Key Words: hydroxychloroquine, azithromycin, antiviral, evidence
Abstract
During the current COVID-19 epidemic, most of the evidence is collected by treating physicians, most of whom do not report their results in peer reviewed journals. Hence, there appears to be an especially broad gap between field experience and academic coverage of hydroxychloroquine-based COVID-19 treatments. The objective of this study is to bring field evidence into the academic literature.
Four relevant, non-academic surveys of physicians, in the US and globally, have been identified and checked for quality, statistical significance, coverage, and conflicts of interest. To avoid uninformed and unduly influenced opinions, only surveys conducted from April 4 to April 19 have been considered. These surveys were answered by thousands of physicians, who treated tens of thousands of COVID-19 patients.
The results: 85% of doctors said that hydroxychloroquine is at least somewhat effective for COVID-19. Hydroxychloroquine was the most utilized treatment for COVID-19 patients. 35%-40% of the doctors using the drug called it very effective or extremely effective against COVID-19. 65% of doctors said they would prescribe hydroxychloroquine for COVID-19 to their family members.
The author declares no competing interest.
No funding was provided for this work.
All relevant ethical guidelines have been followed.
Introduction
The largest body of knowledge of COVID-19 treatments is collected by practicing physicians, outside of research settings, and not reported in peer reviewed publications. The objective of this systematic review is to capture some of this clinical experience and bring it into the academic literature. The scope is limited to hydroxychloroquine-based treatments, administered in the early (viral) stages of COVID-19.
The most effective and popular COVID-19 treatment regimen, combining hydroxychloroquine with azithromycin, was introduced by Institut Hospitalo-Universitaire (IHU) Méditerranée Infection, directed by Didier Raoult. The HCQ based treatment was presented at a March 16, 2020 conference (Raoult, 2020), and published a few days later as (Gautret, et al., 2020). It became instantly popular among physicians on March 20-21.
Many doctors and hospitals used this treatment from March 20 to March 27. The treatment’s effects were observed and discussed with colleagues, from March 27 to April 4. Thus, starting around April 4, doctors who used or observed the use of any HCQ-based treatment were able to provide eyewitness testimonies. Many other doctors were able to give their expert opinions, based on the experiences of their colleagues and their professional knowledge. On April 20, the NIH COVID-19 Panel published guidelines that were adverse to HCQ treatment (The National Institutes of Health COVID-19 Treatment Guidelines Panel , 2020). On April 24, the FDA issued a warning (The FDA, 2020) concerning the drug’s safety. These events might have prejudiced some doctors against HCQ. The time frame chosen for this systematic review, April 4 to April 19, is selected to ensure that physicians had sufficient experience with HCQ but had not yet been prejudiced by external events.
Explanation of Methods
A physician’s answers to questions regarding the treatment s/he has used can be considered direct evidence. Corresponding statistics computed from the responses of N physicians, treating on average M patients, should have equal power and higher resilience than results of a randomized clinical trial conducted on N*M patients, in the absence of a systematic bias.
A physician’s choice of a certain treatment over another, indicates that the chosen treatment is considered more effective. A physician’s decision to implement a certain treatment rather than no treatment proves that the treatment’s effectiveness/risk profile is considered high enough. This can be considered indirect evidence.
A physician’s opinion about a treatment which he or she did not directly use in practice, but learned about from other physicians, can be considered an expert opinion.
Well implemented surveys can capture much of this evidence and expert opinions.
Methods
Surveys or polls of physicians were sought, using multiple search engines (DuckDuckGo, Bing, Google, Yandex), searching for ‘physician survey hydroxychloroquine’, ‘doctors survey hydroxychloroquine’, and similar combinations of keywords; no quotes; not limited by dates. The search was repeated many times, excluding previously found items.
Surveys or polls from three companies were found. Each of the three survey companies were researched and confirmed as reputable. A list of all relevant surveys and polls, done by these three companies, in the selected time frame, was compiled. This yielded four surveys from three different companies: Sermo (two surveys), InCrowd, and Jackson Coker. Sermo’s surveys appeared to be most professional and informative. No strong competing interests, that may have any bearing on the surveys, were found in any of the three companies.
Drugs used for other effects, other than antiviral, have been excluded from this review for the following reasons. High dose steroids are used during a cytokine storm. Acetaminophen, Ibuprofen, and Herbal remedies are used as symptomatic treatment. Vitamin D is not considered an antiviral treatment or an essential part of one. Bronchodilators are bronchodilators.
Results
Although the surveys posed different questions to different audiences, the results were congruent. Because CQ is hardly used in practice, CQ and HCQ are both referred to as HCQ.
Table 1. Summary of results
| J C | Sermo W3 | Sermo W4 | InCrowd | |
| Polling Date | April 4-7 | April 6-9 | April 13-15 | April 14-15 |
| Publication Date | April 8 | April 15 | April 23 | April 21 |
| Location | USA | Global | Global | USA |
| # doctors | 1271 | 4016 | 5500 | 203 |
| Recommended HCQ | 65% (1) | n/a | n/a | n/a |
| # COVID-19 treaters | n/a | 1337 | 1376 (3) | 203 |
| Used HCQ / HCQ+AZ | n/a | 50% | 53% | n/a |
| % HCQ users rating VEE (4) | n/a | 40% | 35% | n/a |
| Reported HCQ effective | n/a | 85% (5) | n/a | n/a |
| Would give to patients’ % | n/a | n/a | n/a | 30% (2) |
| Remarks | HCQ shortages |
- Would give HCQ to their family
- Would prescribe HCQ / HCQ+AZ to this percentage of their COVID-19 patients, on average. 30% is quite a high number, because most COVID-19 patients probably need no treatment, especially the patients of the surveyed physicians, about a third of whom are pediatricians. The numbers for plasma and Remdesivir are 21% and 16%, respectively.
- This number includes physicians who used HCQ in outpatient and hospital ex/ICU settings.
- VEE = Very or Extremely Effective (4 or 5 on the scale 0 – 5)
- 2 or higher on the scale 0 – 5
Notice that except for Jackson Coker, surveys’ results were published about a week after they had been conducted, so their results could not influence each other.
Sermo Week 3
(Sermo W3, 2020)
Survey Period: April 6-9
Published on April 15
Country: Global
N = 4016 – the total number of physicians surveyed, including those who have not treated COVID-19
Effectiveness:
The top treatments used or seen to be used by physicians and reported as very or extremely effective among COVID-19 treaters include:
Table 2. VEE Treatments
Hydroxychloroquine n=875 (40%)
Plasma from recovered patients n=363 (46%)
Percentage of physicians to report that HCQ/CQ is at least partially effective (scoring 2 or higher on the scale 0 – 5) against COVID-19:
Table 3. Physicians rating HCQ/CQ at least partially effective
Global: 85%
US: 81%
Italy: 94%
Spain: 91%
China: 88%
This data suggests that physicians in countries with more than average COVID-19 experience appreciate HCQ more than physicians in countries with less than average experience.
Usage
N = 1337 (the number of COVID-19 treaters out of the 4016 physicians surveyed)
SCREENING: COVID-19 treaters
Table 4. Medications physicians have used to treat COVID-19 patients
| Drug | % |
| Azithromycin or similar antibiotics | 58% |
| Hydroxychloroquine or Chloroquine | 50% |
| Anti-HIV drugs (e.g. Lopinavir plus Ritonavir) | 23% |
| Drugs used to treat flu (e.g., Oseltamivir) | 22% |
| None | 16% |
Treatments used by less than 10% COVID-19 treaters are excluded here.
The survey did not include inquiries about drug combinations. However, these numbers and well-known information from other sources suggest that in most cases when HCQ or CQ was prescribed, it was in combination with Azithromycin (AZ).
There were important differences in the perceived effectiveness of HCQ in the US as compared to the rest of the world. In the US, HCQ/CQ was used by 39% of COVID-19 treaters, compared to 75% and 83% of practitioners in Spain and Italy, respectively. Of note, Spain and Italy broke the rapid rise and started a rapid decrease in death rates around April 2-3 (Our World in Data, 2020).
Sermo Week 4
(Sermo W4, 2020)
Survey Period: April 13-15
Published on April 23
Country: Global
N = 1376 (after screening; 5,500 doctors were surveyed)
SCREENING: COVID-19 treaters
Effectiveness
N = 1376 (636 Non-Hospital physicians / 1045 Hospital physicians; except ICU only)
Q11. Effectiveness on patients outside hospital setting (Mild/Moderate): For patients you treat outside the hospital (mild/moderate in community setting), rate the efficacy of medications you have used to treat COVID-19.
NET: Very/Extremely Effective (Don’t Know Excluded)
Table 5. VEE Treatments
| Non-Hospital | Hospital ex/ICU | |
| n=636 (Q8) | n=1,045 (Q9) | |
| Hydroxychloroquine | 88 (38%) | 196 (31%) |
| Azithromycin | 79 (23%) | 126 (19%) |
| Vitamin C | 39 (26%) | 36 (19%) |
| Drugs to treat flu | 31 (24%) | 66 (26%) |
| Plasma | 23 (68%) | 63 (61%) |
| Zinc | 20 (25%) | 19 (20%) |
| Anti-HIV drugs | 19 (27%) | 71 (22%) |
| Remdesivir | 10 (27%) | 50 (34%) |
Results ordered by the number of physicians who rated the drug Very/Extremely Effective in the more relevant, non-hospital group. (Results are listed only for drugs in Table 6 in the next section) Notice that percentages in parentheses exclude treaters who did not answer the question about each drug’s effectiveness. Effectiveness of HCQ was rated differently in different countries. In the US, it was rated below its rating in the rest of the world.
HCQ / HCQ+AZ is clearly in the league of its own, per number of physicians rating it as “Very or Extremely Effective”.
Usage
N = 1376 (636 / 1045 for Non-Hospital physicians / Hospital physicians, except ICU only)
SCREENING: COVID-19 treaters
Table 6. Share of COVID-19 Treating Physicians Who’ve Used Medication Within Setting
| Non-Hospital | Hospital ex/ICU | Computed Average | |
| n=636 (Q8) | n=1,045 (Q9) | ||
| Azithromycin | 60% | 70% | 65% |
| Hydroxychloroquine | 40% | 66% | 53% |
| Drugs to treat flu | 22% | 25% | 23.5% |
| Anti-HIV drugs | 12% | 32% | 22% |
| Vitamin C | 28% | 21% | 24.5% |
| Zinc | 17% | 11% | 14% |
| Remdesivir | 6% | 16% | 11% |
| Plasma | 6% | 10% | 8% |
Simple averages have been computed to reflect the higher probability that HCQ-based treatment was started early in non-hospital settings compared with hospital settings.
Given the low standalone effectiveness and broad use of AZ, it is likely that in most cases HCQ was used in combination with AZ. The relatively large percentage for physicians using and highly rating Zinc suggests that HCQ+AZ+Zn was used extensively.
Note 1
33% of treaters complained about HCQ shortages. For comparison, only 27% of the treaters complained about ventilator shortages. The number was 48% for Super Treaters (doctors who treated >20 COVID-19 patients) outside of hospital settings. It is reasonable to conclude that HCQ treatment results would have been even better if not for HCQ shortages, causing treatment delays.
Note 2
This survey captures the relevant results of treating about 25,000 – 30,000 COVID-19 patients (Q7).
InCrowd
(InCrowd, 2020)
Survey Period: April 14-15
Published on April 21
N = 203
Country: USA
Specialties: US Primary Care Physicians (61), Pediatricians (59), and Emergency Medicine or Critical Care Physicians (83)
SCREENING: Physicians who have or are currently treating 20 or more patients with flu like symptoms
Q11: For what percentage of your COVID-19 patient population would you prescribe each of the following treatments? If other, please specify.
The offered options are: Acetaminophen, Antibiotics (e.g. azithromycin, etc.), Bronchodilators, Hydroxychloroquine, Plasma (from recovered patients), Ibuprofen, Remdesivir, Antivirals, Chloroquine, Steroids (High Dose), Flu treatments (e.g. Tamiflu, Xofluza), Herbal remedies, Anti-HIV Drugs, Interferon-Beta, Other.
Table 7. Surveyed physicians would prescribe to this % of their COVID-19 patients
| Drug | % |
| “Azithromycin etc.” | 41% |
| Hydroxychloroquine or Chloroquine | 30% |
| Plasma | 21% |
| Remdesivir | 16% |
| Antivirals (non-specific) | 10% |
Flu treatments (e.g. Tamiflu, Xofluza), Anti-HIV Drugs, Interferon-Beta, and Other scored 2%-7% each.
No answers were reported about the combination of drugs, but the numbers suggest that non-pediatric doctors would prescribe HCQ+AZ to ~40% of their COVID-19 patients. Many physicians using HCQ prescribe it only to those deemed at risk, so 30-40% is impressive.
Jackson Coker
(Jackson-Coker, 2020)
Survey Period: April 4-7
Published on April 8
N= 1,271
Country: USA, all 50 states
Reported margin of error is 3% with a 95% confidence level.
