UPDATE: A Covid-19 case correlation between malarial and non-malarial countries has been plotted by Dr. Roy Spencer, and the results are stunning – see below.
Encouraging news: three new medical studies show a commonly available anti-malaria drug known as chloroquine aka chloroquine phosphate is showing strong results against COVID-19 infections in both China and South Korea. Excerpts from three studies, including one published in Nature are below.

An Effective Treatment for Coronavirus (COVID-19)
Presented by: James M. Todaro, MD and Gregory J. Rigano, Esq.
In consultation with Stanford University School of Medicine, UAB School of Medicine and National Academy of Sciences researchers.
Translation by: Celia Martínez-Aceves (Yale B.S. Candidate 2021), Martín Martínez (MIT B.S. 2017)
Summary
Recent guidelines from South Korea and China report that chloroquine is an effective antiviral therapeutic treatment against Coronavirus Disease 2019. Use of chloroquine (tablets) is showing favorable outcomes in humans infected with Coronavirus including faster time to recovery and shorter hospital stay. US CDC research shows that chloroquine also has strong potential as a prophylactic (preventative) measure against coronavirus in the lab, while we wait for a vaccine to be developed. Chloroquine is an inexpensive, globally available drug that has been in widespread human use since 1945 against malaria, autoimmune and various other conditions.
Chloroquine: C18H26ClN3
Background
The U.S. CDC and World Health Organization have not published treatment measures against Coronavirus disease 2019 (“COVID-19”). Medical centers are starting to have issues with traditional protocols. Treatments, and ideally a preventative measure, are needed. South Korea and China have had significantly more exposure and time to analyze diagnostic, treatment and preventative options. The U.S., Europe and the rest of the world can learn from their experience. According to former FDA commissioner, board member of Pfizer and Illumina, Scott Gotlieb MD, the world can learn the most about COVID-19 by paying closest attention to the response of countries that have had significant exposure to COVID-19 before the U.S. and Europe.[1]
As per the U.S. CDC, “Chloroquine (also known as chloroquine phosphate) is an antimalarial medicine… Chloroquine is available in the United States by prescription only… Chloroquine can be prescribed for either prevention or treatment of malaria. Chloroquine can be prescribed to adults and children of all ages. It can also be safely taken by pregnant women and nursing mothers.”[2]
CDC research also shows that “chloroquine can affect virus infection in many ways, and the antiviral effect depends in part on the extent to which the virus utilizes endosomes for entry. Chloroquine has been widely used to treat human diseases, such as malaria, amoebiosis, HIV, and autoimmune diseases, without significant detrimental side effects.”[3]
The treatment guidelines of both South Korea and China against COVID-19 are generally consistent, outlining chloroquine as an effective treatment.
Specifically, according to the Korea Biomedical Review, in February 2020 in South Korea, the COVID-19 Central Clinical Task Force, composed of physicians and experts treating patients agreed upon treatment principles for patients with COVID-19.[4] In China, the General Office of the National Health Commission, General Office of the State Administration of Traditional Chinese Medicine as well as a Multi-Center Collaborative Group of Guangdong Provincial Department of Science and Technology and Guangdong Provincial Health Comp and the China National Center for Biotechnology Development have established effective treatment measures based on human studies.[5]
According to their research (reported in Clinical Trials Arena),
“Data from the drug’s [chloroquine] studies showed ‘certain curative effect’ with ‘fairly good efficacy’ … patients treated with chloroquine demonstrated a better drop in fever, improvement of lung CT images, and required a shorter time to recover compared to parallel groups. The percentage of patients with negative viral nucleic acid tests was also higher with the anti-malarial drug… Chloroquine has so far shown no obvious serious adverse reactions in more than 100 participants in the trials… Chloroquine was selected after several screening rounds of thousands of existing drugs. Chloroquine is undergoing further trials in more than ten hospitals in Beijing, Guangdong province and Hunnan province.”[6]
…
Chloroquine as a prophylactic (preventative) measure against COVID-19[11]
According to research by the US CDC, chloroquine has strong antiviral effects on SARS coronavirus, both prophylactically and therapeutically. SARS coronavirus has significant similarities to COVID-19. Specifically, the CDC research was completed in primate cells using chloroquine’s well known function of elevating endosomal pH. The results show that “We have identified chloroquine as an effective antiviral agent for SARS-CoV in cell culture conditions, as evidenced by its inhibitory effect when the drug was added prior to infection or after the initiation and establishment of infection. The fact that chloroquine exerts an antiviral effect during pre- and post-infection conditions suggest that it is likely to have both prophylactic and therapeutic advantages.”
