Guest Post by Willis Eschenbach
Watts Up With That is about more than just the climate. It’s also about interesting things in the world. So if you’re looking for just climate, this isn’t the post for you. However, it’s an interesting peregrination through the world of the mathematics of illness.
We’ve been hearing a lot about “exponential growth” in relation to the cases, spread, and mortality of the Wuhan Virus. And to be sure, it is indeed a global health crisis, one we need to take very seriously.
The curious part is, “exponential growth” doesn’t actually describe the progress of a given disease. Exponential growth never stops—it just gets larger and larger, going up and up without end. But that’s not what happens with a disease.
For example, here’s what has been happening with the total number of Wuhan Virus cases in South Korea.

Figure 1. South Korean total cases of Wuhan Virus since the beginning of the epidemic. SOURCE
We see the same shape of curve regarding the total number of deaths in China.

Figure 2. Total deaths in China from the Wuhan Virus since the illness took hold. SOURCE
Now, this particular “s-shaped” curve is called a “Gompertz Curve”. It is a curious curve, in that it is not symmetrical. It goes up faster than it levels off. Here’s an example.

Figure 3. A typical Gompertz Curve, which describes the evolution of the number of total cases or the number of total deaths in an epidemic.
So I thought I’d see how well those two graphs in Figures 1 & 2 could be fit by a Gompertz Curve. First, here’s the graph of the South Korean total cases, along with the best-fit Gompertz Curve:

Figure 4. Total Wuhan Virus cases, South Korea, along with the best-fit Gompertz curve for the data.
You can see why the Gompertz Curve is used to describe epidemics—it’s a very good fit to real-world epidemiological data. And because any given Gompertz Curve ends up at some maximum value that it doesn’t exceed, it also allows us to estimate the part of the curve that hasn’t happened yet. So far, there have been some 7,362 cases in South Korea. The Gompertz Curve estimates that the final total will be on the order of some 8,100 cases or so.
Now, that’s not a hard number, of course. All kinds of things can happen to bend the curve either up or down. But it’s better than just making a blind guess.
Next, here is the same kind of look, data plus best-fit Gompertz Curve, but at the deaths in China.

Figure 5. Total Wuhan Virus deaths, China, along with the best-fit Gompertz curve for the data.
Again, with the same caveats as before, we can take an educated guess at what the total number of deaths is likely to be. By the end, the Gompertz Curve estimates about 3,500 deaths.
Finally, let’s take a look at the deaths in South Korea. It’s still early, deaths are still happening, so this will be more uncertain.
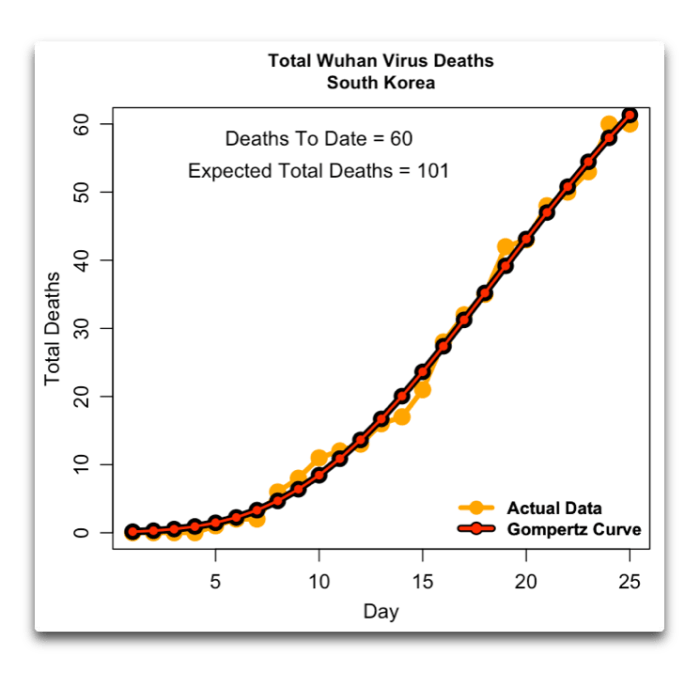
Figure 6. Total Wuhan Virus deaths, South Korea, along with the best-fit Gompertz curve for the data.
Although the uncertainty in this one is greater, it looks at present like the final total of deaths in South Korea will be on the order of one hundred, give or take.
Conclusions
On my planet at least, this is very good news. Deaths in China look like they will be on the order of 3,500 lives lost. Cases in South Korea are near to peaking. And although it’s early to do this kind of analysis on the number of deaths in South Korea, to date there have only been 60 deaths, and the best fit Gompertz Curve peaks out at a hundred deaths.
Please be clear, though, that I’m not minimizing the danger. A virus of this nature can do immense harm if we don’t stay ahead of it. What I’m saying is that China and South Korea show that we indeed can stay ahead of it.
So let me suggest that we take all precautions, wash hands, social distancing, canceling large gatherings, testing as and when required, self-quarantine, it’s very important to slow the virus down … and that we also dial way back on the hysteria and the politicization of the issue. I assure you, assigning blame to one political party or the other and buying six cases of toilet paper won’t help end the epidemic. Although I must confess, thanks to the web I finally understand the panic buying of toilet paper. I read that it’s because when one person sneezes, a hundred people soil their underpants … so don’t be one of them.