SCREENING: None. All physicians who elected to answer the survey, about 1% of the firm’s database of physicians. It was not established whether they treated or did not treat COVID-19 patients. It is likely that there was positive self-selection by doctors who treated COVID-19.
65% said they would prescribe drugs chloroquine or hydroxychloroquine to treat or prevent COVID-19 in a family member. 54% said they would prescribe it early, while another 11% said they would prescribe it if the disease becomes serious. 30% said they would prescribe chloroquine or hydroxychloroquine to a family member prior to the onset of symptoms if they had been exposed to the coronavirus. 11% said they would not use the drug.
73% of physicians practicing solo or with ownership stake in a practice, said they would prescribe HCQ/CQ to a family member. That means that more experienced physicians are more likely to prescribe HCQ. The share drops among critical care, emergency medicine, and hospitalists to 43%, 55%, 54%, respectively.
The lower usage of HCQ by critical care and emergency physicians can be explained by the fact that they are dealing with patients in a later stage of COVID-19, which might be characterized as a different illness, dominated by ADRS and multiple organs damage, rather than by viral infection.
Discussion
Only a small fraction of physicians use plasma, but they highly rate it.
Doctors’ wide-spread use and high recognition of HCQ+AZ treatment against COVID-19 is strong evidence, and, possibly, conclusive proof of the treatment’s safety and effectiveness.
Later Surveys
Sermo’s weekly COVID-19 surveys break the results down by regions, countries, and other useful categories. Sermo continued publishing surveys about doctors’ choices of COVID-19 treatments even after April 19. In May, they reported a decline in the use of CQ/HCQ and a rise in the use of Remdesivir.
InCrowd conducted a similar survey on May 29-31. It also reported a decline in the use of CQ/HCQ and a rise of Remdesivir, possibly for external reasons.
Jackson Coker has conducted no other related surveys.
Remarks
Some doctors started adding Zinc to the HCQ+AZ cocktail, as reported in (Risch, 2020). It is expected that additional experience in treating COVID-19, since the surveyed period, has increased the safety and effectiveness of multiple treatments, including HCQ-based ones.
Conclusions
85% of the globally surveyed physicians recognized HCQ as at least partially effective in treating COVID-19, according to Sermo W3. More than half of the surveyed US physicians would take the drug or give it to family members early or even before onset of symptoms, according to JC.
Aside from the rarely used plasma, HCQ / HCQ+AZ based treatments are preferred by physicians by wide margin over other drugs. HCQ / HCQ+AZ based treatments are the most used, most recommended, and most highly rated by physicians treating COVID-19 at an early stage.
Personal Note
Except for this paragraph, this paper appears here exactly as it was submitted to medrxiv.org on June 30 (MEDRXIV/2020/143800). It was rejected today, on July 4: “We regret to inform you that your manuscript will not be posted. A small number of papers are deemed during screening to be more appropriate for dissemination after peer review at a journal rather than as preprints.“
I felt this might happen when I saw medrxiv’s home page “Supported by Chan Zuckerberg Initiative“. Now, I submit it to an open peer review.
On a side note, speaking of New Paper Demonstrates Strong Efficacy of Hydroxychloroquine. Mortality rate cut in half!
there is an earlier peer-reviewed paper, confirming HCQ+AZ effectiveness:
Jean-Christophe Lagierab, Matthieu Million, Philippe Gautret, Raoult, Didier et al., Outcomes of 3,737 COVID-19 patients treated with hydroxychloroquine/azithromycin and other regimens in Marseille, France: A retrospective analysis, June 25, Travel Medicine and Infectious Disease https://www.sciencedirect.com/science/article/pii/S1477893920302817
References
FDA. 2020. FDA cautions against use of hydroxychloroquine or chloroquine for COVID-19 outside of the hospital setting or a clinical trial due to risk of heart rhythm problems. fda.gov. April 24, 2020. [Cited: April 24, 2020.] http://archive.is/xwOAc.
Gautret, Philippe , Lagier, Jean-Christophe and Raoult, Didier et al. 2020. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial. International Journal of Antimicrobial Agents. March 20, 2020. https://www.sciencedirect.com/science/article/pii/S0924857920300996.
InCrowd. 2020. Novel Coronavirus COVID-19 Physician Tracking Report. InCrowdNow.com. April 21, 2020. https://incrowdnow.com/wp-content/uploads/2020/04/InCrowd-Novel-Coronavirus-COVID-19-Physician-Tracking-Report-Wave-4.pdf.
Jackson-Coker. 2020. Physicians Poll on COVID-19 Medications. JacksonCoker.com. April 8, 2020. includes https://jacksoncoker.com/about/in-the-news/physician-poll-on-covid-19-chloroquine-and-hydroxychloroquine/. https://jacksoncoker.com/landing-pages/physicians-poll-on-covid-19_medications/.
Our World in Data. 2020. Daily new confirmed COVID-19 deaths per million people, rolling 7d average, Spain & Italy. ourworldindata.com. 2020. [Cited: June 29, 2020.] https://ourworldindata.org/coronavirus-data-explorer?zoomToSelection=true&time=2020-03-09..2020-05-15&deathsMetric=true&dailyFreq=true&perCapita=true&smoothing=7&country=ESP~ITA&pickerMetric=location&pickerSort=asc.
Raoult, Didier. 2020. COVID-19, presentation at GENERAL ASSEMBLY AP-HM CARE AND DIAGNOSIS. mediterranee-infection.com. March 16, 2020. https://www.mediterranee-infection.com/wp-content/uploads/2020/03/COVID-19.pdf.
Risch, A Harvey. 2020. Early Outpatient Treatment of Symptomatic, High-Risk Covid-19 Patients that Should be Ramped-Up Immediately as Key to the Pandemic Crisis. American Journal of Epidemiology. May 27, 2020. https://doi.org/10.1093/aje/kwaa093.
Sermo W3. 2020. Sermo’s COVID-19 Real Time Barometer Study, Wave 3. Sermo.com. April 15, 2020. includes https://app.sermo.com/covid19-barometer, https://www.sermo.com/press-releases/sermo-reports-week-3-results-globally-17-point-increase-in-covid-treaters-who-have-used-hydroxychloroquine-33-50-and-azithromycin-41-58/. https://public-cdn.sermo.com/covid19/dd/c7f7/f7344a/344a00427889ec27e2b8df1c15/w3-sermo-covid-19-barometer.pdf.
Sermo W4. 2020. Sermo’s COVID-19 Real Time Barometer Study, Wave 4. Sermo.com. April 23, 2020. includes https://www.sermo.com/press-releases/sermo-reports-jury-is-still-out-on-remdesivir-31-of-physicians-who-have-used-remdesivir-rate-it-as-highly-effective-31-rate-it-with-low-effectiveness-38-rate-it-as-somewhere-in-the-middle/. https://public-cdn.sermo.com/covid19/c2/3aba/ba8889/88898d406a8a84a60947e34a56/sermo-barometer-banner-tables-wave-4.xlsx.
The National Institutes of Health COVID-19 Treatment Guidelines Panel . 2020. Coronavirus Disease 2019 (COVID-19). covid19treatmentguidelines.nih.gov. April 20, 2020. [Cited: May 1, 2020.] http://archive.is/gk3xt.
There is a very useful resource for research paper links here:
https://c19study.com
Thx for the link, poison fir some specialists here 😀
Yeah, thanks. IMO, the Lagier et al. study, i.e. the very latest paper from the Raoult group is probably the most up-to-date. Singled out here:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7315163/
+100
It bothers me when I see figures in a graph that do not correspond to published numbers. If you look at the number of deaths per million, updated on 7/11, the numbers for the US appear to be at about 550 and above France.
We are at 413, and below France, according to the link below for the same date.
https://www.worldometers.info/coronavirus/#countries.
So which numbers are correct?
Don’t forget to treat early and include zinc (unless the objective is a poor outcome, in which case, adjust data as needed).
No one should wait to get sick to make sure they have plenty of every nutrient associated with immune system health.
In fact, everyone should know the exact list of all essential nutrients for a human being, and have at least basic knowledge about the role each plays in our body.
No one can be healthy without proper nutrition.
It used to be easy.
But modern food industry and marketing has made it hard for our own instincts…our nose, eyes, and tongue…to tell us what we need, what is good to eat, what is bad, etc.
First biology class I took in college, first semester, human health and reproduction.
Nothing Earth shaking, but detailed and specific knowledge replaced sketchy information with some fine detail but huge gaps.
Most people don’t know anything about proper nutrition, some a bit. But it’s not so easy to have a proper nutrition, there are many reasons, why. Learning at school is deplorable, missing time for several reasons is mainstream if you are working, or in case of parents, both are working to buy and prepare proper nutriotion in case they know at least a bit about.
Fruits you can buy are mostly unripe with vitamine deficits, vegetables usually come from in general outleached grounds with some mineral deficits.
Working indoors is one reason for vitamine D deficits.
And if you have a look at at least the German Greens, they try to regulate the market for nutrition supplements, because they believe, they are not necessary, to high dosed etc.
As usual, they have no clue of real life and it circumstances.
Forgot to mention, short of money is a reason too for mal nutrition.
Poverty is a real killer. No healthcare systems and no proper food. The numbers for Africa are horrendous, but Germany is seeing kids malnourished.
The US too. And elderly are systematically vitamin D3 deficient.
The Greens will say let them eat green leaves, drink “natural” water.
Note the recent report on COVID in sewage samples from mar-2019 – just imagine what bad water and sewage treatment will do!
The poor in America are the most overweight and obese population in the country. There is plenty of money for food, it’s just spent poorly.
“Fruits you can buy are mostly unripe with vitamine deficits, vegetables usually”
Say what?
Do you have evidence for this?
Ripeness has to do with starch being converted to sugar, and the vitamins are already there.
If the ground in which plants are grown do not have the nutrients plants need, they will not grow.
Even small deficits in mineral concertation will make a plant look very obviously wrong.
Spots, yellow…
Are you really saying that buying fruits and vegetables is a fools errand because they are all crappy?
Are you saying junk food is more affordable than wholesome foods?
The opposite is true in both cases.
Processed foods are expensive, calorie per calorie, compared to wholesome foods.
Where I shop foods are fresh and ripe, unless it is one of the well known ones that cannot be picked and shipped ripe.
Ripe bananas in the tropics will be mush before they get loaded onto the boat to ship them.
Pineapple is far better when picked bright yellow, but they are too soft to ship at that pont.
Except local ones in season, foods like tomatoes are picked green and ripened with ethylene gas to make them turn red.
They have zero flavor.
But all of these things have always been true.
I have been involved in agriculture since the 1980s, and right now have dozens of fruit trees and plants.
But most people do not even grow a garden for fresh greens and herbs during the times of year it is fast and easy to get a garden going.
Laziness and ignorance are the problems, not leached soils and unripened fruit.
OMG
No, but they could be healthier, could have more minerals, even if not deficient for growing.
Source
An other with more examples
Source, German
Not everybody has a garden as we have it, and is able to grow the plants they want or need, as you state at least correctly.
Don’t get your shorts in a twist. The “nutrients plants need to grow” and the “nutrients animals/omnivores/humans need to get from those plants” are not identical. Large Venn overlap, but not 100%. Commercial farmers must cater to the plants’ needs. It’s up to us humans to look out for the rest. Laziness is not necessarily the problem with city beehive dwellers. Ignorance and misinformation propagated by FDA and DoAg surely is a problem.
You want more ?
A Study on the Mineral Depletion of the Foods Available to us as a Nation over the Period 1940 to 1991
Full study
New UK Study Shows Decline in Fruit
and Vegetable Mineral Content
This section is compiled by Frank M. Painter, D.C.
Enough ?
Go in your garden and play around 😀
Nicholas,
Almost everything you say is correct. There are a lot of greenies out there who will tell you something was better in the past. Food is one of them They usually give organics a pass from such judgement. I still remember as a kid watching some of the neighboring farms that grew organically. Unlike us, those farmers wore environmental suits suits while working the fields, and rode in enclosed tractors with AC – still in those outfits. Because what they were spraying on those fields was more safer than what we were using…?! There is a reason organic food does not usually look as good as “Non-organic” food (an oxymoron, as any chemist knows). When organic food does look as good as non-organic, check the nation of origin. It’s usually China. They don’t allow American inspectors on their farms.
American farmers have been rotating crops since the 40’s. I understand that some areas of the world don’t do that. DON”T EAT THEIR FOOD!
My wife is an animal rights activist. I remember her showing me a photo a couple of years ago of a guy who had gone into a wolf or coyote den to kill the pups. He then posed with his trophies. I told her that photo was ancient. She contacted the source (ASPCA donation drive). They confirmed that the event had taken place in the 1940’s, and the man worked for the Government. They had no newer pictures, but assured her the Government was still doing this, and her donation could help stop this barbarous activity.
The data about American-farmed food having fewer minerals is just as valid. We did prefer the food Grandpa and Uncle Bob had grown versus the grocery store – it was fresher. Greenie scientists extrapolate the mineral content from the past using models. Hm. Who else does that?
And to this day, I will not touch “organically-grown” food. The stuff they can put on it is dangerous. Just look at those environmental suits. They are not to protect the food from the farmer.
