the top 10 are: Ukraine, Algeria, San Marino, Indonesia, Italy, Philippines, Iran, Iraq, Dominican Republic, Spain. I don’t think that tells us much right now, except for calling into question the theory that the virus can’t survive in hot weather – three of those countries are tropical. When the whole thing is over, however, this metric may give us some interesting comparisons between the efficacy of health systems in different parts of the world.
There are all kinds of interesting questions. There are problems with small data sets and this would seem to apply to small countries. Remember that a single nursing home in Washington state dominated and skewed the U.S. statistics for some time. Even today, I think the intercept in the trend line of deaths vs cases in the U.S. is at least party due to that outbreak.
With regard to virus survival in hot weather, keep in mind the effect of travel – i.e., a person can pick up the virus in one country and carry it to another. We reasonably know where the Wuhan virus originated. It stands to reason that conditions favorable to its environmental survival existed in Wuhan at the time of the outbreak and animals are carriers.
There were direct flights from Wuhan to several airports in the U.S., Canada, Japan, Hong Kong, Singapore, Taiwan, Indonesia, South Korea, Thailand and several other localities, especially cities within China (where there are also many train connections) with either hotter, colder or similar weather prevailing in Wuhan at the time. It appears that there are preferred range of weather conditions for survival of the virus based on community transmission from import. There is at least one paper from China that discusses this.
Cutting off the transport of the virus is the key to ending propagation. Part of this would seem to be creating conditions that are unfavorable to its survival within the community, cleaning, adjusting temperature, humidity, etc. More research is needed of course.
Your question about virus spread in a smaller culture is interesting. Once it’s there it probably does spread if there is a lot of social interaction and that culture is especially susceptible to infection. I imagine that a lot of praying is going on in Vatican City.
I would like to see the rate of virus spread for hotter climates vs colder climates.
In Texas it appears rate of spread is not as fast, but I don’t have daily numbers by state to say this for sure.
I have been watching Thailand’s cases because they have lots of Chinese tourism and hot climate. The rate is not too high but they recently got another 60 cases of which 42 tied to large people gatherings.
In the UK there are two malaria drugs Chloroquine (prescription, mentioned by president Trump) and Qualaquin (available without prescription), both have side effects, the most serious are:
Chloroquine – Anxiety (attempts at killing oneself)’
Qualaquin – Anxiety (behaviour change, similar to drunkenness)
If need be, I’ll rather be drunk than suicidal.
🙂
Chloroquine Side Effects
https://www.drugs.com/sfx/chloroquine-side-effects.html
Qualaquin Side Effects
https://www.drugs.com/sfx/qualaquin-side-effects.html
Whatever you do, don’t take chloroquine prior to a first date.
If you check the side effects for Aspirin on drugs.com you wouldn’t take them either. At the top of the list of side effects they say that there is no data on the frequency of the side effects.
“…So, small countries tend to report more cases per head than large ones? Seems a bit odd. Are small countries better at counting cases than large ones….”
Any measure ‘per capita’ is skewed by the small population number that you divide by. Look at Nobel prizes per head of population. The top two countries are the Faroe islands and St Lucia. That does NOT mean that these countries are supremely intelligent. It just means that they are so small that a random one Nobel laureate living there (or TWO in the case of St Lucia!) catapults the country to the top of the list….
Well yes, the Faeroe Islands did produce a Nobel prizewinner. But I don’t think that having a small sample size will skew a per capita measure towards the right – i.e. above the average of a much larger sample (from the same population). Surely, a small sample size makes the uncertainty bigger – you’re much more likely to get an outlier like the one you quoted. But it doesn’t increase the expected value.
There have been 80 confirmed cases so far in the Faeroes; no-one has died from it there. If you took a similar sample size from, say, Denmark (to which the islanders are closely culturally related), then on the current numbers you’ d expect about 10 cases. Their new infections per day appear to be dropping, even though the number tested is going up each day; so hopefully they’re almost through.
The Chief Medical Officer of the Faeroes said on Tuesday (according to Wikipedia) that at this point, most people have been infected within the Faroe Islands. That suggests that the virus spread unusually fast in an isolated community. That could also be what happened in Iceland, and might also be why Andorra and Liechtenstein have more cases per population than the surrounding countries. What’s going on in San Marino is anyone’s guess, but that’s a place I wouldn’t want to be right now.
Why not use the plasma of those who have recovered, if this could be the only rescue?
If you do not manage to develop antibodies, that no drug will help.
I cordially greet.
Ren: You attack it from both sides. Weaken the ability (slow down) of the virus, to give your immune system help.