Here on my hillside, I don’t need social distancing. I’m a hermit anyhow, have been for a while now. I hate going to town, and I love my forest home. The plum trees in our entry were fooled into blossoming by the warm dry February.

But then the plum trees got surprised by the March rains. The ground underneath them looked like a local snowfall, there was not a blossom left on the limbs … we’ll see if we get any plums in the fall.
I spent the day using the weedwhacker to give a haircut to the flowers and greenery growing up through the bricks on the patio I built … perhaps I should have put down geotextile fabric, but I do like the way the plants never stop shouldering their way up through the tiny crevices. I take it as a sign of hope, that life endures no matter the obstacles.
My best to all, wash your hands, stay well in these parlous times.
w.
As Usual: I ask that when you comment you quote the exact words that you are responding to. This avoids endless misunderstandings and disagreements.
Data: All of the data is from the Worldometer site.
For Math Geeks Like Me: The Gompertz Curve is defined as
y(t) = α * exp(-β * exp(-k * t))
where
t = time alpha = upper asymptote beta = growth displacement k = growth rate
On Political Correctness: Yes, I know that the wokerati have taken up the cry that calling it the “Chinese Coronavirus” or the “Wuhan Virus” is RACIST!!!, their go-to accusation to try to discount anyone they don’t like. Consider it my small blow for freedom of speech and not bowing to political pressure. Me, I’m the least PC guy imaginable, and I was brought up in a household where racism was simply not tolerated in any form, so trying to bust me for being RACIST!! just doesn’t work. I know who I am.
And if you think that the people who are claiming that this is RACIST!!! actually believe it and it’s not just sleazy political maneuvering, consider the following two tweets, six weeks apart:

Followed by …

However, if you insist on taking that route, before you bust me for calling it the Wuhan Virus because it originated in Wuhan, please let me know your racism-free politically 100% correct alternative names for each of the following illnesses, all of which are named for their place of origination:
- Rocky Mountain Spotted Fever
- Lyme Disease
- Marburg Fever
- West Nile Virus
- Valley Fever
- Middle Eastern Respiratory Syndrome (MERS)
- Ebola Virus
- German Measles
- Lassa Fever
- Ross River Fever
- La Crosse Encephalitis
- Legionnaire’s Disease
- St. Louis Encephalitis
- Heartland Virus
- Bornholm Disease
- Junin Virus
- Nipah Virus
- Rift Valley Fever
- Zika Virus
- Norovirus
I mean, we don’t want to be RACIST!! regarding the people of St. Louis or the inhabitants of the Rocky Mountains, do we? …
Willis, although there are good news for China/South Korea, this is happening with restrictions that cannot last forever. At some point they will have to remove the restrictions. It would be silly to think that this will not have an impact on those graphics’ evolution.
This is what I foresee: 2 weeks of restrictions to level-off the curves, then the restrictions disappear and we have rapid increase of cases, then new restrictions, then new reduction in cases, then restrictions removed, then new increase in cases… etc etc. In the end we all are going to have the coronavirus at some point. The question is how much total restriction time can we stand before the economy is completely ruined everywhere and the world as-we-know-it experiences dramatic and long-lasting changes, perhaps forever. The death toll of the virus is going to look like a minor problem in comparison.
Things will ramp up slowly, especially in the travel industry. It might be a good idea for the U.S. to purchase a couple of cruise ships for conversion to floating hospitals for future emergencies.
This virus has exposed numerous system weaknesses that hopefully we will address but it’s human nature to prepare for the previous battle.
I went to a nearby Walmart this morning and water, toilet paper and vitamin C were among the items sold out. The fresh fruit and vegetables looked fully stocked as did refrigerated orange juice and lemonade shelves. Most of the milk section was empty but there was still some remaining.
The hoarding will level off. There is no shortage of food and supplies and the store shelves will be restocked quickly and this will calm the fears of the public over the coming days.
New active ingredient from Lübeck is said to help against coronavirus
by Linda Ebener
They worked on him day and night, and soon they will be presenting their development to the scientific world in the renowned scientific journal “Science”: a team of researchers led by Professor Rolf Hilgenfeld from the University of Lübeck has developed an active ingredient that is supposed to help against the novel corona virus. This is responsible for the current Covid 19 pandemic. The drug has already been tested in the laboratory in human lung cells that are infected with the new virus. The active ingredient is active, says Hilgenfeld. That means he helps. Hilgenfeld and his co-workers Xinyuanyuan Sun and Linlin Zhang’s approach: The active ingredient is said to render the viruses in the lungs harmless. Because the corona primarily attacks the lungs.
https://www.ndr.de/nachrichten/schleswig-holstein/Der-Wirkstoff-gegen-das-Coronavirus-kommt-aus-Luebeck,corona666.html
Wow, the active ingredient is active. In fact it is really active, the active ingredient, that is.
The link says nothing really, and the video in the link did not play.
The video finally loads, it’s still not informative.
Er rechnet in diesem Fall allerdings damit, dass es schneller gehen könnte, “wobei das erstmal auch nur Spekulationen sind”, so Professor Hilgenfeld.
There is years of testing for most drugs between placing in cell cultures and approval for usage given.
A tiny percentage of drugs that work when you place them in a cell culture will be safe and effective when someone puts a pill in their mouth.
The human body is not a petri dish of cells.
Typo…a tiny percentage…
Sorry.
Fixed … I hate typos.
w.
Thank you sir.
You do a great job Willis.