I apply Azomite rock dust to the garden every spring before planting.
Been using it for several years now.
The stuff makes a noticeable difference in the taste and appearance of all the vegetables.
See https://azomite.com/azomite-home-page/frequently-asked-questions-about-azomite-mineral-products/
@Yirgach
We use so called powdered limestone, hornshavings and compost from our heap.
And we add smal pieces of wood charcoal remaining from last BBC.
Most people have no place to plant anything.
Today, discussing nutrition might be seen as racist. /s
Counter question: what is not racist ? /sarc
How about Susan Ricist?
Lookin’ to run with Biden, and well, blow the planet up.
OK, you opened the door, so I have to post this now because it’s one of the funniest things I’ve seen lately. This is the man running against Trump.
https://twitter.com/FogCityMidge/status/1255245341886218241
So 85 % of doctors globally used HCQ but only 43% in America. I think if I ever got sick I would ask who my doctor voted for before handing myself over for treatment. Just sayin’
My GP has said he will prescribe the HCQ /Azith/ Zinc group if I contract Covid-19 particularly after being tested. I am in the senior citizens age group. When I spoke to him about this treatment it was like “You may very well say that but I could not possibly comment” and so he agreed to write a prescription if the time came, because he is fully aware of the survival rates from it.
For those whose doctors won’t prescribe HCQ, make a reservation for a weekend trip to a malaria-infested country and demand the doctor give it to you for that.
Or just go across the southern border…..and buy it over the counter
Or some Chinese chalk that is marked the same way.
Great whit, hiskorr.
I second Dave!
NMG will tell us in thousands of words that the studies are all flawed and/ or meaningless, because he just found a study that…..
I am all up in your head, aren’t I?
Cupcake, you have no idea how big that makes me smile.
You ? 😀 😀 😀
Don’t be to proud of yourself as if I mention you in a positive way.
You are the best example of what a negative one is 😀
Pretty sure you don’t exist anywhere in reality.
And…Leftist never smile….that was a leftist lie. Leftists always lie.
I’ll have to take your word for it.
One thing is for sure and everyone knows it: @ur momisugly$$holes will be @ur momisugly$$holes.
Thanks for my daily reminder.
Nicholas: Perhaps Krishna is being too kind, so that you misinterpret, as you are want to do.
When people see cockroaches, rats, house flies, and bats at a wet market, the informed look in disgust because of what’s in their heads.
That is how in our heads…
It also tells everyone you have no idea what people are saying, because you do not listen, do not read, do not recall…
In any case, this is not a study, it is a survey.
Might as well call a poll a study.
John Cook called his “work” a study too.
But this is from April, when no one knew as much as they do now.
I happen to know that they are still polling people.
I have not looked at them for a while, but I will now go and see how polls from right now look.
Not because I find them to be highly compelling, but because obviously what people think now is derived from more information and experience than ones taken last April.
Have you learned anything new since April?
Not from your comments, be sure 😀
Gans
I don’t feel that you are contributing anything substantive to the dialog. Your forte seems to be insults to those who hold a different opinion. How about trying to attack the statements with logic and facts instead of attacking the person?
It has been my experience that Nicholas has contributed more in the way of information and analysis than most here. I wish I could say the same about you. I wouldn’t be any more ignorant if you had never posted anything.
Let me ask you a question. What are the chances that some obscure doctor who published early, that no one had heard of before the pandemic, would come up with the right dosage of a drug never before used for this disease, and the right amount of time to take the drug? Consider that the dosage and amount of time to take a drug are usually an essential part of early trials for new treatments. Now this doctor just might be Sherlock Holmes’ smarter brother — Shear Luck — but, it seems improbable to me. HCQ just might turn out to be the best thing in the world for COVID-19; however, at this point in time, the evidence for that is very poor. Those who promote it based on anecdotes and small, non-random trials are not scientists. They are in the same category as those who avoid black cats and throw salt over their shoulders after spilling some.
“What are the chances that some obscure doctor who published early, that no one had heard of before the pandemic, would come up with the right dosage of a drug never before used for this disease, and the right amount of time to take the drug?”
Well a doctor should be able to understand how to get information on a drug that has been around for over 60 years. So I don’t but that assertion. Sars was like 1.5 decades ago and there is a plethora of medical information about Chloroquine at known safe doses that were proven to be effective.
The bad studies, most of which failed, show the worst of society. The people who want there not to be a cheap cure are evil at best. I am not saying I know which people are evil…
HCQ+ is cheap, safe and has some evidence it helps if taken early, Clyde. Why don’t you just jump on a different TDS horse? My review of the study “proving” HCQ causes heart troubles showed it was a pile of steaming ideological crap. Any supposed scientist or medical practitioner supporting it is/was a liar.
After my WuFlu diagnosis yesterday, I will be taking HCQ+ one way or another. At age 72, I’ve learned my reasoned judgement is usually right-on. Listening to ideologues or representatives of special interests (as you apparently are one or the other) always gets one in trouble or costs one alot of money (even poverty), usually both. And death is not an uncommon outcome.
I’ve closely followed the arguments on every side of the various ChiCom virus and WuFlu debates since day one. They have all degenerated into ideological debates driven by misinformation from ChiCom, WHO and other politicized sources. The mere fact that those sources do not clearly inform reviewers that the results from their studies are based on application of HCQ to near-terminally ill patients indicates they are deliberate propaganda.
Screw off, Clyde.
But Dave:
Can’t you just be patient, and wait another 4 months? There’s a respirator there you can use too…
Of course that was sarcastic… Be well, and good luck sir. Keep up the vitamin D too.
Thanks, Mario! Sarcasm aside, at no time is anybody shoving that tube down my throat. I’ll do everything in my power to avoid that fate. Clyde has no common sense.
I as one would not dare! 🙂 You are a fighter… and you will be fine, I can (unscientifically) feel it.
You might be more correct than you know, Mario. If I ever get a chance, it would be fun to tell you how I went back to Fresno, CA a week later to successfully retrieve my stolen, future-champion Pug dog. I usually accomplish what I truly set my mind to. I appreciate your good feelings towards me, Mario.
Hey, I would love to take that off line. Would be a great story to hear. Your situation certainly gives you a pass by the way, on your colorful language… and that your responses are well reasoned, regardless of whether people agree with your thought process. I just so happen to align…
If you mean with “obscure doctor” Didier Raoult, than be aware that he isn’t certainly not as obscure as you belive. He is what everybody calls a specialist and / or expert
And his studies and trials are based on earlier successful trials of treatment in China.
So he had a base for dosage and time amount.
And in the beginning, they were always testing the viral load and find out, how long to treat.
Btw. these studies have been discussed here iin earlier times and, as published on google docs, days later, they disappeared.
Dave Fair,
Right on! All the stuff I have seen corroborates what you said. All this anti-HCQ propaganda is TDS on steroids. We old folks should use it immediately and don’t forget the zinc.
But you old folk tend to be Trump voters, that is motivation enough to believe the opinion articles disguised as science… [disclaimer OK I have always gravitated towards older folks, shoveling snow as a kid, talking to older neighbors and grandparents when I could. The wisdom attracted me. I am 55, I am getting close myself… can’t wait!]
So they poo poo good anecdotal and better than anecdotal results because they did not follow a practice that someone needs to fund at great expense, while people die. And then if a study is funded, and runs filled with bad data that will later need to be retracted… that’s fine. Because it’s on CNN, and the MSNBC, NYTimes or the CDC or WHO said so.
Biden notwithstanding, old folks are not stupid nor easily mislead. My reference to HCQ+ means a combination of HCQ, AZ and zinc. It seems to be the ideal combination in the relevant studies.
Even at age 72, I did not seek to take HCQ+ until yesterday’s diagnosis of WuFlu. I think its use as a prophylactic should be saved for those in higher risk categories; the elderly with high blood pressure, diabetes, heart problems, obesity, etc. Having said that, I also believe that people should use their own judgement on taking HCQ+.
Good luck, Dan. Hopefully we come out of this politicized mess stronger as a people.
We have a winner of the title: Parrot of the Day
Thanks Clyde.
Dave,
I agree again, completely. My mistake for assuming immediately meant immediately on testing positive.
Breaking news moving world markets.
Experimental treatment reduced mortality by 62% in vivid patients:
“- Data Presented Includes a Comparative Analysis of Clinical Recovery and Mortality Outcomes from the Phase 3 SIMPLE Trial Versus Real-World Cohort of Severe COVID-19 Patients Receiving Standard of Care —
— Traditionally Marginalized Racial/Ethnic Groups Treated with Remdesivir Had Similar Clinical Outcomes as Overall Patient Population —
FOSTER CITY, Calif.–(BUSINESS WIRE)– Gilead Sciences, Inc. (Nasdaq: GILD) today announced additional data on remdesivir, an investigational antiviral for the treatment of COVID-19, adding to the available body of knowledge on treatment outcomes with remdesivir. The data are being presented at the Virtual COVID-19 Conference as part of the 23rd International AIDS Conference (AIDS 2020: Virtual) and include a comparative analysis of the Phase 3 SIMPLE-Severe trial and a real-world retrospective cohort of patients with severe COVID-19. In this analysis, remdesivir was associated with an improvement in clinical recovery and a 62 percent reduction in the risk of mortality compared with standard of care. “
how many different names have you used on this site Mcginley?
Back when I had to worry about being doxxed at work for being wrong on global warming, I used the handle Menicholas.
Since then I have used my name.
Something on your mind, boder?
One might think that anyone who wonders about that probably has sock puppets.
Are you concerned I slipped a comment in under your nose?
Lol, couldn’t care less what you do or don’t do.
You are very curious and ask a lot of questions for someone who does not care.
You didn’t realise, the poll was about studies, and I spoke about these studies, never mind 😀
But you tell me, I don’t read, nice 😀 😀 LOL
Nicholas
I read a poll that said Hillary will win the 2016 election. Must be true! 🙂 Funny how climate skeptics disparage consensus, but those pushing HCQ use it as their main support.
There have been so many different drugs tried, all showing some apparent benefit, that I think anyone with an open mind should consider the placebo effect as playing a role in all this.
Is there any consensus about HCQ ??
Not really, or did I miss s.th. ?
Btw, in questions of climate, there is s.th. like a skeptical consensus 😀
You can’t compare the one with the other if you are open minded (enough) 😀
I do not know about concensus, but I have noticed that ever since I made some comments that you disagree with about HCQ, you have not stopped saying my name, and making dumb replies to every comment I make.
Today the only thing on your mind, hours before I got here, was what I was going to say.
One thing you never do, and I mean NEVER…EVER…is read a comment, and then respond to someone in an intelligent manner, even if you disagree with them, even if they just have a random question.
Ever.
You have no idea how to read something, consider what is being said, and offer some thoughts in the manner of a conversation.
I liked you better back when you were a credulous, gullible, admittedly scientifically illiterate, and more or less a somewhat pleasant person.
Remember the day you learned that malaria was not a virus?
https://wattsupwiththat.com/2020/03/17/an-effective-treatment-for-coronavirus-covid-19-has-been-found-in-a-common-anti-malarial-drug/#comment-2940060
I re-learned the fact, as while commenting I in fact forgot it, point
For the rest:
You get out what you put in.
PS
You forgot
Mainstream vs climate skeptics
Mainstream vs use of HCQ
Virae prohibited to replicate is usually not to reduce on a placebo effect 😀
But maybe, Corona is a placebo ? 😀
In early April, the doctors knew the outcomes they had seen, and there was no political motivation to push results one way or the other.
No idea what to think about infos coming from Turkey, where everybody with symptoms is treated with HCQ, and have a lower death rate than Germany, in total and in relation to population.
Erdogan, while trying for a new Caliphate in Libya, threatened to allow infected migrants through. I’ll withhold judgement on any Turkish stats.
Goldstein publishes more of his personal interpretation of studies of studies of medical rumours here on WUWT. Can also be interpreted as 85% of physicians administering HCQ feel it is a positive psychological crutch at fairly low cost for patients wanting the best meds possible, even if they don’t really work. Pretty soon we should be up to the indisputable 97% consensus that it does something good/bad which we have heard before.
Just search on “HCQ ineffective” for an instant Goldstein rebuttal…..
Just compare the differences in protocols the studies you prefer in contrast to the studies of L. Goldstein or mdman above linked.
Maybe you could say exactly what it is you want to say?
What protocols are you referring to?
Which are the good ones, and why?
Which ones are not as good, and why?
Are you capable of that sort of communication?
Or are you just a little girly man who pretends to know sh!t from shinola after a few months of internet echochambering?
I think the warnings about the estrogenic properties of all that quercetin you are gobbling up has had the desired effect.
Growing tits yet, or is it all behavioral at this pint?
I never wrote about steroids or quercetin, learn to read comments, and wrote about what.
You never wrote about quercetin?
Is that what you said?
*rolls the eyes*
Steroids was part of the protocol that was changing over time.
You babbled something about comparing the protocols.
Try to keep up.
Was it a three drink lunch again?