Dr. Spencer,
Where did you source your data from? The WHO has this site that appears to contradict it …
https://experience.arcgis.com/experience/685d0ace521648f8a5beeeee1b9125cd
Thanks,
D. Holliday
To those who have pointed out that Indonesia and Malaysia have both high incidence of Malaria and Covid-19 and that fact weakens Dr Spencer’s theory – Malaria in Indonesia and Malaysia has become resistant to Chlrorquine. Therefore Chloroquine would no longer be used as a prophylactic in those areas. In my opinion the fact that Indonesia and Malaysia have both high incidence of Malaria and Covid-19 actually further supports Dr Spencer’s theory that the prophylactic user of Chloroquine for Malaria is acting as a prophylactic for Covid-19,
https://www.ncbi.nlm.nih.gov/pubmed/12114045
I was thinking that maybe guys that had Malaria might be immune to Covid-19.
@ur momisugly#%! – another theory went down the drain. 😉
In summary, we have found that patients with COVID-19 are prone to digestive symptoms and nearly half report a digestive symptom as their chief complaint. In rare instances, patient can even present with digestive symptoms in the absence of respiratory
symptoms.
Compared to COVID-19 patients without digestive symptoms, those with digestive symptoms have a longer time from onset to admission and a worse clinical outcome.
These results obligate additional research evaluating the prevalence, incidence, predictors, and outcomes of digestive symptoms in this still emerging pandemic.
https://journals.lww.com/ajg/Pages/default.aspx
Urgent Request!
I have just tried several of Anthony’s links to the studies above, and find that Google has just barred most of them. Has anyone else experienced this?
yes all links to doc.google.com.
only one runs, but it’s noct a helpfull one
Oof, yes. Click on the “new medical studies” link at the very top of the article. The error message is:
“We’re sorry. You can’t access this item because it is in violation of our Terms of Service.
Find out more about this topic at the Google Drive Help Centre.”
Other links in the article seem to work OK. Might be a technical glitch. Or perhaps an EU GDPR problem?
Here is a look at the results of a group of anti-viral drugs tested against Covid-19, … https://docs.google.com/document/d/e/2PACX-1vTi-g18ftNZUMRAj2SwRPodtscFio7bJ7GdNgbJAGbdfF67WuRJB3ZsidgpidB2eocFHAVjIL-7deJ7/pub?fbclid=IwAR3HXmAaRvsKQwtD4mT0W6NU4bTJvZnR6f3KLRcsWkXSOGn33dbdR1KyS0Q
Link does not work.
Google says it cannot be viewed.
And here is the more important update from one of the leading virologists in Germany on the subject: it helps if you know German, but the short version is that the study is unscientific BS and no conclusions can be drawn from it:
https://www.focus.de/gesundheit/news/wir-sind-kein-stueck-schlauer-top-virologe-drosten-entkraeftet-hoffnungsvolle-studie-zu-moeglichem-corona-heilmittel_id_11791311.html
Pretty much just what I have been saying.
Picked up some Sapphire Gin and lot soft tonic water (with quinine). Starting a new tradition based on the old British tradition- gin and tonic in the afternoon. Might be prophylactic, probably not harmful. Cheers mates!
taking chloroquine is not without risks – be warned
chloroquine is a safe drug if taken as directed but an overdose of 2x is deadly! It also has some pretty dire side effects:
Chloroquine
Side-effects
Rare or very rare
Cardiomyopathy; hallucination; hepatitis
Frequency not known
Abdominal pain; agranulocytosis; alopecia; anxiety; atrioventricular block; bone marrow disorders; confusion; corneal deposits; depression; diarrhoea; eye disorders; gastrointestinal disorder; headache; hearing impairment; hypoglycaemia; hypotension; insomnia; interstitial lung disease; movement disorders; myopathy; nausea; neuromyopathy; neutropenia; personality change; photosensitivity reaction; psychotic disorder; QT interval prolongation; seizure; severe cutaneous adverse reactions (SCARs); skin reactions; thrombocytopenia; tinnitus; tongue protrusion; vision disorders; vomiting
Side-effects, further information
Side-effects which occur at doses used in the prophylaxis or treatment of malaria are generally not serious.