The study shows that chloroquine is effective in preventing SARS-CoV infection in cell culture if the drug is added to the cells 24 h prior to infection.
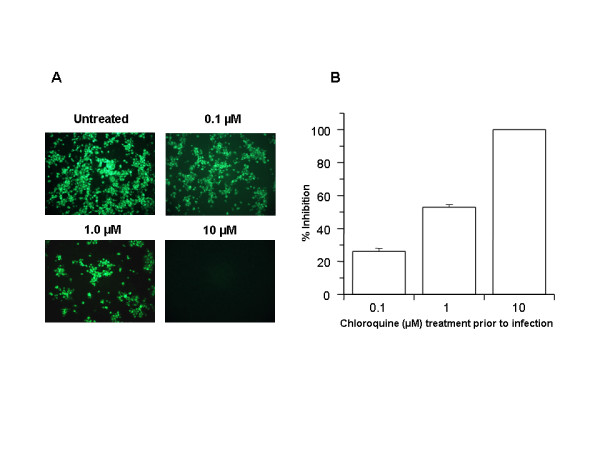
FIGURE 1
Prophylactic effect of chloroquine. Vero E6 cells pre-treated with chloroquine for 20 hrs. Chloroquine-containing media were removed and the cells were washed with phosphate buffered saline before they were infected with SARS-CoV (0.5 multiplicity of infection) for 1 h in the absence of chloroquine. Virus was then removed and the cells were maintained in Opti-MEM (Invitrogen) for 16–18 h in the absence of chloroquine. SARS-CoV antigens were stained with virus-specific HMAF, followed by FITC-conjugated secondary antibodies. (A) The concentration of chloroquine used is indicated on the top of each panel. (B) SARS-CoV antigen-positive cells at three random locations were captured by using a digital camera, the number of antigen-positive cells was determined, and the average inhibition was calculated. Percent inhibition was obtained by considering the untreated control as 0% inhibition. The vertical bars represent the range of SEM.
…
In addition, the study also shows that chloroquine was very effective even when the drug was added 3–5 h after infection, suggesting an antiviral effect even after the establishment of infection.
…
The UK has banned the export of Chloroquine[13]
As of February 26, 2020, the UK government has added chloroquine to the list of medicines that cannot be parallel exported from the UK. Chloroquine was never on this list before. This likely happened because of the growing body of evidence of chloroquine’s effectiveness against coronavirus.
China prioritizes internal use of Active Pharmaceutical Ingredients (APIs) including Chloroquine[14]
In early February, Chongqing Kangle Pharmaceutical was requested by the Ministry of Industry and Information Technology, Consumption Division to promptly increase the manufacturing and production of the active pharmaceutical ingredients chloroquine phosphate despite slowed production during the Chinese New Year.
…
Conclusion
Chloroquine can both both prevent and treat malaria. Chloroquine can prevent and treat coronavirus in primate cells (Figure 1 and Figure 2). According to South Korean and China human treatment guidelines, chloroquine is effective in treating COVID-19. Given chloroquine’s human safety profile and existence, it can be implemented today in the U.S., Europe and the rest of the world. Medical doctors may be reluctant to prescribe chloroquine to treat COVID-19 since it is not FDA approved for this use. The United States of America and other countries should immediately authorize and indemnify medical doctors for prescribing chloroquine to treat COVID-19. We must explore whether chloroquine can safely serve as a preventative measure prior to infection of COVID-19 to stop further spread of this highly contagious virus.