DMacKenzie
July 7, 2020 at 7:03 am
It is a free choice world, supposedly… so if by any chance you consider a treatment for COVID-19, at some point in time,
please don’t take QHC, and maybe better do consider a seasonal flu vaccination, best a cocktail one, for a further boosting of your immune system, when at it.
It will be great if you manage to persuade also likes of Fauci and Billy Gates of this world to take the same route.
It will be and make it easier for all concerned, I think.
cheers
Whiten, everything you mentioned doesn’t do anything substantial for Covid19, or any coronavirus for that matter, so my choice WILL be to NOT take them for that purpose. The annual flu vaccine is worth it for flu. In Didier’s original HCQ study of 26 patients, 6 quit the treatment due to adverse reaction to the HCQ. Like you say, free choice…..
Get back to us if you catch the ChiCom virus’ WuFlu, DMacKenzie. Let us know what you think of HCQ+ then. Since my diagnosis, I don’t have a sense of humor about high-minded rationalizations.
I haven’t lost faith in my immune system. All the studies point to quite high recovery rates. /s
@DMacKenzie No, 6 did not quite due to adverse reactions to HCQ.
Maybe you need to re-read the study if you even did in the first place.
Here are the reasons :
“Six hydroxychloroquine-treated patients
were lost in follow-up during the survey because of early cessation of treatment. Reasons are
as follows: three patients were transferred to intensive care unit, including one transferred on
day2 post-inclusion who was PCR-positive on day1, one transferred on day3 post-inclusion
who was PCR-positive on days1-2 and one transferred on day4 post-inclusion who was PCRpositive on day1 and day3; one patient died on day3 post inclusion and was PCR-negative on
day2; one patient decided to leave the hospital on day3 post-inclusion and was PCR-negative
on days1-2; finally, one patient stopped the treatment on day3 post-inclusion because of
nausea and was PCR-positive on days1-2-3.”
Besides, that was only his very preliminary study, that he shared with the world, so others could also help determine if they would have similar results. Unfortunately, it would seem, they went on attack to try to discredit him instead of doing science.
He followed up with a study of 80 patients, then with another of over 1000 patients, and finaly with one of 3700+ patients.
This is the last one.
https://www.sciencedirect.com/science/article/pii/S1477893920302817
CBeaudry,
Death and/or ICU 93 2.5 35 1.1 58 9.4 <0.001 37 17 <0.001 3 3 0.1149 13 9.5 <0.001 5 3.1 0.0449
It’s a fine study, and I do not wish to denigrate the work that many people put into it…..
But look at, for example “Death and or ICU” numbers…..in percentages there is just no real difference whether 2.5 people out of a hundred died or 1.1 died or 3.1. There are many possibilities why sick people don’t recover and a percent doesn’t cover it. Also note the recovery times. Again a day is really insignificant. I’ve waited longer than that in hospitals to be released.
You are right, D McKenzie.
Any differences in the CFR can be easily shown to be either statistically insignificant, or the result of triaging patients prior to treatment.
If 100 people get the virus, and the ones who get very sick go to an ER, and the ones who get somewhat sick go to an outpatient care physician, and the outpatient care physician treats all of those people, then the results of that treatment cannot be compared to the set of all people who got the virus.
Because the worst off ones were removed by going to the ER!
And this is one of the reasons why without blinding and randomization, comparative studies about effectiveness OR efficacy are not scientifically valid.
There are many decades of examples of the proof of this.
It has been correctly state here and on other threads on this topic many times.
Many of the people who refuse to accept this principle are not operating on the level of science, but on the level of political considerations, or refusal to be persuadable.
Perhaps the most powerful force operating on many people regarding this and other such issues is pride and ego.
There are a lot of people in this world who do not wait for enough evidence to be available before making up their minds about some important issue.
If and when they have grabbed onto position or view or opinion which is factually incorrect, they will not be willing or able to admit it or to change their mind.
Too many people have made up their minds without all the facts in hand.
They are now doomed, and we with them, to remain locked into ignorance of the truth.
Thanks for the link, the results:
“Conclusion
Although this is a retrospective analysis, results suggest that early diagnosis, early isolation and early treatment of COVID-19 patients, with at least 3 days of HCQ-AZ lead to a significantly better clinical outcome and a faster viral load reduction than other treatments.”
The current issues is the on going TDS DNC talking points along with the cancel crowd rampant activities on anyone that publishes HCO-AZ positive results. Yesterday my local newspaper used an AP (DNC talking points) article that was unbelievably slated to discredit HCO: https://www.ksl.com/article/46774017/brazils-president-bolsonaro-tests-positive-for-coronavirus
Need less to day they did not publish my post about their use of DNC talking points.
Needless to say !
HCQ advocates are saying hard core conservatives, such as myself for example, are suffering from TDS.
Now the claim is that any result contrary to what HCQ fans want to believe, is DNC propaganda?
The upshot is, anyone who is not a leftist needs to hitch their wagon to a favorable outcome of clinical trials for HCQ curing COVID?
I sure hope this does not represent a widespread attitude.
DMacKenzie
July 7, 2020 at 4:38 pm
Many, you have no idea how idiotic, brain dead zombie, silly crazy stupid, this statement of yours is:
“The annual flu vaccine is worth it for flu.”
Completely stupid in steroids.
One of them givens is a natural proper persisting conditions, the other is simply a clause of stupidity in steroids.
Seasonal flu is a natural cyclic persistence, in consideration of at very least, of 100+ different viral infection diseases, periodic, seasonal, where the stupid humanos like you and me, but not only, are periodically subjected to the natural force of more than 100+ different viral infections disease’s force… of nature, of the life condition.
How much your silly seasonal flu vaccination against such does cover!
Tell me, 2%, 5%, or maybe 10%, at most!
Tell me stupid.
How does it suppose to work?
How much the flu vaccines work or impact against the natural force and power of seasonal flu.???
Let me tell you… nada, nilch zilch.
Only thing such vaccines do is upset the equilibrium of life, by causing an IDS condition in the prospect of herd immunity.
That the only worth of seasonal flu vaccines!
The main life code in the core of this novel corona virus, is far far much older than me you, Fauci, Billy Gates, or even all of us put together at 7 to 8 billion humanos.
Is millions and millions of years older than humanity itself.
Has being there many many millions of years before humanity.
You sillies think it can be stopped or blocked and controlled by face masks or insane lockdowns….please do think again.
cheers
Wrong. You are confusing common cold viruses with influenza. Completely different viruses.
Ron
July 8, 2020 at 7:24 pm
Ron, completely failing your point made!
All them little badies are “seasonal”, or are them not?????
And related to the same organ almost all.
Ron!
cheers
@whiten
What season is then the best vor SARS-CoV-2?
Summer? Like the southern states are showing right now.
Winter? Like in China.
Spring? Like in Europe.
The cold and flu do not damage your f***ing kidneys and clotting your blood to induce strokes and thrombosis.
Ron
July 9, 2020 at 1:24 pm
The cold and flu do not damage your f***ing kidneys and clotting your blood to induce strokes and thrombosis.
——————-
Exactly “little dancing boy”. 🙂
A condition or syndrome called IDS does that, easy.
Especially badly and deadly when non natural in origin.
Good.
You going around and still coming around, with your “dancing”.
🙂
cheers
Ron
July 9, 2020 at 1:24 pm
Summer? Like the southern states are showing right now.
Winter? Like in China.
Spring? Like in Europe.
———————
Ron, the main point of the questions you posed is simply matter of dumbness and illiteracy.
Not understanding the point of “panic”.
Will be the same with the consideration of seasonal flu versus this new corona virus.
The difference in the clause is the panic… instilling of fear, by any means possible.
If panic the same as per normal seasonal flu, the picture will be the same, dummy.
Simply choice of tracing it or not as for more panic to be produced.
Whichever way considered, the further tracing of this novel corona virus as happening, persist only due to panic and fear… it is not any more in its peak infectious disease epidemic vector for almost all countries or herds in consideration.
It is simply basically applied as a scare mongering story, at this stage, Ron.
Can you understand this simplicity!!!!!
If the same method approach applied for seasonal flu epidemics, and followed ever so thoroughly the same picture will arise.
Is not like we ever done this before for seasonal epidemic influenza…
it is a first, in only one aim, scare the shite out of you, and with no regard or responsibility… Ron.
Some record like this about a seasonal epidemic influenza does not exists there yet because we never before this went so far as becoming so crazy, insane and self destructive.
cheers
Hmmm, since this hydroxychloroquine treatment for Covid-19 first appeared for me at least on Dr. Roy Spencer’s webpage March 18th and sometime later we found out that hydroxychloroquine is routinely prescribed for Rheumatoid Arthritis & Lupus, it would be interesting to see the rates of Covid-19 infection for those Lupus and Rheumatoid Arthritis patients compared to the population at large.
That’s also the data I want to see, Steve, does the group already under treatment with hydroxychloroquine show clear evidence of protection against either incidence or severity of Covid-19?
Zhong et al. Lancent Rheumatology, 10.1016/S2665-9913(20)30227-7 (Peer Reviewed)
COVID-19 in patients with rheumatic disease in Hubei province, China: a multicentre retrospective observational study
Rheumatic disease patients on HCQ had a lower risk of COVID-19 than those on other disease-modifying anti-rheumatic drugs, OR 0.09 (0.01–0.94), p=0.044 after adjusting for age, sex, smoking, systemic lupus erythematosus, infection in other family members, and comorbidities. 43 patients with rheumatic disease and COVID-19 exposure.
Yes and in Italy a survey of 65000 lupus & arthritis patients, only 20 caught COVID-19.
https://www.jpost.com/health-science/italian-scientist-says-she-discovered-main-mechanism-behind-covid-19-626737
Near the bottom of the report.
That “only 20 out of 65,000” is a smoking gun if true but I’m afraid the gun was loaded with blank cartridges.
Chiusolo was just repeating — possibly originating — some rumor that was mysteriously circulating in the beginning of May. That round 65,000 number was suspicious in itself… I thought then, if she knows the precise number of patient positives and presumably has access to an accurate number of patients, why only share such a preposterous estimate as “65,000”?
It may be she misspoke during the interview or was misquoted by the Jerusalem Post. Derek Lowe consulted the Global Rheumatology Alliance directly on May 4 articleand they were tracking only 11,762 patients worldwide. He was unable to source the 20/65000 ratio.
“Yes and in Italy a survey of 65000 lupus & arthritis patients, only 20 caught COVID-19.”
The link is to a newspaper report only, and it is completely wrong.
From Science:
“The number is completely fictional. As mentioned here in the comments, the president of the Italian Rheumatology Society was contacted directly and states that this number is completely wrong, that the society is monitoring 150 patients in its registry, 20 of whom are taking hydroxychloroquine. The 65,000 number is bogus.”
Earlier in the pandemic, I listened to a doctor explain (can’t remember who or where sorry), that they could not find a single lupus patient who had contracted COVID-19. He had put out an appeal to try to find one out of the 2 million or so lupus patients in the US who had the virus.
It’ inexplicable why such data hasn’t been collected and collated. It’s very likely easily available.
I am currently doing my own study where n=1=myself.
You mean that you have not seen the Italian retrospective survey?
https://www.jpost.com/health-science/italian-scientist-says-she-discovered-main-mechanism-behind-covid-19-626737
You have to read quite a long way down to find it 65,000 patients, only 20 with covid-19.
That seems to be significant.
I posted about this last night.
People with lupus are getting it, in high numbers.
And when they do, it is bad.
Here is a link to one of the posts I made.
And here is the link to a regirstry of 600 patients with rheumatic disease who are infected.
45% wound up hospitalized, so far, and 9% are dead…so far.
There was no protective effect from being on HCQ when they got sick.
There were two groups that had a protective effect…those taking biologics, as they are called.
Anti-TNF drugs worked the best, they were protected, but only partially.
People taking anti-IL-6 drugs were also protected, but not as much.
Here is the link, and this is what good data collection looks like:
https://ard.bmj.com/content/annrheumdis/79/7/859.full.pdf
You can’t make the statement there is no protective effect. What was the state of their health… Lupus is an auto-immune disease… whereby treatment quells the misguided immune system.
If you understood how HCQ and Zn worked you would know that is slows viral replication in the presence of ample Zn, which gives your “functioning” immune system time to respond.
Two parts, get it?
If you cared about providing information, why do you treat every issues like a biased hack?
I did not originate the statement.
I was summarizing one of the results of the work I linked to.
It is right in the first paragraph of the paper.
Here is the text:
“Results A total of 600 cases from 40 countries were
included. Nearly half of the cases were hospitalised
(277, 46%) and 55 (9%) died. In multivariableadjusted models, prednisone dose ≥10mg/day was
associated with higher odds of hospitalisation (OR
2.05, 95% CI 1.06 to 3.96). Use of conventional
disease-modifying antirheumatic drug (DMARD)
alone or in combination with biologics/Janus Kinase
inhibitors was not associated with hospitalisation
(OR 1.23, 95% CI 0.70 to 2.17 and OR 0.74, 95% CI
0.37 to 1.46, respectively). Non-steroidal antiinflammatory drug (NSAID) use was not associated
with hospitalisation status (OR 0.64, 95% CI 0.39 to
1.06). Tumour necrosis factor inhibitor (anti-TNF) use
was associated with a reduced odds of hospitalisation
(OR 0.40, 95% CI 0.19 to 0.81), while no association
with antimalarial use (OR 0.94, 95% CI 0.57 to 1.57)
was observed.”