If you have ever followed biotech companies or the process for getting a new drug from the lab to approval, you would know one in about 5000 drugs that work great in cell cultures is ever approved for use in humans, and the process takes on average 12 years, and costs about $3 billion.
Some sources list a far lower cost, and other ratios, like only a few hundred million dollars, or that as many as one in 1000 are approved.
But an overview of the literature on this gives a centered average value for these numbers at 12 years, 3 billion dollars, and one in 5000 drugs, from lab bench to doctors being able to prescribe.
https://www.medicinenet.com/script/main/art.asp?articlekey=9877
https://www.policymed.com/2014/12/a-tough-road-cost-to-develop-one-new-drug-is-26-billion-approval-rate-for-drugs-entering-clinical-de.html
https://www.drugs.com/fda-approval-process.html
Willis,
Your analysis is interesting, but I fear your conclusions may be overly optimistic.
The reason is that both China and South Korea are under a phase of intense disease control. Large areas of China are in lock-down, while South Korea has massive amounts of testing. This has two implications:
Firstly, in those countries, as the controls are relaxed, there is likly to be a second wave of infection. Spanish flu had at least three major waves of infection and deaths through 1918 and 1919.
Secondly, it is hard to see how such controls can work in US. Countries like France and Belgium have closed all shops, restaurants, cafes, theatres etc and are beginning to restrict local travel. Could that happen in US and would the public put up with it?
Chinese factories began coming back on line a couple of weeks ago and reports are they’re at over 50% capacity now. All of the temporary hospitals in Wuhan have been closed, so things are improving there. We need to learn all that we can to benefit from China’s experiences, including recovery.
For now, there is at least some reason to be optimistic. We ought to know within a week if China’s recovery is just false hope or not.
It’s already happened here, see
https://www.lohud.com/story/news/politics/2020/03/16/ny-nj-and-connecticut-shutter-all-casinos-gyms-8-p-m-monday/5057995002/
Also in NJ we have a curfew from 8pm to 5am.
Dear Willis,
This is an interesting article:
Why outbreaks like coronavirus spread exponentially, and how to “flatten the curve”
https://www.washingtonpost.com/graphics/2020/world/corona-simulator/
Different scenarios, shown visually too.
“Even with different results, moderate social distancing will usually outperform the attempted quarantine, and extensive social distancing usually works best of all. Below is a comparison of your results.”
You might want to take a look at it.
Best regards,
Scarface
Nice animations.
Willis,
I think you made an error in the expression of the Gompertz curve: the last exponent should be -k*t (a product) and not -k^t (which would mean k at the power of t). So the correct function is:
y(t)= a*exp(-b*(exp(-k*t))
Thanks, Francis. I think what I wrote is right. See Wolfram’s MathWorld on the subject.
w.
Willis,
At the link you gave, I see the function arranged quite differently.
But please see also here, which would support Francis MASSEN’s point.
https://demonstrations.wolfram.com/TheGompertzSigmoidFunctionAndItsDerivative/
I appreciate your interesting post.
Further research shows that you and Francis are right. It’s
alpha * exp(-beta * exp(-k * t))
I’ll correct the head post.
w.
Thanks for the correction. I was trying to get it all to plot out on Excel. This explains it.
Francis MASSEN,
I would have to agree with you, based on what I found here.
https://en.wikipedia.org/wiki/Gompertz_function#Gompertz_Curve
Under the “formula” heading at this Wikipedia page, I can’t copy and paste it here. But the stated formula there could be written out here in the form f(t)=a*exp(-b*exp(-c*t)), which corresponds to what you wrote.
There are more than a few comments on here about H1N1 that do not agree with the data on the CDC web site – here is the real data https://www.cdc.gov/flu/pandemic-resources/2009-h1n1-pandemic.html
Keep in mind that H1H1 was a virus that could be treated by existing antiviral agents. This was NOT the case with COVID19 during the first month or so. The Anti Viral agents pulled out of the CDC Cure Locker did not work! This was not the fault of CDC. There is no way the CDC can have a “Cure” already designed in their Cure Locker. AND there is no way that the CDC could develop a Cure in 30 days.
Further, look into CFR 42 – Public Health. The past administration ruled by REGULATIONS. Numerous regulations were added the majority of the CFR regulations. Millions of pages and hundreds of thousands of new regulations. These regulations restricted the access, use and distribution of the new tests that everyone blames Trump for delaying. It took time to change these regulations IAW the law/rules. He could not wave a wand and make them disappear, destroying the myth that Trump is an Authoritarian. If he was he could have done like past presidents.
All Virus’a are NOT equal – That is why the Common Cold is still around. There are millions of the viruses that cause the Common cold and they are constantly changing,
Your website says so, InfoWars and Natural News say otherwise. Either way, “data” (stuff on a website) isn’t evidence. It isn’t science. It’s propaganda.
The CDC website might rate as being slightly more credible than Alex Jones, but not by much. Either way, I don’t see why either (Jones or the CDC) should get subsidies.
Which is why no one pays any attention to you, of values your opinion on anything whatsoever.
You do not see why anyone should find the CDC more credible than Alex Jones, but think your own opinions count for anything at all?
How can you even pay attention to yourself, when all you have is guiding you is the horse sense of an uneducated low IQ internet troll?
You failed to provide any evidence that any of your fetish vaccine has any benefit in the US.