Overdose
Chloroquine is very toxic in overdosage; overdosage is extremely hazardous and difficult to treat. Urgent advice from the National Poisons Information Service is essential. Life-threatening features include arrhythmias (which can have a very rapid onset) and convulsions (which can be intractable).
https://bnf.nice.org.uk/interaction/chloroquine-2.html
The antimalarial drug chloroquine is the most severe and frequent cause of poisoning in Africa’,2 and the Far East.3 The mortality rate in the published studies ranges between 10 and 30% and is amongst the highest in clinical toxi- c~logy.~ The high mortality rate in chloroquine poisoning is related to close dose-dependent toxicity and to rapid onset of severe cardiac symptoms.
https://onlinelibrary.wiley.com/doi/pdf/10.1111/j.1365-2044.1990.tb14629.x
And Arizona man is dead and his wife is in critical condition after taking chloroquine because they were afraid of Corona virus.
What is it that I am reading that CoQ10 helps in the prevention of catching the Covid virus, is it true or false?
Malaria had been eradicated from India for a decade and staged a comeback during year 1971. Since 1971, several avtars of fever afflicted India. Viral fever, Dengue fever, Chikungunya – all began as killers. With time we learnt how to coexist with those diseases. Corona Virus showed up during recent months. That engulfed the entire World. The world would soon learn how to coexist with Corona Virus.
Since year 1971, Chloroquine has been my default drug in fever cases. Viral fever, Dengue fever, Chikungunya – all political entities responded to Chloroquine. By simple mathemathics, there can be two possibilities :-
1. New avtars of fever during consecutive years were new variants of malaria.
2. Chloroquine known as antimalarial, may be nonspecific fever drug, effective also against Viral fever, Dengue fever, Chikungunya, and now Corona Virus.
Chloroquine is a harmless drug with single dose required in endemic population and 5 tablet (double strength) course required elsewhere.
Immunity boosters in routine and Chloroquine at first fever sign may be a magic mantra to make the World Corona free. Atovaquone-proguanil should also be tried in place of Chloroquine.
Dr K Chaudhry http://immunity.indianmedical.net
FIRST Author of Jaypee Brothers
I am just gonna leave this here:
https://www.msn.com/en-us/news/us/fearing-coronavirus-arizona-man-dies-after-taking-a-form-of-chloroquine-used-in-aquariums/ar-BB11BDzF?ocid=msedgntp
This is the same kinda idiot who would drink rubbing alcohol when out of vodka.
I do not know what kind of idiot he is.
Except that now he is a dead idiot.
Chloroquine phosphate is the same form that the Belgium paper recommends.
Well, he had to take it out of the box, which has a big red banner which says Not For Human Consumption, front and back, also has that written across the back of the plastic and foil card the tablets are in. I know, I have used it in the past maintaining aquariums for businesses and individuals in a former life. Perhaps today there are no warnings, been awhile since I did the aquarium cabana boy routine.
I saw at least one article that has the box with the warning label you mention.
It is for sure that it was extremely boneheaded.
But when people have no medical knowledge, and are more afraid than they are cautious…this is a predictable outcome for at least some number of people.
Panic and fear lead to irrational decision making.
IMO, anyone who talks about, or writes about these drugs, has a responsibility to prominently post warnings of the toxic nature of these drugs.
Brazil has been freed up Today no more madness. Viva Bolsonaro this is just a common severe flu. Positive result in Brazil with cloroquine just coming in. If there was no internet NO ONE would have differentiated this from normal flu
Hello,
I looked for studies who could help against the coronavirus SARS-COV-2 infection, and I think I might have noticed something promising, so I’m writing here my proposal for prevention of Covid-19 and possibly a treatment, to be tested:
Zinc Ascorbate proposed against Covid-19
Author: Valentino Cingolani
23/03/2020, Recanati, Italy
Version 0.3
Given that:
1. the combination of zinc ions and zinc ionophores at low concentrations inhibit the replication of SARS-COV in cell culture, via inhibition of elongation of RNA-dependent RNA polymerase and reduction of RNA template binding [1];
2. in zinc ascorbate, ascorbic acid enhances zinc absorption into cells [2];
Here I propose that zinc ascorbate supplementation could be effective in the prevention and cure of SARS-COV-2 infection and Covid-19 disease.
Zinc ascorbate supplementation is already used in diabetes and glycemic control in humans.
It is proposed that zinc ascorbate should be tested both in-vitro and in-vivo against SARS-COV-2.
Also, zinc ascorbate supplementation, given the high feasibility of a clinical trial and the potential immense benefit to people, should be tested as soon as possible, for the possibility of prevention and cure of Covid-19 disease.