The information that is the basis of that summary is extensively documented ands described in numerous tables of data.
That is what the data says.
It is not what I say, and your assertion that ” I cannot say it” is nonsense.
mario: I urge you to reconsider this. McGinley’s only agenda is to live up to the creed, “first, do no harm.” He has been ultra cautious re: hcq, but he explains himself and cites his sources. You seem like a reasonable guy, read his posts and tell me where he is wrong. He demonstrated a clear understanding of how the “two parts” work in a lab. He hasn’t seen good evidence (he doesn’t make Mr. Stokes’ error of re-defining “evidence” to suit a whim) that it works in the field.
P.S.- Not that he needs me to step in, one thing you must grant is that McGinley stands his ground. In any event, he doesn’t deserve to be insulted.
Hi Paul: Thank you for your ability to craft a gentle missive.
If you are responding to my statement, “You can’t make the statement there is no protective effect.”
I could restate it as, “You can make any statement you want.” Not that I am the decider of who should have opinions. 🙂
There is no “proof” that HCQ and Zn at the prescribed levels and duration we are talking about causes widespread harm or does not have a protective effect. One can argue about that all day long, so that will not be resolved by this response.
There is plenty of “evidence” that HCQ and Zn have a protective effect.
One can argue about whether or not HCQ is defined as an ionophore or not all day long. I have only seen evidence that it is called an ionophore by doctors in the field. It is not clearly defined how it can be determined, hence the debate.
The evidence that there has been a protective effect has been shown in many cases.
The debunking of the dangers of HCQ for Covid patients has also been widely circulated. The debate will go on and not be settled here.
So it goes back to “First do no harm”, the Hippocratic oath. I am glad you brought this up.
That does not mean, do nothing! I think there is strong evidence that in this case, there is much more harm being done, by not using HCQ and Zn early on, as prescribed.
Look at it as a probability. Doing nothing… you get what we have. Supplying HCQ and Zn early on has shown no harm, and has shown better outcomes fewer deaths.
These are the people that have been much discussed…people with diseases like RA and lupus, and other conditions of a similar nature called rheumatic disease, collectively.
The status of this group of people has been much talked about, and it is now obvious most of the talk has been based on erroneous information.
In other words, people are saying a lot of stuff that is not true about people who have been taking HCQ, and using the misinformation to invent a bunch more misinformation.
So, no w there are multiple data sets of these specific individuals.
Interestingly, many people with such diseases take some of the other types of drugs that are being used to treat covid patients.
And a sample of 600 people with these conditions, of which lupus appears to be the second most common, and who have also contracted COVID-19, has been closely examined and a whole bunch of information about their condition and situation is compiled.
This is not based on what anyone wants to think, or believes to be the case, or was hoping would be found to be the case, or anything like that.
This data is all gathered based on actual people and what they took and how they have fared after contracting COVID 19.
Some might view it as extremely valuable information from which a wealth of insight might be gleaned.
Of course, that would be people who would like to have factual information, no matter what it tells us.
The type of person who is of a scientific bent is one example of who might want to get data of a factual and unbiased nature.
Others might seek to dismiss it, and give it no weight, or make excuses for why it is not important, or relevant, even if such efforts were transparently biased.
I am not at all sure what would motivate anyone to do so, but here we are.
So, these people are already taking this stuff.
IL-6 blockers.
HCQ.
Anti-TNF drugs.
Steroids.
And there is what happens to these people, compiled in detail.
Summarized and analyzed.
Anyone can see that we have people in this country who have appointed themselves professional obfuscators.
Exactly why will be a question for the ages.
Thank you Paul.
I really do appreciate someone who defends the person getting ganged up on.
As Rud has aptly put it, I am interested in popularity contests.
We have people with whom I have had little to agree with over many years on this site, with whom I am now in almost full agreement on at some aspects of what is happening with this pandemic.
I have no problem or qualms about standing up next to these people and supporting them on that which we can agree on.
Crap…NOT interested in popularity contests.
There’s a very significant difference between the Italian study as posted by A C Osborn, and the BMJ article Nicholas McGinley posted. The italian study reported that very few of the patients taking HCQ were diagnosed with WuFlu. The BMJ article looked only at patients that had already been diagnosed with WuFlu.
“The italian study reported that very few of the patients taking HCQ were diagnosed with WuFlu.”
It was not a study, but a nonsense newspaper report
From Science:
“The number is completely fictional. As mentioned here in the comments, the president of the Italian Rheumatology Society was contacted directly and states that this number is completely wrong, that the society is monitoring 150 patients in its registry, 20 of whom are taking hydroxychloroquine. The 65,000 number is bogus.”
Mike,
You are correct.
I have no confidence in the Italian study, since it has been refuted by people within the community of people represented.
I am going to stick to opining on information that stands up to scrutiny as being legitimate.
I am not saying the Italian study is accurate or has any value or not.
What it appears to be is an estimate of the number of people with the disease, vs the number that have been heard from that report taking HCQ and then getting Covid.
But it is very obvious that most people who have these conditions have not volunteered their information.
It is unclear why anyone would consider this a useful way to determine infection rates.
I agree with you when say there is a difference between what is being compiled.
The BMJ study is very clear on how the data is sourced.
After a call went out for patients to enroll in a worldwide registry, those who responded were contacted through their doctors, who supplied the information that was compiled.
So they are not trying to make any observations of overall infection rates.
What they are doing is looking at the set of people that have enrolled in the registry, which was voluntary.
They then separated out all of these individuals who had contracted COVID-19.
It was not limited to lupus patients.
It was limited to all people with what is classified as a rheumatic disease.
This is a group of diseases with certain aspects in common, and for whom the same types of medications are often found to relieve symptoms.
They are regarded as incurable and lifelong conditions, often progressive, sometimes severe, sometimes mild. Typically with recurrent flare ups and then remission periods of more mild symptoms.
These diseases are disorders of the immune system.
Some have called them autoimmune diseases in the past.
But the understanding and the description of the etiology has evolved and become more refined over time.
That phrase is not as commonly applied any more.
In any case, there was for some reason a focus on lupus patients in the online scuttlebutt regarding these people.
I think we should look at the whole set of these patients and not focus on one subset of them.
Because what was germane to the topic at hand was that we have a population who have been on long term courses of the medications we now need to know more about.
In other words, there is not any obvious rationale to only consider lupus patients, and not all people who were already taking these drugs when they got COVID.
In any case, whether we look at them all, or just the lupus patients, we have individuals who were on HCQ, and others who were not.
Some of them were taking these other drugs.
Since what we are concerned about is COVID and what helps and what may help and what is not being shown to help, we should look at everyone in the set of patients, and later we can decide who and what medications are relevant.
Cast a wide net, and then sort the information.
So this comparison in the BMJ report is not answering the question of “How many lupus patients got COVID?”
It is looking carefully at people who took one or more of these group of medications, and other people who did not take any of them but who had the same underlying conditions.
We can now compare lupus patients who took a malaria drug and then got Covid, to lupus patients who did not take a malaria drug and then got Covid, and examine the data for similarities or differences in how they fared upon getting the disease.
It seems logical that this methodology has a good chance of eliminating self reporting biases.
We do not need to know how many people have these conditions all over world, what the underlying rates of disease was in those places, etc. That gets cumbersome and impossible to parse right out of the gate.
For one thing, people with these diseases, particularly lupus, are known to be very careful about avoiding sick people…they are very susceptible to infectious diseases because they are on immunomodulating drugs.
i.e., they take drugs that shut down part of the immune system.
When they get sick, it is often very much worse for them than a healthy person.
Which one of the usual suspects who defend science consensus will say this study doesn’t mean anything?
Yes there does seem to be a divergence of opinion on several areas of scientific doubt where the consensus follows the government money which follows the establishment opinion. Epicycles anyone?
Goldstein, did you know that a survey of climate scientists proves nothing about the climate?
Climate scientists live in a virtual world playing with numbers. Doctors actually heal people. Real world results are hard to argue with, but you’ll try.
Polls and surveys said Clinton would win in 2016.
icisil
Get real! Results have to be turned into numbers that are impacted by confounding factors such as demographics. The only way you get around that is by stating “I know a doctor who claims he has cured people.”
I wrote a post earlier… you’re talking past each other.
Yes, numbers are great. But when no one will do a true double blind placebo based study (and it’s been months now) due to politics… and while the studies that have been done use bad data… or use the drug in a way it is KNOWN not to be effective, we are left to use our common sense.
That is, it appears that taking a safe drug at a low dose has nearly zero downside risk and is shown to dramatically reduce effects of the virus.
Meanwhile, people are dying and we are arguing past each other.
CS, the only thing that matters is that people don’t progress to serious illness. How do you rationalize the Texas doctor treating his infected nursing home patients with HCQ, and the vast majority did not get seriously ill or die? That is a highly unusual occurrence in that context, or demographic. To say that is meaningless is meaningless.
And is indicative of Clyde’s manevalent ideology, icisil.
Clyde,
Oh, yeah?
Well, my niece’s teacher’s cousin’s step father heard that there was a person who once knew a doctor who said he never heard of that happening.
This confuses me. if there are lots of doctors who consider HCQ as being an appropriate treatment, why is the literature FULL of studies showing it to be of either no value, or positively harmful?
if the answer is that politics is driving these findings rather than dispassionate science, then I am all adrift – because I cannot then believe ANY published finding – either supporting or refuting this drug….
Look at the protocols of the different studies, you see why there are diffetent outcomes.
Late use versus early use, as so often discussed here, but my impression is, shortage in remembership seems to be mainstream here.
Why would you listen to anyone or anything that is not actually healing patients? If doctors say HCQ is helping their patients, why would you not at a minimum consider what they say is true?
Because I have been lied to frequently before. And the result of being lied to by authoritative figures is to make me suspicious of ALL authoritative figures – not just the ones I disagree with…
Yah, but not everyone’s a liar. The flux lines of this epistemological exercise tell me that many independent, highly skilled practitioners are reporting a benefit from personal experience, whereas many establishment voices with conflicting interests are trying to find fault without anything but the usual framing and manipulation of data. What does each have to gain and/or lose?
Speaking of conflict of interests
New Docs: NIH Owns Half of Moderna Vaccine
https://childrenshealthdefense.org/news/new-docs-nih-owns-half-of-moderna-vaccine/?itm_term=home
Probably late to the game, but read this article about the Gilead/Boston hospital test on Remdesivir / the Lancit report on HCQ, and the complicity of the CDC.
https://www.lewrockwell.com/2020/07/no_author/lancetgate-scientific-corona-lies-and-big-pharma-corruption-hydroxychloroquine-versus-gileads-remdesivir/
personally, I think it boils down to free choice–if I want the Remdesiver and can pay the price, the doc should provide it. Same with the HCQ+ zinc. My body, my choice…
This is a poll dated April…early April.
Worthless.
Who cares what people thought back then?
Get current opinions from the same people and see how it has changed.
Besides, the people that matter are not a survey of random doctors, but the ones that work with patients in critical care situations.
Back around then my very busy doctor told me he had yet to get back a single positive test result.
You have it backwards. The ones to listen to are the ones who can keep patients from progressing to critical care. I think the general consensus is that HCQ doesn’t do well for critical care patients, so why would we listen to critical care specialists about HCQ?
Follow the money Geezer. Treatment cost of HCQ–about 7 dollars. Treatment cost with Gilead’s remdsiver (sp?) about 2400 dollars. Ask about the financial ties to Gilead certain CDC officials have among others.
Rolling a patient on their side (prone position) is an effective treatment for low blood oxygen. How much does that cost?
I would prefer to be treated before I need to be rolled 😉
Lucky you. Every time I need to be treated I get rolled ($$$$$)
So thats how its done…
Wit is not your strong suit, Loydo.
“Ba-dum-tsss,” yes, sarcasm, no.
https://www.youtube.com/watch?v=6zXDo4dL7SU
xoxo
My opinion, exactly.
“Follow the money Geezer…”
Oh, that certainly makes me suspicious of Remdesivir. But it tells me nothing about the efficacy of HCQ. And the more people offer that kind of argument, the more suspicious I get about ALL the trials…
I think that, as a society, we have successfully undermined Science. I suspect that social media has had a large part to play in this – allowing the worst tribal instincts of humanity free play….
Good doctors are not scientists; they are healers. Beware the doctors who are only scientists.
He is flat out lying about the price of remdesivir.
It has been established that 5 days is as good as 10 days.
1 vial will cost $320.
But no one has bought any yet.
Gilead gave away the entire supply in existence, and since it takes 6 months to make a single dose, they are not yet in possession of any to sell.
But, it will be ready soon.
Trump has secured the entire supply for the US government, through to September production.
By December they think they will have made enough for a couple million people.
It saves 5 days off of an average hospital stay.