I have humiliated you.
niceguy March 16, 2020 at 8:45 am
Are you blind? Why do you think that there is no polio in the US, when there used to be 35,000 cases per year and even the President got it? People were terrified of it when I was a kid, and they no longer are.
Why do you think that there’s no longer polio in the US? Good thoughts? Anti-vaxxers killed the polio viruses with fly swatters? What’s your theory about the disappearance of a virulent disease?
Bad news on that front … if you want to know who’s “humiliated” by your claims, grab a mirror …
w.
“there used to be 35,000 cases per year”
Cases of WHAT?
How many were tested, like for coronavirus?
“Why do you think that there’s no longer polio in the US?”
Answer your own question, NPC.
Pass. I can’t deal with that level of stupid. “Cases of WHAT” he asks … cases of Corona Beer, I guess.
My best to all the rest of you,
w.
Some of the commenters here seem very knowledgeable in matters of epidemiology, so maybe some of you can weigh in on the Diamond Princess.
The Diamond Princess was the cruise ship that was quarantined off the coast of Japan after a COVID-19 outbreak on board. Of the 3,700 or so passengers on board, 705 contracted the virus. Of these, six eventually died, giving a death rate of under 1 percent. In keeping with what we’ve come to expect, none of those deaths were among people under 70. My understanding is that all, or very nearly all, of the passengers were tested. From an epidemiological standpoint, could you even ask for a better natural laboratory in which to observe the effects of this illness?
So how is it that of 3,700 people packed into a veritable petri dish, only 17 percent ever contracted the virus at all? Could it be that this thing simply isn’t as contagious as many believe?
How much time were these people NOT in lock down?
During that time, how many were contagious?
I can understand the run on toilet paper. It takes a lot of TP to wipe the fecal matter from these idiots brain cavity.
I fully agree with Willis. I’ve been keeping a very, very close watch on the numbers for the simple reason that my bride of 48 years is in a Rehab facility (same company as the Kirkland Washington facility) for a broken leg. She has COPD, and being older, she is in the high risk category. Her facility is taking a lot of sensible precautions, including excluding all visitors. This latter precaution puts a serious pinch on the two of us and limits my ability to learn from the occupational/physical therapists the tricks for taking care of her for the next two months until she is out of her leg brace. Having some medical background, I’ve been very helpful to the staff in tending to her needs while in the facility; that help is now gone. As super frustrating as this is, I fully agree with the common sense precautions. Despite few interactions with the public, such as shopping, I dare not bring in a bug that I’ve been exposed to. It could be fatal. I worry just as much, if not more, about all the other cold and flu bugs.
When you look carefully at the numbers there is only one major category of risk – the aged with lung and or immune compromised systems. The public panic over this virus is insane.
Willis, thanks for posting this piece. Anything that helps to tamp down panic over the virus is a help for those of us who really need assistance. God speed.
There are some fascinating simulations of disease spread here.
w.
Haha, a good time to locate another graph-digitiser and so I have just tried the online WebPlotDigitizer
https://automeris.io/WebPlotDigitizer/
-Not bad 🙂
It seems that both the China death rates and the South Korea cases are slightly better fitted by a logistic curve than the Gompertz.
(Using the PAST program – model-non-linear fit)
If anyone is interested in real forecasts there is a spreadsheet on my website:
https://scottishsceptic.uk/2020/03/11/coronavirus-forecast-model/
Fortunately, there is a way to beat CV19:those under 50 represent only 10% of the loading on the healthcare system, so it is possible to get the economy over the worst of the epidemic by allowing or even encouraging those under 50 to get infected whilst delaying and controlling the rate of infection of those over 50. That allows the majority of workers (70%) to continue as before and controls demand on healthcare. Fortunately, a variant of this appears to be the strategy being adopted by the UK.
I haven’t a clue what the US is doing – but god help you if you think it’s going to peak at the Chinese level without major intervention by government.
Excellent observation. The UK government are getting it right and mustn’t be deflected by all the noises off. If extreme measures are used now to close it down it will only come back when the extreme measures are removed.
Which is excellent…this one?
“allowing or even encouraging those under 50 to get infected whilst delaying and controlling the rate of infection of those over 50.”
I would love to hear the excellent plan for making this simple sounding plan a reality?
Do you guys live somewhere that people are segregated by age group, and the under 50 can be kept away from the over 50 for a few months?
How many doctors are over 50?
Police?
Pharmacists?
Business owners?
Do these age groups live separately where you are?
What the hell are you talking about anyway?
I followed your model for the U.S. that you left here on Monday. It was close on day 1, but by day 4 it over predicted deaths and cases by about 100%.
And how do we let people under 50 get it as quickly as possible, and preventing them spreading it, when those people live with, care for, and attend to the needs of the older people that we will somehow simultaneously protect?
If you cannot articulate exactly and specifically how you think that can happen, you are just talking out of both sides of your mouth.
“What could possibly go wrong?” How many film script writers did it take to come up with that idea?
Mystery Solved! It is not Corona-gate!
Why are few children dying?
Why is there an increase in the number of old people dying when most populations are experiencing an increase in their elderly as the post-war baby boomer age?
Why is an area in China currently experiencing an economic reversal due to US trade tariffs and the stall of an economy feeding off the collapse of Western civilization, suffering health problems?
Have medical staff other than those who were removed for discussing the outbreak in Wuhan die?
Why when you rush out and decide to measure a finite quantity in your community would you not expect to get these types of curves that flatten out with time?