Full study available here
Then there’s this second study:
Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studiesJianjun Gao, Zhenxue Tian, Xu Yang
Abstract
The coronavirus disease 2019 (COVID-19) virus is spreading rapidly, and scientists are endeavoring to discover drugs for its efficacious treatment in China. Chloroquine phosphate, an old drug for treatment of malaria, is shown to have apparent efficacy and acceptable safety against COVID-19 associated pneumonia in multicenter clinical trials conducted in China. The drug is recommended to be included in the next version of the Guidelines for the Prevention, Diagnosis, and Treatment of Pneumonia Caused by COVID-19 issued by the National Health Commission of the People’s Republic of China for treatment of COVID-19 infection in larger populations in the future.
https://www.jstage.jst.go.jp/article/bst/14/1/14_2020.01047/_article
Finally, there’s a new study in the prestigious journal Nature:
Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro
Excerpt:
Chloroquine, a widely-used anti-malarial and autoimmune disease drug, has recently been reported as a potential broad-spectrum antiviral drug.8,9 Chloroquine is known to block virus infection by increasing endosomal pH required for virus/cell fusion, as well as interfering with the glycosylation of cellular receptors of SARS-CoV.10 Our time-of-addition assay demonstrated that chloroquine functioned at both entry, and at post-entry stages of the 2019-nCoV infection in Vero E6 cells (Fig. 1c, d). Besides its antiviral activity, chloroquine has an immune-modulating activity, which may synergistically enhance its antiviral effect in vivo. Chloroquine is widely distributed in the whole body, including lung, after oral administration. The EC90 value of chloroquine against the 2019-nCoV in Vero E6 cells was 6.90 μM, which can be clinically achievable as demonstrated in the plasma of rheumatoid arthritis patients who received 500 mg administration.11 Chloroquine is a cheap and a safe drug that has been used for more than 70 years and, therefore, it is potentially clinically applicable against the 2019-nCoV.
Our findings reveal that remdesivir and chloroquine are highly effective in the control of 2019-nCoV infection in vitro. Since these compounds have been used in human patients with a safety track record and shown to be effective against various ailments, we suggest that they should be assessed in human patients suffering from the novel coronavirus disease.
A commonly available over-the-counter quinine source exists in Margosa Tree Bark and Cinchona succirubra, Peruvian Bark


Tablets of bark extract are widely available in tablet form, from many sources, including Amazon.com here.
There’s also quinine in Tonic Water, which is available just about anywhere at any grocery or liquor store and also at Amazon:
Tonic water is a soft drink containing quinine, which gives it a bitter taste. Quinine is a common treatment for malaria. Quinine comes from the bark of the cinchona tree.
UPDATE:
From Facebook, Dr. Roy Spencer adds this new information.- Anthony
On the subject of using antimalarial drugs for COVID-19 treatment, I’ve compared COVID-19 cases versus malaria incidence by country….
This is amazing. I downloaded all of the data for 234 countries, incidence of total COVID-19 cases (as of 3/17/2020) versus the incidence of malaria in those countries (various sources, kinda messy matching everything up in Excel).
RESULTS, Multi-country average malaria cases per thousand, COVID-19 cases per million, in three classes of countries based on malaria incidence:
- Top 40 Malaria countries: 212 malaria = 0.2 COVID-19;
- Next 40 Malaria countries: 7.3 malaria = 10.1 COVID-19
- Remaining (81-234) countries: 0.00 malaria = 68.7 COVID-19
Again, the units are Malaria cases per thousand “population at risk”, and COVID-19 cases per million total population.
In all my years of data analysis I have never seen such a stark and strong relationship: Countries with malaria basically have no COVID-19 cases (at least not yet).
Additional support for antimalarial drugs for COVID-19 treatment comes from this investigation linked below.
The map says it all: COVID-19 is where Malaria is not.