[1] Zn2+ Inhibits Coronavirus and Arterivirus RNA Polymerase Activity In Vitro and Zinc Ionophores Block the Replication of These Viruses in Cell Culture – Aartjan J. W. te Velthuis 2011, PLoS Pathog https://journals.plos.org/plospathogens/article?id=10.1371/journal.ppat.1001176
[2] Zinc-chelated Vitamin C Stimulates Adipogenesis of 3T3-L1 Cells – C. Ghosh 2013, Asian-Australas J Anim Sci https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4093222/
My proposal is available at https://drive.google.com/file/d/1x0DVGz303NiFmjy8hwDoA6SGht1NNAIG/view
Thank you all for any comments and if you could help in setting up a trial.
Valentino Cingolani
Why the parenthetical reference to phosphate? I don’t see P in the chemical formula
In the interests of balance, it is worth noting the Daily Mail “exclusive” investigation that claims that Rigano is a fraud:
https://www.dailymail.co.uk/news/article-8143845/Malaria-cure-coronavirus-promoter-cryptocurrency-hustler-fake-Stanford-University-claim.html
The article fails to mention the full panoply of chloroquine studies, so it may be as much motivated by anit-Trumpism as anything.
Incredible!
We shall know much more in the future, but this is truly astounding.
Here is some more regarding the apparent huckster who seems to be at the center of at least part of this sensationalism.
As you say, it could be anti Trumpism…but this Rigano guy appears to have misrepresented himself at the very least.
He does not correct when he is referred to as a doctor…he is not.
He does not correct when referred to as an advisor to Stanford U…he is not, apparently. Stanford seems to have denied it and disavowed him.
https://www.newyorker.com/news/news-desk/donald-trumps-dangerous-messaging-about-a-possible-coronavirus-treatment
https://youtu.be/tcHeVqoLVWI
BTW…Didier Raoult seems to be a master of self promotion as well.
I was just looking at his impressive Wikipedia bio…then noticed that all of the many dozens of references used are all papers Raoult himself authored or co-authored.
Many of the claims made are astounding to say the least.
Maybe…too astounding?
IDK.
I am very curious to see how this all shakes out.
More news from France:
“French Expert: Second Study Shows Malaria Drug Helps Fight Coronavirus”
https://www.breitbart.com/news/french-expert-says-second-study-shows-malaria-drug-helps-fight-coronavirus/
But critics point out the same problems as many noted with the first set of “studies”:
“Dr Raoult, whose theory has been taken up by US President Donald Trump, said his new study of 80 patients showed that four out of five of those treated with the drug had “favourable” outcomes.
He had earlier reported that after treating 24 patients for six days with hydroxychloroquine and the antibiotic azithromycin, the virus disappeared in all but a quarter of them.
The research has not yet been peer reviewed nor formally published in a medical journal.”
“Raoult’s critics have pointed to problems with the protocol of his testing and worrying side effects of the drug.
Fakemed, a group of scientists against fake news in health, lambasted the 68-year-old professor.
After Raoult released his latest findings on the internet over the weekend, Professor Francois Balloux of University College, London, tried to dampen talk that the drug could be a silver bullet.
“No, (this is) not ‘huge’ I’m afraid,” he said on Twitter.
“This is an observational study (i.e. not controlled) following 80 patients with fairly mild symptoms. The majority of patients recover form #COVID19 infection, with or without #Hchloroquine and #Azithromycin treatment.”
Statistician Tim Morris of the university’s clinical trials unit was even more scathing.
“If hydroxychloroquine turns out to be useful,” he tweeted, “it’s a shame that this group will be praised as heroes and prophets instead of held to account for the misinformation and self-promotion they’ve been churning out at a critical time.”
Chloroquine and hydroxychloroquine, which is often sold as Plaquenil, have been hailed as a potential “gamechangers” by Trump, but US government experts are as yet unconvinced, with Dr Anthony Fauci, the head of the US National Institute of Allergy and Infectious Diseases, calling the results so far “anecdotal”.”
“Dr Philippe Gautret, who was part of the team behind Raoult’s latest findings, admitted that they only used the combination of drugs on “patients who had not been showing signs of being seriously ill after admission” to the hospital.
“Our strategy was precisely to treat them at that stage to stop the disease getting to a more serious stage,” he told AFP.
“A doctor can and must think like a doctor and not like a methodological researcher,” Raoult wrote in an article for the French Le Monde daily, defending his methods.
According to his latest study, 65 of the 80 patients treated improved and were discharged from hospital in an average of less than five days. One patient aged 74 was still in intensive care and another aged 86 died.
But his critics say such results were fairly typical of the virus.
Two Chinese studies have shown that “10 days after the start of symptoms, 90 percent of people who have a moderate form (of the disease) have a controlled viral load,” epidemiologist Dominique Costagliola, of the French health research institute Inserm, told AFP.
The fact that they got these results using hydroxychloroquine “does not make the case for its effect,” she said.”