Why when you decide to assign deaths to a particular commonly occurring virus do these deaths increase then slow as the population exits the normal winter elevation of deaths of the elderly or compromised?
It is not Corona-gate, it is simply linking the sudden increased testing of a common cold virus after a bitter Northern winter, to the natural collapse of the socialist health systems dealing with an aging population bubble entering the death zone.
Happy for an explanation that I am wrong. Please include an explanation why children aren’t dying in proportion to their occurrence with the elderly.
From the statistics I’ve seen for the USA:
First column is date,
Second column = total COVID-19 cases to date
Third column = total COVID-19 deaths to date
Fourth column = New COVID-19 cases in day
Fifth column = New COVID-19 deaths in day
Last column = % of new cases dying in day
2/29 68 1
3/01 75 1 7 0 0.0%
3/02 100 6 25 5 20.0%
3/03 124 9 24 3 12.5%
3/04 158 11 34 2 5.9%
3/05 221 12 63 1 1.6%
3/06 319 15 98 3 3.2%
3/07 435 19 116 4 3.4%
3/08 541 22 106 3 2.8%
3/09 704 26 163 4 2.5%
3/10 994 30 290 4 1.4%
3/11 1301 38 307 8 2.6%
3/12 1697 41 396 3 0.8%
3/13 2247 49 550 8 1.5%
3/14 2943 57 696 8 1.1%
3/15 3668 68 725 11 1.5%
From the numbers for new cases so far, it seems like the disease is still spreading exponentially (the number of new cases per day continues to increase, for now). The number of new cases could further increase in the near future, since the availability of more test kits will mean more people tested, and possibly more positive diagnoses of people with mild symptoms who otherwise might not have been tested.
However, the last column, or percentage of new diagnoses who died, is decreasing–over the last six days, the average death rate was 1.3%, and it has been under 2.0% the last four days and five out of the last six days. Granted, there is a lag time between diagnosis and death, but there could be a lot of undiagnosed carriers (showing no symptoms or mild symptoms) out there, who haven’t been included in the denominator, but a death count is probably much more accurate, so that the eventual death rate may actually be much less than the 1.3% in the last six days.
Still, 3,668 positive diagnoses represent only about 0.0011% (11 ppm) of the American population, most of whom are concentrated in three states (CA, WA, and NY) so it is still possible to contain the virus. What is needed is to test more people who may have been exposed to known cases, and those showing symptoms, and ask all those testing positive to isolate themselves until healed or hospitalized.
However, it may not be possible to fit a Gompertz curve to the USA data, because we have not yet reached the inflection point of the curve, where the number of new cases per day starts decreasing.
Just did a quick curve fit of the US data from Feb 15th to Mar 16th and the assymptote (alpha) is 642,000!
Granted it is a very limited data set and it has not hit either “knee” in the curve…
Cliff Mass linked this map from the NY Times.
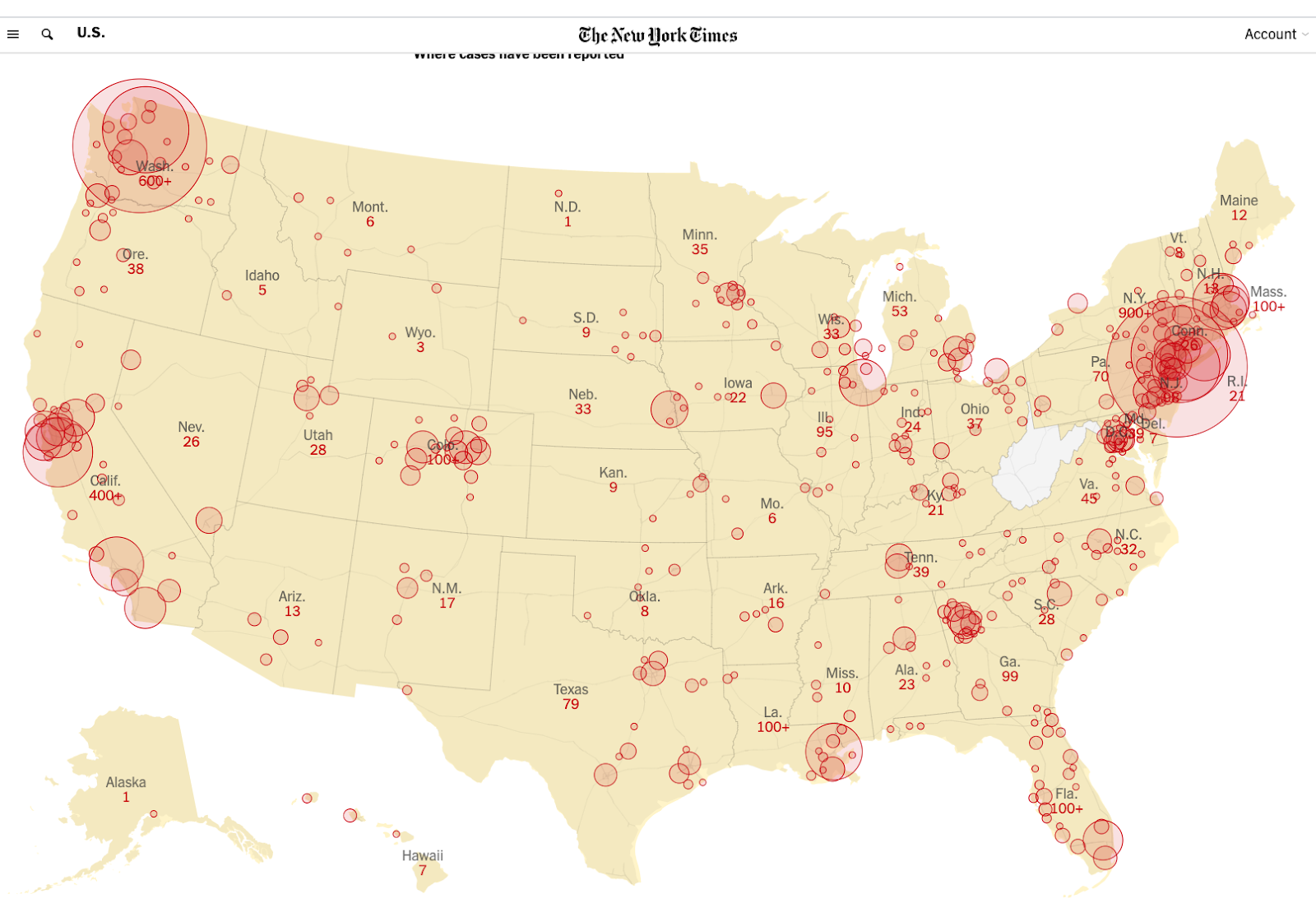
Looking at this, my H0 is “R0 is higher in denser populations”, which seems obvious. Of course, the big cities will have more outsiders coming in who could be infected. But looking at the map, fly-over country has it too, and one case may be enough to start the contagion.