Absolutely great news Anthony. You’re already my hero but this is huge news. It was mentioned on Breitbart but they took it from top story to the basement for some crazy reason. I’ve read 4 papers and the abstract of a fifth and they all corroborate each other look very very real. This doesn’t appear to be a mild success either, these medicines not only prevent you from getting the disease but some are claiming they are an absolute cure.
1 – Note that this is NOT a confirmed cure – it is a reported possibility. How many other reported possibilities turn out to be incorrect in other situations?
2 – NO ONE in the media is interested in ‘good news’ – especially when there is a panic going on. Think about it. Which would you be more likely to read – an item saying that everything is OK, or one saying that you might die?
The media are NOT in the business of providing a balanced view of a situation. They are in the business of getting readers.
Dodgy, I don’t and never have waited for others to figure things out–especially government. The data in this case is something I’ve looked quite deeply into. This sucker is dead.
Both my wife and I are on a 200 mg/day regimen. Both with health considerations, and we’re not going to simply wait for something that MAY be released sometime in the future if the politicians at the CDC and FDA decide that flyover country is worth it. Certainly the small investment is worth the risk.
If I were closer to the Mexican border, we’d be making a run there for our friends. The usual Canadian pharmacies don’t appear to be stocking the product, at least on line.
Up early, with a breakfast of a Vitamin D pill washed down with Tonic Water (Quinine). Good thing I skipped the Gin, because I’m already grumpy.
Here is my complaint:
I’ve been writing since 2002 about the failure of green energy to provide useful (dispatchable) electrical power, due to intermittency and diffusivity.
Since then, tens of trillions of dollars have been squandered by incompetent/corrupt politicians on green energy scams – that are not green and produce little useful energy.
Excess winter deaths in the United Kingdom total up to 50,000 per year, often triple the per capita rates of Canada and the USA, because of needlessly high energy costs and poor housing insulation, etc.
We are now seeing a huge reaction to the Coronavirus scare, and rightly so – schools closing, sports and cultural events cancelled, restaurants closed, etc.
So how is it that the green energy scam, propelled by the global warming/climate change scam, has been allowed to continue? Is it that 50,000 needless Excess winter Deaths don’t count, but the risk of dying of coronavirus is serious? Maybe it‘s because everyone of a certain age is at risk from the coronavirus, but only the elderly-and-poor die from energy poverty – the inability to heat their homes due to excessively high energy costs caused by wind-and-solar-power scams.
Yes I’m grumpy, but with good reason. Deaths are deaths – it doesn’t matter if you are killed by the coronavirus or by the phony green actions of incompetent and corrupt politicians.
I’m going back to bed and hibernating – turning the electric blanket up to nine – see you in the Spring.
Regards, Allan
https://wattsupwiththat.com/2017/07/17/alarm-about-alarmism/comment-page-1/#comment-2553701
Joe d’Aleo and I had written a paper on Excess Winter Mortality based on other evidence when the major Lancet study was published, so we revised our paper to include that excellent study. Our summary reads:
“Cold weather kills. Throughout history and in modern times, many more people succumb to cold exposure than to hot weather, as evidenced in a wide range of cold and warm climates.
Evidence is provided from a study of 74 million deaths in thirteen cold and warm countries including Thailand and Brazil, and studies of the United Kingdom, Europe, the USA, Australia and Canada.
Contrary to popular belief, Earth is colder-than-optimum for human survival. A warmer world, such as was experienced during the Roman Warm Period and the Medieval Warm Period, is expected to lower winter deaths and a colder world like the Little Ice Age will increase winter mortality, absent adaptive measures.
These conclusions have been known for many decades, based on national mortality statistics.”
Cold Weather Kills 20 Times as Many People as Hot Weather September 4, 2015
by Joseph D’Aleo and Allan MacRae
https://friendsofsciencecalgary.files.wordpress.com/2015/09/cold-weather-kills-macrae-daleo-4sept2015-final.pdf
https://wattsupwiththat.com/2017/09/23/the-evils-of-climate-enthusiasm/#comment-2618246
[excerpts]
The elderly and the poor in the United Kingdom, Germany and other countries are suffering increased winter deaths due to high energy costs. In the UK, this human disaster is called “Heat or Eat”.