That translates into a $12,000+ savings per patient.
Every jackass who refuses to get it will cost us all a big fat pile of cash.
Meanwhile, hundreds of clinical trials are ongoing, in every country, and every state, and almost every large and medium size city. Meaning it is free.
Trials for other drugs vs standard of care will now mean other drug vs remdesivir.
IOW…no one will get placebo anymore in any trial.
It would be unethical.
SoC is remdesivir.
I seem to recall everyone is supposed to have insurance.
And also that the government has said no one is gonna get charged for any treatment related to getting COVID.
Did that get rescinded?
Go to any business news site and enter remdesivir in a search, and this info will be there.
Except the clinical trial parts…go to clinicaltrials.gov for that info.
Any day now, Gilead will begin clinical trials for an at home inhaled version of remdesivir.
Anyone who thinks they have the virus can get it for free in any one of many clinical trials, or another usage called expanded access…all free.
In fact, clinical trials pay participants for their time.
Many of the trials are giving remdesivir and another drug.
I would enroll in remdesivir plus the anti-IL6 drug trial, if I had it.
Here is a link set up to go directly to the 40 trials with remdesivir.
They added one since yesterday.
Number 11 on the list is remdesivir plus Tocilizumab (anti-IL6 monoclonal antibody)
But what do I know, I am just a moron troll.
Oops, the link…
Here it is.
Number 11
https://clinicaltrials.gov/ct2/show/NCT04409262?term=remdesivir&draw=2&rank=11
How can Remdesivir be the “standard of care” when it is virtually brand new and nobody knows what side effects may be waiting. There have been no proper trials over any time period of about 6-8 months as it was only rushed out of development last year. (that is my understanding, sorry if anyone can correct me).
The main claim for remdesivir seems to be as you said – reducing hospital stays by about 5 days. Knowing it is usually used for more serious cases, does this mean that patients die sooner? Statistics can be used in many ways!
One can stand up and say trial this, trial that, studies show etc. but this is a situation where people are dying in significant numbers and many within two or three weeks of realising they are ill.
In this situation I am for going early with what are impressive results with HCQ and Zinc sulphate and including azythromycin if there is indication that pneumonia infection is present (although it may be late in the day for best results in that case). Obviously under a doctor who can check for possible heart contraindications.
The pushing of remdesivir, given the complete lack of long term safety and underperformance v. HCQ etc seems highly irrational.
The cost comparison also raises concerns of propriety in my mind.
SteveT
The notion that “big pharma” would let much of its current and future customer bases die-off on the odd chance that one of them would come out a with a new COVID-19 treatment is not following the money. They’ve lost lots of seniors and future seniors with 3-4 scripts. Remdesivir is a $1B development. They’ll make that back by the end of Sept if things go ideally-well. If not, then the future of the drug is uncertain. And everyone else besides Gilead was a loser in wasting research money but not hitting it big.
One of the most disgusting aspects of the COVID pandemic has been the ruthless jockeying by drug companies and their agents to push their own drugs and actively bad mouth possible competitors without regard for the good of the public.
Dodgy
You asked, “… why is the literature FULL of studies showing it to be of either no value, or positively harmful?” It is the same reason that about half of peer-reviewed, published studies can’t be replicated in the medical field. That is why large samples of random subjects have to be used, and confounding factors such as co-morbidities have to be accounted for. Early results from ad hoc clinical trials, with a disease that a large proportion of those infected have mild to no symptoms, used only in the early stages, should be expected to have good results. That is why so many different drugs appear to have some efficacy. What is even more critical is that those not in need of hospitalization, or just some palliative care for a few days, are not the important ones. It is those, for whom HCQ is not recommended, that are most in need of effective treatment. At this point in time I wouldn’t give much credence to any of these early ‘studies.’ It is understandable that a physician who can monitor his/her family members would, out of desperation because of the lack of alternatives, consider prescribing HCQ if a family member showed signs of possible COVID-19. If they get well, it might have been HCQ or it might have been an inherent resistance to the virus. It is like the drunk blowing a whistle to keep the pink elephants away. The real test is if people who are seriously ill can be cured. Anything less is Witch Doctor medicine.
BS, Clyde. The severely ill are dying at prodigious rates NOW, no matter the treatment! The real test is to find out how to keep people from becoming severely ill. Your ideological stance is ugly. F**k off.
P.S., Clyde. With my recent diagnosis of WuFlu, this is personal now. So, again, F**k off, Troll.
In reply to ‘Dodgy Geezer’:
Dodgy, look at motive. Who win and Who would lose to hide a very effective Covid treatment from the American people?
If people are lying, trying to hide a very effect Covid treatment, that is criminal/an attack on the US people and the lying needs to be called out. Particularly as this appears to be organized lying.
Six US Michigan Hospitals, financed by the Henry Ford foundation are not going to lie about the fact that 2541 patients….
….Treated with HCQ/AZ plus zinc within 48 hours of admittance to the hospital …
(that is not early treatment, that is earlish treatment, a doctor in New York treated 500 of his patients as soon as Covid symptoms were detected, his results is a reduction in the covid death rate by a factor more than 10.)
….were 71% less likely to die of Covid, as compared to the patients that did not get the treatment. Interesting there was not a single heart attack in the treated group, while one Fake HCQ study alleged that 25% of those treated with Covid died of heart attack and there was a reduction in outcomes for the HCQ treated patients.
Dodgy Geezer, science stops working when organized paid groups of people have agendas and lie and take over the media. This is different than a single incorrect study.
We do know that the Lancet study that lied and that presented false data has been withdrawn….
We also know that company that supplied the data for that study has refused to supply source data and is not returning phone calls.
Science also works because there is only one correct answer. A group of doctors in Michigan are not going to lie about the effectiveness of HCQ. There going to do what they are told and they are going report unfiltered results.
Six different hospitals, Michigan hospitals treated 2541 patients and their evidence based results are….
Early treatment of Covid patients (the earlier the better) with Hydroxychloroquine and Azithromycin plus zinc reduced the covid death rate as compared to untreated patients by a 71%.
https://www.ijidonline.com/article/S1201-9712(20)30534-8/fulltext
Treatment with Hydroxychloroquine, Azithromycin, and Combination in Patients Hospitalized with COVID-19
Results
Of 2,541 patients, with a median total hospitalization time of 6 days (IQR: 4-10 days), median age was 64 years (IQR:53-76 years), 51% male, 56% African American, with median time to follow-up of 28.5 days (IQR:3-53).
April?
It is now July.
Might as well look at polling data to help decide about an election.
In the world of climate skepticism, we regard people who try to reason by citing surveys as the most unscientifically minded people in the arena.
This is no different.
Data from polling two months ago has zero weight, and can even be taken as obviously biased, towards when less was known.
Look at how the Henry Ford Health System data was skewed by a sequential survey of patients.
Indeed July, but 2020, not 1520 😀
It’s a world of difference. One is an abstraction that has nothing governing interpretation; the other is the personal appraisal of highly skilled professionals.
Salute!
c’mon, NickMc…..
I do not recall the cosmic “peer(brotherin law) reviewed, double blind, clinical trial that resulted in the FDA to recant on emergency use of the malarial drugs.
All we got to use is testimony from many practitioning doctors and what they did and what seemed to work.
Wanna do a serious study of HCL and its “helpers”?
How can we round up few thousand folks of all races and colors and blood types and underlying medical conditions and then expose them all to the bug in very controlled environmental conditions and then separate the infected from those that did not seem to suffer? Then we examine all kindsa things for both groups, but we start a HCL+ regimen on the infected ones. Then we look at those poor souls for blood type, race, underlying conditions, etc as we watch them die or recover. And how many had heart rhythm problems or whatever that can be traced to the HCL? Guess we should have also taken another thousand off the street with no Corona problem and had them take the HCL like I did not of my own free will years ago. How many of them died or had debilitating problems compared to Advil or the myriad of drugs advertised on TV for problems most people might have and didn’t have the problem from the guy in front coughing?
My not so humble opinion is the FDA caved to the deep state and ignorant, politically motivated mass media.
As with thousands of ads on TV, all the FDA had to do was include that famous line at the bottom of the screen warning about side effects that may occur in a very tiny of people, and relate that to the veteran numbers of we millions that ingested the damned HCL for years and croaked.
Gums rants….
We should read HCL as HCQ, because HCL is somewhat differnt, isn’t it ? 😀
I have no idea what you are trying to say Gums.
What I am saying is very clear: April was three months ago.
Since then a lot of new information has come to light.
Since then many more people have been treated.
Those polls are still being done, so why not report the up to date ones?
Who wants to guess what they say?
I already checked.
Salute!
No problem, NickMc
I am trying to make the point that there has been no super duper study or trial that makes taking the malaria prophylactic some kinda death sentence.
The malaria compounds have been used and studied for eons.
As with all the new, magic drugs advertised on every TV channel three times and hour, its warning would be that only 1 person in 100,000 might have indigestion, and anyone with an existing heart problem and high blood pressure should consult their doctor ( do not know how you got the HCL without seeing your doctor, but gotta put that in the add to mitigate lawsuits).
That is my point Nick.
The damned malaria stuff seems about like Advil, and should be treated the same.
If the stuff helps, then great, but the FDA and certain media should not discourage its use as long as the warning we find on every label states that the efficacy has not been proven to CURE covid-19 and that no other compound has been proven to cure the virus attacks upon your body.
There is a lotta difference between asserting some chemical or drug will CURE a disease versus suggesting a possible use of an existing compound that has been thru the rigorous testing to get approval by the FDA for widespread use without special scrutiny.
I do not find an assertion that HCL plus other stuff could cure the corona virus attack. All I can find is that it MAY reduce the severity or shorten the problem.
back to the bbq, as the damned critters can not fly and don’t smoke or heat or breeze.
Gums sends…
Gums, please ‘send’ your location; I’m hungry.
There are still more than 100 studies enlisted for HCQ in the U.S alone at the moment, other countries are doing trials as well, so I guess at some point we will have sufficient data for one or the other outcome.
Disclaimer: I would really like to see a comparison Zn alone/HCQ alone/HCQ+Zn.
RE: “Look at how the Henry Ford Health System data was skewed by a sequential survey of patients.”
Please provide evidence for your allegation. Weren’t you the one dismissing Leo’s submission and touting a ‘sequential’ survey of doctors opinions. Memory refresher: “Get current opinions from the same people and see how it has changed.” D’OH!
Do as I say, not as I skew?
Your concern about the upcoming election is noted, St. Nicholas.
Unfortunately, doctors can be extremely close-minded, especially with anything that might go against their training, and anything smacking even remotely along the lines of preventive and/or natural or non-pharmaceutical. I realize a lot of that is to protect themselves from lawsuits, but it means that it can be difficult to accept what they say at face value.
Bingo and the winner is McGinley!
I should have put money on it.
I didn’t even question that, clear as clear water is who will be the winner 😀
Yeah, I am pretty sure he’s one of are old time frauds, Brandon Gates, Griff, Tony Mcleod or one of the other name changing frauds, the writing style is familiar i just haven’t put my finger on it yet but I will.
boder
I don’t see the similarity in the writing styles. Ask Anthony if they are the same people.
I am pretty sure you are a jackass, Boder.
Gates does not come round here no more.
Last time he was here was the time I argued him straight into a tonic-clonic seizure.
I am not sure when that was…
After this time I pantsed him and stole his lunch money:
https://wattsupwiththat.com/2015/04/26/inquiry-launched-into-global-temperature-data-integrity/
Last time I saw Tony, was that time he lost a $1000 bet with me, that every one here witnesses, regarding his inane opinion on Arctic sea ice.
How do I know you are not him? He was nearly as unpleasant as you, so I am suspicious…
Do not think I am forgetting about that money, Tony!
Alright, you caught me. It is I and he is me.
It was fun while it lasted . . . 🙁
Speaking for myself, I am way too quick and nimble for him to ever gets his greasy fingers in me.
I have to take a shower.
OT — when I get a severe illness, I have a symptom that hasn’t been discussed — severe whining (at least that’s what my daughter says). Will hydroxychloroquine control that symptom?
BTW, I had a dental appt. scheduled for this afternoon, and I got a call from the dental office saying they cancelled it because my dentist wasn’t feeling well. I asked about covid-19, and the staff told me they don’t know — he’s going to be tested for it — and this is the second time he’s been tested. Earlier this year, one of his dental hygienists quit, because she was paranoid about catching covid-19. We talk a lot because my family has been going there for over 30 years. And dental problems is one of my major malfunctions, and I help them stay in business.
Here’s a HCQ study published a few days ago, for what it’s worth, conducted by a Detroit area hospital system. Death rates between HCQ treated vs. non-treated patients. HCQ cut death rates . Their results indicate early treatment is needed for effectiveness.
https://www.henryford.com/news/2020/07/hydro-treatment-study
+42^42. Old military saying: When in doubt, whip it out. The HCQ+, that is. Was diagnosed with the ChiCom virus’ WuFlu yesterday evening after developing symptoms a few days ago. Will be contacting my primary care Dr. this afternoon. Will certainly demand HCQ+ treatment. Will go outside the VA if necessary. F**k St. Nicholas.