Everybody has their circles of family, friends, and associates, the first potential victims of R0. Those circles overlap with other circles. And then there are all the people who are not in those circles whom you have fleeting contact with in stores, mass transit, airports, hospitals, bread lines, whatever, and all those people have their own circles.
In the big cities, some of those fleeting contacts could be massive. Bigger crowds in stores and subways.
Higher R0 means it spreads faster and less chance of it dying out.
For the voyeurs, Johns Hopkins will give you gory details:
https://coronavirus.jhu.edu/map.html?mod=article_inline&modtag=djemBestOfTheWeb
Mainland China new cases have leveled off since early Feb.
Germany has more confirmed cases than SouthKorea. That ain’t due to more testing. Are you paying attention, Angela?
The Diamond Princess has had 3 deaths, 325 recovered.
There’s one case in Greenland and 3 in Alaska, 10 in Hawaii. Hmm. It’s a hard rain a-gonna faaaallll?
BTW – no cases in Antarctica, so I guess isolation works.
and
This really sucks:
https://nypost.com/2020/03/17/diamond-princess-cruise-ship-passenger-tests-positive-for-coronavirus-a-second-time/
A Japanese man who recovered after testing positive for coronavirus aboard the quarantined Diamond Princess cruise ship caught the bug a second time at home, according to a new report. The man, in his 70s, first tested positive for COVID-19 Feb. 14 while on board the vessel off the coast of Yokohama, Japanese news agency NHK reported.
He was confirmed negative for the bug on March 2, and was allowed to take public transportation home from the Tokyo medical facility where he was staying, to western Japan’s Mie prefecture, according to the report. But it wasn’t long before he started to feel sick again, and developed a fever of about 102 degrees on Thursday, according to the report. He went to the hospital Friday, and was confirmed to be infected again on Saturday.
Well, so much for the British notion that the elderly should be confined while the young exposed themselves to infection and developed immunity, after which the elders could be released from confinement. Here’s Britain’s belated response to the epidemic.
https://www.blabber.buzz/conservative-news/809039-uk-on-second-thought-our-coronavirus-strategy-could-kill-250000-people-special
This is from Italy: https://youtu.be/o_cImRzKXOs
After 1368 Boccacio wrote his Decameron. 600 years later, Poe wrote The Masque of the Red Death. So… it could be worse. And has been.
The Decameron ends well, if indecisively. Poe’s Masque of the Red Death can be thought of as the obverse of that, and it mocks human thoughts, perceptions, aspirations, calculations, and actions.
We can be pleased that the current menace is so minimally lethal, for the youngsters, despite being rather aggressive in its spread. We fogies may think of ourselves as martyrs to youth. And hope that some lessons are learned.
Here’s the Decameron
https://blindhypnosis.com/the-decameron-pdf-giovanni-boccaccio.html
and here’s the Poe
https://www.poemuseum.org/the-masque-of-the-red-death
and then there’s C.S. Lewis in 1948 reflecting on the atomic bomb panics. For atomic bomb, read: coronavirus:
[[This does not and should not impair all proper and effective means of slowing down the progress of the virus. In all fairness, we must point out that atomic warfare is to some extent volitional. Covid19 is not. But carrying-on, as the Brits did in WWII, is indeed an admirable attitude.]]
In one way we think a great deal too much of the atomic bomb. “How are we to live in an atomic age?” I am tempted to reply: “Why, as you would have lived in the sixteenth century when the plague visited London almost every year, or as you would have lived in a Viking age when raiders from Scandinavia might land and cut your throat any night; or indeed, as you are already living in an age of cancer, an age of syphilis, an age of paralysis, an age of air raids, an age of railway accidents, an age of motor accidents.”