The Excess Winter Mortality Rate in Britain is much higher than that in Canada. Canada has a population of about 35 million and the UK about 65 million, but Excess Winter Mortality in Canada is about 5000 to 10,000 per year, and in the UK it is 25,000 to 50,000 per year.
Canada and the UK have genetically similar populations and similar health care systems. Canada tends to be colder but mostly drier than the UK. However, Canada generally has much lower energy costs and better-insulated housing and probably better central heating systems, on average. This suggests that adaptation to winter and low energy costs are significant drivers of lower Winter Mortality rates.
Imagine IF the UK had competent politicians in the past several decades instead of warmist imbeciles. Instead of spending billions on green energy debacles, they could have spent the funds on improving home insulation and central heating, and encouraged fracking of shales to reduce natural gas prices., and a whole lot of grannies and grandpa’s would still be alive for their grandchildren.
Cheap, abundant, reliable energy is the lifeblood of society – it IS that simple.
When politicians fool with energy systems, real people suffer and die.
Regards, Allan
Alan
In contrast to the Italian, French or British the Germany’s mortality rate is very low, perhaps sauerkraut and schnapps for breakfast might do it. 🙂
Hi Vuk,
I read somewhere recently that millions of German households are living without electricity because of unpaid bills. Is this correct? I cannot find the reference.
I believe you are correct, that Excess Winter Deaths in Germany were lower than the UK and many other European countries – at least in the past – the following study includes data from 1988-1997, before the German Energiewende lunacy drove up electricity costs to their current high levels. German EWD’s may be much higher now.
I believe that German housing is better-built that English housing, much of which reportedly has very poor insulation, drafty windows, etc.
And as you say, it could also be the diet – schnapps and fish – high in Vitamin D.
EXCESS WINTER MORTALITY IN EUROPE: A CROSS COUNTRY ANALYSIS IDENTIFYING KEY RISK FACTORS
http://jech.bmj.com/content/57/10/784.full
Table 1 – Coefficient of seasonal variation in mortality (CSVM) in EU-14 (mean, 1988–97)
CSVM 95% CI
Austria 0.14 (0.12 to 0.16)
Belgium 0.13 (0.09 to 0.17)
Denmark 0.12 (0.10 to 0.14)
Finland 0.10 (0.07 to 0.13)
France 0.13 (0.11 to 0.15)
Germany 0.11 (0.09 to 0.13)
Greece 0.18 (0.15 to 0.21)
Ireland 0.21 (0.18 to 0.24)
Italy 0.16 (0.14 to 0.18)
Luxembourg 0.12 (0.08 to 0.16)
Netherlands 0.11 (0.09 to 0.13)
Portugal 0.28 (0.25 to 0.31)
Spain 0.21 (0.19 to 0.23)
UK 0.18 (0.16 to 0.20)
Mean 0.16 (0.14 to 0.18)
Alan,
as per May 2019 – 340.000 were affected by power cuts.
Source
Thank you Krishna,
I thought the numbers were higher.
However, even 340,000 could lead to many Excess Winter Deaths.
Regards, Allan
Most of the West Germany Germans are fine with good incomes, the East Germans’ standard of living has greatly improved too. It is nearly 15 million immigrants ‘gastarbeiters’ although not too badly paid many unnecessarily live below official poverty line in monetary terms. Most ‘gastarbeiters’ send significant proportion of their earnings back to their close or extended families in the countries of the origin.
https://wattsupwiththat.com/2018/01/09/hewlett-packard-report-includes-planned-penal-colonies-for-climate-skeptics/#comment-2254514
I’ve taken time to publish a bit more on this subject
https://noconsensus.wordpress.com/2020/03/19/zero-risk-options-for-treating-coronavirus-patients/
It would seem that antivirals are our best hope for treatment. Isolation and immune system boosting are what can be done now on a wide scale to avoid succumbing to the disease.