BTW, it was in fighting the Asian Marxists that I got my combat wounds, which wound up prepaying my healthcare. What goes around.
Never deal with societies that follow Marxism, eat weird wild animals, live in close proximity to pigs and ducks and unhygienically slaughter animals in inner cities. Whatever the costs, limit Chinese travel, move manufacturing of most things back to the USA and destroy the ChiCom monster economically as well as militarily.
God bless you for your service:
I will hope the your last sentiment is never to be needed, having to use our military, except as a show of strength by being strong… Get well fast and let us know how you are doing with treatment.
Our Nicholas comes more than once a year, unfortunately.
Not suggesting attacking the ChiComs, just containing.
That’s a great clarification… Your posts are inspirational…
Thank you for your sentiment, Mario. I’ve been called many things when dealing with numerous controversial business and political issues over the decades, but inspirational is a new one! When opposing popular (but bad) ideas, the most common description was antisocial asshole.
Sadly, the Woke brigades don’t want to listen to reasoned experience. It will take at least another generation for the inexperienced (and those who won’t read history or who actually misinterpret history) to make enough mistakes to learn the lessons of history and the bad outcomes of good intentions. Humans are not perfectable; centralizing power to force perceived (usually political or religious) perfection always turns out badly. Democratic free markets usually shake out the bad ideas; not perfectly, but better than anything else.
Ideological movements always eat their own. The currently pervasive cancel culture, made more toxic by technology, is now dragging down its own idols of old. It will continue to drive society into waring camps and it will not end well for the common man. E Pluribus Unum, the motto of the US, is the great idea of American democracy. Tearing it down will destroy us.
Amen that Dave. I learned later in life why I was usually the one taking a counter view to many arguments… and that realization was eye opening to me. You speak cogently, and sound fortified with experience when you counter in an argument. It shows.
Since HCQ is a prescription drug let’s look at OTC.
IF one of the reasons HCQ works is because it is a zinc-ionophore allowing zinc to go inside the cells from the bloodstream, there are a number of OTC products which are zinc-ionophores. The one I take, along with a Zn supplement, is Quercetin.
I’ve been doing the same. Quercetin is found in red apples and other food stuff. I’ve been eating an apple for breakfast for years now–apple a day keeps the dr away. I read about the need for zinc in a healthy immune system back in Feb. and started that supplement then, along with upping my Vit.C &D. added the quercetin supplement just recently as I figured the amount in a single apple wasn’t all that much, and what the hey–doesn’t cost very much, and assume that the VA won’t be prescribing HCQ as a preventative anytime soon.
Never get a flu shot, don’t use anything that brags on killing 99.9% of germs, and the only issue I have is some mild seasonal allergies. Got all the health conditions associated with my age (74), but never get sick, and intend to keep it that way with a strong and healthy immune system –not vaccinations.
John, the Dutch have a saying:
A herring a day keeps the doctor away. Two herrings a day keeps everyone away.
And the Finns – a 20-year fermented herring empties the entire block, pronto.
Still, I wonder if anyone has checked the vitamin content of fermented herrings. I’ll bet we are in for a surprise!
Elderberry is highly effective against human coronavirus NL63, one of the three known
coronaviruses to enter cells through the ACE2 “back door.” It directly stops the attachment of
the virus to ACE2, so probably does the same for the new coronavirus as well. Since viruses
need to hijack our cells in order to multiply and spread, and since if they don’t do that they
eventually die, blocking the entry of the virus into the cell destroys its ability to multiply, spread,
and survive.
Elderberry’s effects aren’t limited to blocking the ACE2 back door. It also destroys the lipid
envelope of avian infectious bronchitis virus, a coronavirus that infects chickens and other birds,
and in humans it is effective against the flu, which isn’t a coronavirus at all. None of these
viruses enter cells using ACE2. Still, its ability to directly block the use of ACE2 as an entryway
means it has the potential to nip the new coronavirus in the bud and prevent it from ever
establishing an infection in the first place. As a result, it deserves a place as a preventative and
first line of defense against the new coronavirus.
And your mother’s breath smells of Elderberry wine! An old bad joke, Don.
Hi ‘don rady’,
Hey Don, please do not make stuff up. Elderberry is not highly effective against Covid.
Regardless of sex or age, Vitamin D normal people, blood serum 25(OH)D levels less than 20 ng/ml are 19 times more likely to die from covid than vitamin D deficient people 25(OH)D blood serum levels less than 30 ng/ml.
Researchers know that because they measured the 25(OH)D levels in the blood.
4000 UI/day per person is required to raise the US populations 25(OH)D levels above 30 ng/ml.
82% of the US black population, 69% of the US Hispanic, and 42% of the US general population is Vitamin D deficient.
Prevalence and correlates of vitamin D deficiency in US adults.
https://tahomaclinic.com/Private/Articles4/WellMan/Forrest%202011%20-%20Prevalence%20and%20correlates%20of%20vitamin%20D%20deficiency%20in%20US%20adults.pdf
4000 UI/day of Vitamin D supplements is required to raise the serum 25(OH)D of the entire population above 30 ng/ml.
https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3585561
Patterns of COVID-19 Mortality and Vitamin D: An Indonesian Study
Vitamin D Insufficient Patients 12.55 times more likely to die
Vitamin D Deficient Patients 19.12 times more likely to die
It is interesting that chemical ‘Vitamin’ D actually changes our body at a cellular level.
The cells in people who are Vitamin D normal have upgrade changes at a cellular level which are made to enable our body to stop internal inflammation and hence all common cancers, to increase the core body system strengthening the spine and warming the core (this explains why people lose 20 to 40 lbs when they correct their Vitamin D deficient and why some people are clumsy)…
… Vitamin D also actives a system that protects the brain… which explains why Vitamin D deficient people suffer long term brain damage. Their IQ is actually lower. Very sad and hidden from those most affected.
For Vitamin D status, cases were classified based on their serum 25(OH)D levels:
(1) normal – serum 25(OH)D of > 30 ng/ml,
(2) insufficient – serum 25(OH)D of 21-29 ng/ml, and
(3) deficient – serum 25(OH)D of < 20 ng/ml.
Ehm, vaccinations are way more likely to boost the immune system than the opposite so that doesn’t make any sense at all. That is actually where possible side effects are originating from and why there is the hypothesis about TBC vaccination and protection from SARS-CoV-2 in the first place.
EGCG is another, and is probably better absorbed than quercetin.
Zinc ionophore activity of quercetin and epigallocatechin-gallate: from Hepa 1-6 cells to a liposome model
https://www.ncbi.nlm.nih.gov/pubmed/25050823
The liposome assay would actually be the gold standard to prove any ionophore property of HCQ.
As one can see from the 3D structure for quercetin and epigallocatechin-gallate both fulfil the criterium of negatively chargeable prosthetic groups in close proximity to work as an ionophore for divalent cations:
https://chem.nlm.nih.gov/chemidplus/structure3D/viewer/117-39-5
https://chem.nlm.nih.gov/chemidplus/structure3D/viewer/989-51-5
It would be very informative to test these in cell culture against SARS-CoV-2 replication for the Zn hypothesis. Or clioquinol as this is not known to have antioxidant properties that could confound any finding but is a well established Zn ionophore.
Ron: This from a MedCram shows a chart at 7:50 into the video:
@mario lento
Yeah, I know but nobody really tested it with the virus AFAIK yet.
Quercetin is somewhat “problematic” in this instance cause it has a lot of other potentially beneficial effects in the context of a viral infection…
– antioxidant
– anti-inflammatory
– autophagy-inducing
etc.
… though the data is not completely uncontroversial.
So to prove the action is through an ionophore effect it would be better to use another ionophore with as less as possible off-target effects.
Oh, yes, I was just showing a chart which claims observation ionophore activity of several substances.
quercetin does seem to help with tamping down (I will use the term misguideded) macrophages so it helps in autoimmune (allergies) disease. What I do not know is if it suppresses all immune response or selectively reduces improper immune response.
I was taking Quercetin + Zinc gluconate daily until I got a script for HCQ. I’ve convinced my wife to take it.
In case of Zn deficit, eat oysters ! 😀 😀
Vegans should eat wheat germ, at least 😀
Oysters only work with Guinness. Many a festive proof of that. They get their oats in volumes!
An uncle, MD, surgeon, swore by it.
Krishna: [this is personal] I have been taking a Saw Palmetto prostate formula which has pumkin seed, and recently I found it had 15mg of Zn per capsule of which I was taking three times per day for some 4 years. It works great for flow.
I also had been taking Ca/Mg/Zn w/D because it’s a good mixture of minerals. (I take lots of other supplements and powdered juiced veggies).
So I recently reduced the dosage of both of these products since I don’t want to be taking so much Zn…
I think that taking 30mg Zn/day is still a bit over the top still…
Anyway, after I started taking 1500mg day of supplemental Quercetin, with NAC, I noticed my lungs (exerciser induced bronchitis) and sinus sensitivity vanished.
It seems the Quercetin brought everything together for me…
Over the years, I used to get sick for weeks and then feel crappy for months. Over the past 4 years, when something bad goes around, I either miss it or get it for a couple days…
With the Quercetin, and EGCG I am sort of looking forward to the flu season to test out my immunity… Oh, and my Vit D is 62ng/mL with K (I do not supplement K) is off the charts >2,500pg/mL
Grumpy
One of the common arguments for the use of HCQ is to make zinc more readily available to the body. Many people are convinced that using zinc gluconate is effective in aborting viral infections that cause colds. If an ionophore is necessary for the bio-availability of zinc, why isn’t it included in the OTC zinc gluconate? Even allowing for the fact that zinc gluconate might be more effective in conjunction with an ionophore, it appears that sufficient zinc can be acquired to be effective, even in the absence of an ionophore, without becoming toxic. A lot of hand waving to rationalize something that may or may not work for COVID-19. I remain agnostic and await high quality trials.
“I remain agnostic and await high quality trials.”
Meanwhile 4 months have gone by and potentially, 70k fewer deaths at no risk by not waiting. It’s called being pragmatic.
+42^42, Mario.
Clyde Spencer:
I am also somewhat agnostic. But, my thinking is that Quercetin is cheap, and the zinc gluconate is free through my health plan, and the combo is doing no harm, so why not take it…
Just be careful with Zn… some is great too much interferes with Cu balance…
Where are you finding a zinc supplement? All the pharmacies and supermarkets around here have been out of stock since February.
Been buying my supplements at a local “health food” store. Costco on line or amazon should work also.
Online at Walmart and Amazon. Some items ship free by themselves, but most everything does with $25-35 order.
Yes, also EGCG, in green tea, so I add green tea extract. I am careful now not to overload on Zn because being in balance is also important. Cu competes with Zn and is also crucial to a well functioning body.
Yes, the article relies on surveys, and some of them go back in time. But the published information is mounting in support of HCQ+. And the efficacy is proving out both pre- and post-exposure. Diagram showing HCQ role in relation to disease stages:
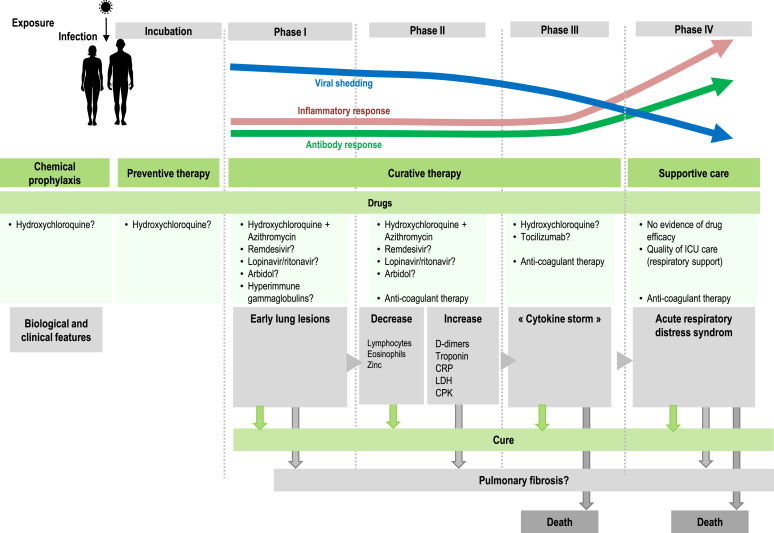
Previous posts provide examples of HCQ treatment along with other proven medicines (eg. Azithromycin) and supplements (eg. Zinc. vitamins C and D). Summarized in the chart above is the role of HCQ+ according to the progression of the disease Covid19.
HCQ Prevents Covid19
The first column on the left is sometimes called PrEP, or pre-exposure to the virus SARS CV2. Now we are getting studies confirming that HCQ plays an important prophylactic role in blocking the virus from taking hold when someone is infected. The Times of India June 19, 2020, article is HCQ beneficial as preventive drug: SMS doctors told ICMR.
https://timesofindia.indiatimes.com/city/jaipur/hcq-beneficial-as-preventive-drug-sms-docs-told-icmr/articleshow/76453826.cms
My synopsis: https://rclutz.wordpress.com/2020/07/07/hcq-proven-first-responder-to-sars-cv2/
Conclusion: 11% of American Doctor respondents had severe TDS.