In other words, do not let us begin by exaggerating the novelty of our situation. Believe me, dear sir or madam, you and all whom you love were already sentenced to death before the atomic bomb was invented: and quite a high percentage of us were going to die in unpleasant ways. We had, indeed, one very great advantage over our ancestors—anesthetics; but we have that still. It is perfectly ridiculous to go about whimpering and drawing long faces because the scientists have added one more chance of painful and premature death to a world which already bristled with such chances and in which death itself was not a chance at all, but a certainty.
This is the first point to be made: and the first action to be taken is to pull ourselves together. If we are all going to be destroyed by an atomic bomb, let that bomb when it comes find us doing sensible and human things—praying, working, teaching, reading, listening to music, bathing the children, playing tennis, chatting to our friends over a pint and a game of darts—not huddled together like frightened sheep and thinking about bombs. They may break our bodies (a microbe can do that) but they need not dominate our minds.
“On Living in an Atomic Age” (1948) in Present Concerns: Journalistic Essays
—and in Iran
https://www.theguardian.com/world/2020/mar/12/coronavirus-iran-mass-graves-qom
On 24 February, at the time the trenches were being dug, a legislator from Qom, 75 miles (120 km) south of Tehran, accused the health ministry of lying about the scale of the outbreak, saying there had already been 50 deaths in the city, at a time when the ministry was claiming only 12 people had died from the virus nationwide.
The deputy health minister, Iraj Harirchi, held a press conference to “categorically deny” the allegations, but he was clearly sweating and coughing as he did so. The next day, Harirchi confirmed that he had tested positive for the Covid-19 virus. There is a recent tweet, not confirmed or denied, that Harirchi has died.
And the NYTimes, bless its heart, has a good video of what was – and wasn’t – done inside Iran –
https://www.nytimes.com/video/world/middleeast/100000007011860/iran-coronavirus-outbreak.html
I’ll refrain from saying that it couldn’t happen to a nicer country, insh’allah.
and in Jordan…Ahmad Al-Shahrouri is a Jordanian Islamic scholar. On his show on Yarmouk TV, a Jordanian TV channel associated with the Muslim Brotherhood, he said “the Jews are more dangerous than AIDS, coronavirus, cholera, and all the diseases of this world.”
and a Good Summary:
https://news.yahoo.com/burial-pits-irans-coronavirus-outbreak-172036490.html
6 minutes. Not much new, but well presented, without froth. And incidentally answers the question Why don’t we have enough test kits.
Our response actually measures rather well compared to other countries.
Another discussion is by Dr Fauci on the Morning Joe show.
March 13: Dr Anthony Fauci, on MSNBC, compliments the Trump administration for its pre-emptive travel bans on China and Europe, explains that test kits must be manufactured before they can be distributed.
https://twitter.com/i/status/1238460647823872000
and
—Trump is being blamed, astonishingly, for the US not having enough test kits to determine the actual numbers of those infected.
1. But he doesn’t control the manufacturing facilities. Nor does the CDC. Many of them are very likely overseas.
2. The kits don’t provide any treatment. They might provide reassurance so long as you don’t wonder about false negatives. No measurable short term benefit.
3. The progress of the disease does not depend in any way on the presence of test kits.
4. And while it may be a year for a vaccine, there is hope for effective treatment:
“Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Since these compounds have been used in human patients with a safety track record and shown to be effective against various ailments, we suggest that they should be assessed in human patients suffering from the novel coronavirus disease.”
—Manli Wang, Ruiyuan Cao, Leike Zhang, Xinglou Yang, Jia Liu, Mingyue Xu, Zhengli Shi, Zhihong Hu, Wu Zhong & Gengfu Xiao
Hunker down, chaps.
“Kung Flu” is less prejudicial than “The Mozelm disease”. Can we close our borders to The Corona family Virii. Unlike them, the Sumerian “Allil” allah is resolute in its malevolence.
“Islam is as dangerous in a man as rabies in a dog.”
Can we close our borders to an RNA coded virus… to paraphrase obama, ‘oh yes we can’.
Is coronavirus hype, created by virologists, modelers, and public health do-gooders? Maybe, according to this German doctor
there is this response to questions we all want answers to…
COVID-19: quelle est la réalité du terrain? Témoignage du Dr Benjamnin Davido, médecin infectiologue referent 16 Mar 20
>>When we had only 40 cases in France, we relied on level 1 Health Referral Centres (établissements de santé de référence; HRCs), such as Bichat or Pitié-Salpêtrière hospitals in Paris, to absorb the flow of patients. Now we have more than 3000 infected individuals, it is obvious that the dozen level 1 HRCs across the country are no longer enough. Consequently, second line centres, like our hospital, are taking their turn, just in time.
We have had to adapt and put in place dedicated COVID-19 units. We have, as of today [13th March] a total of 11 beds, with a planned increase to 20 beds next week. _Centres no longer have the time nor the space to receive and respond to the demand for screening._ Fifteen days ago, the screening of suspected patients had to be done in the hospital with containment measures. Today, it is no longer possible as these places are taken by confirmed cases. Screening is therefore performed in the emergency department. This is stage 3 crisis management, although this has not yet been officially announced, which underlines the pressure from the flow of patients arriving in hospitals.
Some hospitals have installed tents for urgent services, but you still need to have the capacity, to have the space and enough caregivers. And these _tents only allow outpatient diagnoses, they don’t allow for patients considered fragile or severe cases requiring hospitalization in a dedicated isolation facility._
Is France heading for a situation like Italy?
It is certain that the curves of the Italian and French epidemics can be superimposed; they are just separated in time by around 10 days. One difference between the two countries is that Italy has a particular set-up in which healthcare is organised separately by region, which may have led to a delay in the organisation of care.
Today, in France, we no longer talk of zones or foci of COVID-19, and we no longer take into account travel. On the contrary, we consider the severity of the illness, and it is the presence of unexplained pneumonia that makes us suspect a COVID-19 diagnosis, especially if it is serious straight away (in resuscitation, for example).
But as we no longer include history of travel, and the relevant symptoms are flu-like, such as having a fever, a runny nose, or coughing, and that, chronologically, it is the peak of the flu epidemic, we have an enormous influx of patients who may have flu or seasonal viral infection (mainly rhinovirus). These are consistent with the new coronavirus and, as such, we cannot, for benign cases, make a clinical distinction between them. _It becomes therefore impossible to screen everyone. In any case, we don’t have enough kits. We are at the stage of counting the number of cotton swabs to take samples…_
Did France act too late to prevent shortages?
Yes. Personally, for 10 days, I and my colleagues have struggled with the healthcare teams to urgently set up a hospitalization and screening structure to make the diagnoses, as some seemed doubtful due to the lack of anticipation by our local bodies. I don’t blame them, because bodies at the ministerial level have not given us the funds for taking the samples, as the laboratories themselves do not yet have the testing machines.
On the other hand, what should have been anticipated is the current situation where we find ourselves with questions over the supply of masks. There are general practitioners who cannot see patients in their office due to a lack of surgical masks (FFP2s _(masks only have demonstrated effectiveness in resuscitation and when obtaining the sample)_, while we are in a period of seasonal flu and colds…and coronavirus. There is also a lack of hydroalcoholic gels. For lack of a better option, it is necessary to rely on hand-washing, which is a backwards step in terms of hygiene practices. That’s why, there should be, from tomorrow, a national plan that fits with the pandemic, as declared by the WHO. Care, as set out in the current plan, is not tenable in the long-term because _in the short-term we will no longer have the capacity to accept and regulate the flow of hospitalized patients, or even to screen them._ If the epidemic lasts for 3 months, I think it will be very difficult.
Hospitals in France have been in crisis for years; in January, healthcare professionals protested against the lack of healthcare personnel and to explain that the austerity policy, which would see hospital beds close and push outpatient care, was not viable. Today, we are reopening hospital beds and requisitioning them to hospitalise suspected coronavirus patients. This morning, the regional health agencies asked us to cancel all scheduled non-urgent hospital admissions.
Doctors in Italy have had to make difficult ethical choices due to the lack of equipment (respirators, beds, etc). Will this happen in France?
We have discussed it among infectious disease specialists, and we think that it’s a question which will sadly arise when we have no more room for resuscitation, which is currently not the case. But COVID-19 patients with severe disease stay in hospital for a long time (around 3 to 6 weeks) so if the epidemic lasts, it may indeed happen. But this decision algorithm is sadly not rare in medicine. We decide not to resuscitate a patient when we know it will not save them. What is new is that this is a kind of illness for which we are not used to taking this type of decision.
[[Military doctors are familiar with the process of triage, which means dealing incoming patients into three sorts: those for whom nothing can be done; those for whom nothing need be done urgently; and those who need urgent care with a prospect of benefit. MASH never really went into that, but they should have when the children weren’t watching.]]
…
Currently, a third of hospitalized patients in resuscitation in France don’t have risk factors, including some under 40 years of age. We don’t know why yet. >>
Then he adds: _”Contaminated caregivers have been probably, in the main, in the community or hadn’t take sufficient precautions at the start of the epidemic by not wearing a mask when the patient had signs consistent with the illness (especially cough). Personally, I think I have more risk of catching the virus on public transport than in the hospital.”_
But a mask will to some degree protect the contacts, not the person wearing the mask. And there are more sick people in the hospital than on the Metro.
https://www.medscape.com/viewarticle/926883?src=wnl_tp10f_200319_mscpedit&uac=26081DN&impID=2317362#vp_4
Makes us – and Trump – look pretty good…among the humans.
On nomenclature:
ABC News, MSNBC, and PBS reporters, and many thereafter, have vilified those who refer to covid19 as the Wuhan virus or even as Chinese in origin.
“it’s nakedly racist and obviously racist and blatantly racist.”
https://spectator.org/abcs-cecilia-vega-and-pbss-yamiche-alcindor-play-the-race-card/
They don’t seem to object to some of the other designated diseases:
Middle East respiratory syndrome -MERS
West Nile Virus
Zika virus
Lassa Fever
Venezuelan equine encephalitis
Venezuelan hemorrhagic fever
Rift Valley fever
Guinea Worm — now, that’s doubly bad, impugning not only Africans but Italians.
German Measles
Marburg Fever virus
Omsk Hemorrhagic Fever
Ross River Virus
Spanish Flu
Bolivian hemorrhagic fever
Argentine hemorrhagic fever
Crimean-Congo hemorrhagic fever
Colorado tick fever
Asian Flu
Kawasaki disease
Ebola
and, lest we feel left out –
Rocky Mountain Spotted Fever
La Crosse Encephalitis
St. Louis Encephalitis
and of course Lyme Disease, named after a town in Connecticut that is 98%white, plus the obvious fact that lime is white.
I guess they have a point. Or maybe they’re just nakedly stupid and obviously stupid and blatantly stupid. No wonder the Chinese kicked them out of the country.
But I rather like calling it the Kung Flu.