So, having a personal physician that suffers from TDS should be considered a predisposing condition (a co-morbidity of sorts)…increasing the likelihood of death by Covid-19.
Trump was right…. which only makes the TDS afflicted even more irrational and irate.
Am I right in thinking that the majority of the anti-hydroxychloroquine propaganda originates in the United States?
Nope, it’s a global phenomena: https://www.marketwatch.com/story/who-formally-drops-hydroxychloroquine-hiv-drug-from-covid-19-drug-study-2020-07-06
Please note that the WHO (ChiCom) study was for severely ill WuFlu patients only. Propaganda is always carefully worded. Such leftist/Marxists propaganda is particularly effective on the susceptible like St. Nicholas.
HCQ+ is recommended for prophylaxis and early symptoms’ treatment only. Once one hits the hospital, outcomes are primarily random and depend on one’s personal characteristics.
Thank the Donald for getting us out of the WHO. Also, F**k the UN and all its subsidiaries such as the IPCC, UNESCO, etc.
HCQ fails at prophylaxis: https://www.newsmax.com/health/health-news/hydroxychloroquine-trial-covid19-study/2020/06/04/id/970477/
Henry, your severe TDS is on display; you failed to reference a follow-on study that debunked your citation. All you had to do in scroll down your article to find the follow-on study. Propaganda is ugly. You are ugly; screw off, twit.
Well done. Henry, like the LEFT, will erase history to change outcomes. They seek a predetermined outcome, not truth. So sad.
Political ideology is ugly, Mario. The Democrat Left is willing to kill thousands to put a demented old man in as President of the US. At times, I am tempted to believe that the long-term health of America’s democratic free market experiment needs a good dose of short-term Marxism/Socialism government insanity to remind liberals of how we got to be the most successful democracy on the planet. Without a supermajority Senate, they might not do much long-term damage.
I hate to admit, I fantasize about that.
But guess what. Trump is allowing, and I say that thoughtfully, allowing the Democrats to reveal themselves. He could clean up the cities stat. But then the media would pull a Simon or a Henry, and say Trump is a fascist against mostly civil protest. So let them suffer their consequences. You don’t hear anymore calls for Gov Cuomo as president after his (let’s call it neglectful homicide) murdered old people. He initially tried to blame everything on Trump, who over delivered.
So, Trump is handing over the Marxist to those who vote for it.
We can see where all the carnage is.
Trump is so brilliantly owning the libs, that they take the bait.
America is Watching…
PS – My full name no spaces, at gmail is my personal email address.
OK, Mario. I’ll be in touch. Watch your back.
Yes sir! Meanwhile Nick the Mck is making up stuff about me, out of whole cloth, which is evidence he has nothing. He’s been exposed…
Mr. Fair, the drug does not prevent COVID-19. The drug does not cure COVID-19. There are now well over half a million deaths attributed to the virus. The drug has failed to help anywhere in the world so take your “TDS” and shove it you know where.
Henry, since I never said HCQ+ prevents or cures the ChiCom virus nor its resultant WuFlu, I surmise your reading skills are on par with your reasoning skills. Since there are worldwide studies showing the drug combination has helped numerous people possibly avoid an ugly death, you are either ignorant of that fact or a liar.
Again, since my diagnosis of WuFlu, I have no sense of humor left in dealing with obvious Trolls like you. I will take HCQ+. If you catch the ChiCom virus and develop the WuFlu, get back to us on WUWT if you change your mind about taking HCQ+. Until then, I heartedly suggest you F**k off; you have no idea as to what you are talking about and could mislead the gullible.
P.S., Henry: My anger with you and your ilk is showing up in my comments on WUWT. It results in them being thrown in temporary moderation, slowing my responses. Anyway, you are still a twit, no matter the trouble I get into with the Moderators.
Mr. Fair, this virus is not political. This virus doesn’t care about socialism nor does it care about capitalism. This virus is a global phenomena. India is the largest manufacturer of HCQ, and it’s case load is growing very fast. There is no “TDS” in India, so tell me, how come the physicians in India haven’t stopped this virus with all the HCQ they make?
Either you don’t read or you can’t comprehend simple facts, Henry. Goodby.
Henry if you contracted Covid and your doctor prescribed HCQ + zinc would you take it?
If he/she didn’t prescribe would you take HCQ + zinc ?
If not what would you do?
Mr. David Fair…
.
.
Calling the virus “ChiCom virus” and the resulting affliction “WuFlu” betrays your lack of scientific/medical acumen. The proper name of the pathogen is SARS-CoV-2 and the resulting disease is called COVID-19.
..
When and if you start using the proper scientific and medical nomenclature, we can continue this discussion.
WHO Stop investigating HCQ.
Why does the WHO Stop investigating HCQ? Why is there fake HCQ research? Fake ‘research’ is sciency stuff written and published, to push an agenda.
Why was there a FAKE Lancet HCQ study that alleged that HCQ caused 25% of the covid patients to die of heart attacks and showed no benefit.
‘IT’ is the
The global phenomena ….. …..to hide the fact that early covid treatment, with low dosage HCQ/AZ plus zinc with reduces the covid death rate by more than a factor of 10 and reduces hospitalization by 84% with zero heart attacks.
We all know, that everything that the WHO, does is approved by China. No surprise.
It is a fact that China is the most powerful country (there are no checks and balances in China, people disappear, there is no defence) in the world and you are just a single person, from a small country, and you like the gravy train, what would you do?
From China’s standpoint, if the US takes years to find out that HCQ/AZ plus zinc reduces the death rate for covid by more than a factor of 10 and reduces hospitalization by 84%, if the treatment is started early,…
Then China wins and the US loses. All of the US loses. There is no left or right side, to US citizens dying and suffering needlessly.
The Lancet, editor Horton, is British. And they want Hong Kong back with Sen. Cruz doing his antifa cameo.
It takes years for Americans to notice that.
Salute!
Direct hit, COMMIE!
It appears, without peer-reviewed truth studies, that certain political tribes and many folks down in the swamp fear for their jobs and influence upon society, I opine.
All must realize that anything that comes outta the mouth or tweet of “orange man bad” must be countered or attacked.
No mystery why U.S. media and info has little info about other country failures and successes with malaria compounds that might actually help your cells to fight this virus.
Remember, the “science is settled”, so do not try any home remedies that have not gone thru three years of “clinical” trials.
Gums sends…
you know i like the Gums ……. part at the end its always good.
Commie B,
I always enjoy your comments.
Someone said somewhere on TV that hcl is broadly in use, well understood for treatment of other diseases, low risk, easily available, inexpensive and could work. He followed up with “what do you have to lose?” Simple logic, right?
That’s when the “new treatment” skidded off into the political ditch. The 97% scientists started blathering uninformed opinions. Governors started outlawing treatments. Federal agencies issued newly discovered warnings. Then it spread to other countries like an out of controlled virus. People started dying from TDS complications. Strange times.
TDS by Proxy
How many people did CNN kill with their scare mongering?
Somewhere I heard (so a statistical study is needed) that there has been a slight increase in deaths due to heart attacks because some people are afraid to get medical help when they first feel such symptoms because they have more fear of the corona virus. (Obviously such a fear would have to be inferred or obtained from a person who actually heard it from the now-deceased heart attack victim.)
A curious “paper”. No author stated up front; I presume it is Leo Goldstein. Publication status? Well, there is a note:
“Except for this paragraph, this paper appears here exactly as it was submitted to medrxiv.org on June 30 (MEDRXIV/2020/143800). It was rejected today, on July 4: “We regret to inform you that your manuscript will not be posted. A small number of papers are deemed during screening to be more appropriate for dissemination after peer review at a journal rather than as preprints.“”
Medrxiv is an unrefereed preprint server, so it is indeed one of a small number to have been rejected.
And so who exactly is recommending HCQ? Four surveys are quoted, but only one (Sermo W3, April 15) gives doctors rating its effectiveness. The survey claims 4016 respondents, but, it turns out, only 1337 have treated Covid, and of those only half used HCQ. And many speak well of it. But that is barely enough time for the results to have come in, since the article claims “It became instantly popular among physicians on March 20-21”.
Nick, sorry yo came in second to Mcginley— try again next time!
https://c19study.com/
The studies that have negative results have “late stage trial” or some similar phrase. Starting treatment late is known to fail so why are they doing it?
53 studies (32 peer reviewed).
The author’s name is directly under the heading.
I read this site because I believe climate change is exaggerated. I have no idea how it has become a forum for political discussion regarding the present administration and possibly the next one. Wear a damn mask and stick to the science.
+++++
1) HCQ+AZ treatment gives results within a week – and sometimes within a few days.
2) So, there are 1,337 C19 treaters, selected randomly, more or less. Half of them used HCQ, and majority of them consider it effective, very effective, or extremely effective. And what is on the other side?
Can you find a single doctor, who used or saw HCQ+AZ used for C19 early without positive effect?
3) Two studies of Sermo and the JC study asked doctors opinions.
Of course we could all line up to be guinea pigs in the fast tracked Moderna vaccine trial like this unfortunate sot did:
https://childrenshealthdefense.org/news/modernas-guinea-pig-sickest-in-his-life-after-being-injected-with-experimental-vaccine/
And why does the person who wants to vaccinate everyone with a vaccine he will make a killing off NOT VACCINATE HIS OWN KIDS?
https://www.uspoliticsandnews.com/why-didnt-bill-gates-vaccinate-his-own-children/
My SWAG is that they are fast tracking it and throwing caution to the wind because it will become a solution looking for a problem shortly.
The opinions of doctors regarding what treatment works is largely controlled by confirmation bias. The DES (diethylstilbestrol) story tells it all. DES is a synthetic progestin with prominent androgenic effects given to women who threatened to abort. Doctors swore by it for 17 years after it was proven in double blind trials to be ineffective. Then a cluster of rare nasty vaginal/cervical cancers started showing up in young women. Turned out to be due to in utero exposure to DES. Further investigation found that the women had histories of male level of activity in childhood and there was a large increase in the frequency of homosexuality. It is one of the classic pieces of evidence that hormones during early development alter brain development.
The point here is that a physician who has done something and sees a positive result attributes the result to his/her action. When the result is negative, it is attributed to the treatment being too late or the pathology to great. In the case of the WuFlu, it is apparent that virtually all people without gross comorbidities will recover. Thus most doctor’s experience is with survival. Therefore, whatever they did was effective against something the media kept saying was terribly lethal.
Doctor’s opinions are NOT evidence for much of anything. My big bitch is the quacks (consultants) who want to put my husband on drugs that reduce ‘cardiovascular events’ but do not decrease all cause mortality. All without considering what effects side effects have on quality of life. As with COVID 19, this is done by trying to scare the patient into submission.
The Swamp is fighting as hard as possible to hide this super good HCQ/AZ plus zinc early treatment data.
Why the heck is it taking the USA so long to start using HCQ/AZ plus zinc as the standard early treatment for Covid? Evidence based, scientifically sound decisions.
How many people have to die, of Covid, for Politics? Is there anyone on the Left that has the courage to speak for the people, rather than the PARTY?
When is the fake news and PBS going to report this astonishing paradigm changing data HCQ/AZ earlier covid treatment outcome?
HCQ/AZ plus, Zinc early treatment resulted in a 84% reduction in hospitalization as compared to the current standard covid treatment….
…. And a reduction in covid deaths, of more than a factor of 10, as compared to the standard treatment. MORE THAN A FACTOR OF TEN.
The earlier, treatment is started, the better.
This study and others shows, HCQ/AZ plus zinc drastically reduce viruses count.
If the virus does not replicate it cannot do damage. Giving HCQ/AZ plus zinc, to people after the virus has replicated does not help.
https://www.preprints.org/manuscript/202007.0025/v1
COVID-19 Outpatients – Early Risk-Stratified Treatment with Zinc Plus Low Dose Hydroxychloroquine and Azithromycin: A Retrospective Case Series Study
Therefore, the odds of hospitalization of treated patients were 84% less than in the untreated group.
One patient (0.7%) died in the treatment group versus 13 patients (3.5%) in the untreated group (odds ratio 0.2, 95% CI 0.03-1.5; p=0.16).
There were no cardiac side effects.
Some of them still have not accepted that Trump won.
Some would watch their grandmother die rather than concede that Trump is right.
Nah, Leftist will make sure that only OTHER people’s grandma would die. Take that to the bank… sarc/…
If in 2019, someone said, and I am winging it here:
“THE USA would lock down the country, prevent businesses from opening, arrest people who go out in the sunshine at parks or who go to church –while forcing infected people to go to be confined within most at risk populations against there will, all while instigating and endorsing riots and mass destruction, removing historic statues, painting Marxists slogans in front of City Hall, Trying to pass mail-in-only voting, while at the same time devising fake medical studies to scare people away from treatments of a disease”
One would be right to respond: “Tinfoil Hat Conspiracy Theory”
Yet, here we are.
Leo Goldstein,
Thanks! An informative retrospective.