Vaccines testing is going to take months and it will take months to produce them. Certainly some amount of production could be done in parallel but one year out is probably overly optimistic for vaccines to play a role on any mass scale.
The researchers going around the system and studying these antivirals are doing the right thing. I hope that all the promising early studies you reference turn out to be correct.
Good summary. Thanks, William.
I would like to see a summary of the issues concerning different vaccines and the methods of producing vaccines.
There is a class of vaccines and a plant based method of producing vaccines which it appears has been suppressed (by endless testing and no funding) as it is too good.
Big Pharma controls what ever they can to maximum profit.
From your summary…
“Even though the CDC knows these drugs are safe to administer, people right now are having extreme breathing difficulties due to the virus and many will die. The CDC is recommending against the near zero risk opportunity to wait until additional testing is complete.”
It is a good thing we have a President, who is only in it for us, not the money which explains why he can deal with the Government Swamp of Special interests.
https://www.foxnews.com/politics/trump-fda-experimental-drugs-coronavirus
Trump announced at a White House press briefing that chloroquine, a drug designed for use in malaria, has been FDA approved and will be made available by prescription “almost immediately.”
Perhaps, but theres also a pretty good correlation between few CV cases and countries with rubbish health services that do retest and report very well. And oddly enough, those countries don’t have a lot of old people and they are busy dying of stuff like malaria, TB, malnutrition and the rest, so CV goes unnoticed.
Good comment.
50 grams of chloroquine phosphate as 200 x 250mg tablets is about 4.40$ in Vietnam.
50 grams of chloroquine phosphate is enough to kill at least a dozen people, probably more.
Hydroxychloroquine has an unusually long elimination half-life of 40–50 days, and I assume that chloroquine phosphate is probably the same. For malarial prophylaxis, an adult typically takes just 500 mg of chloroquine phosphate weekly.
The dose required for efficacy is not far from the lethal dose. In fact, the prescribing information says that as little as 1 gram (1000 mg) can be fatal to a child:
https://www.drugs.com/pro/aralen.html
The dead guy apparently took about 5 grams, all at once, which is a massive overdose. That’s why he’s dead.
The world’s basic problem is overpopulation . The crowding together of people in megalopolies and the demographics of many countries where 40% of the people are under 35 with no work causes mass migration across national borders. The current minor blip in corona deaths, far from reducing the population ,will cause a massive increase 9 months down the line as many millions are required to stay home from work or even shelter in place with little to do to pass the time . We should prepare for the health care systems to be overwhelmed. A world wide crash program in midwife recruitment and training should be started immediately.
This is a very important notion, however, to be aware that the only humane method of overpopulation is family planning. Those who are obstructing it must be hard-pressed.
“Family planning”: Libspeak for the systematic killing of innocents.
It won’t be too long before the most self absorbed generation (Millennials) use “family planning” to justify wheeling members of the 2nd most self absorbed generation (Boomers) to the elimination centers. I fear a day is coming when adult “eliminations” will outnumber baby abortions.
Some years back, Germans feared todie out !
Source
So, some more will not be so bad 😀 (at least for the pension schemes)
Sigh. Malthusians sure are persistent. There are also completely wrong. Also, they refuse to personally help improve the situation they say is so dire. They’re kind of like warmunists who regularly fly to the coasts to enjoy their oceanfront property.
Restated, some people believe if we can just kill off the population, there will be more stuff to go around. That is anti life and a devastating belief.
Instead, more CO2 will cure most of their worries if only they were rational!
**************
Congrats WUWT! This post mentioned on Mark Levin’s radio show evening of 3-18-20.
**************
Huge deal Mr Watts. Thank you.
They re reporting a 100% cure rate on human studies now!
Yes I heard that live, but he didn’t mention the update …. And the side effects mentioned for Cloroquine on drugs.com are frightening to me. I bought a box of 30 150 mg tablets down here in La Paz mexico – over the counter BTW.
When I saw Dr Roy Spenser’s update, that prompted me to check out my local friendly Farmacorama pharmacist…so I bought a box, but will just hold on to it for a while to see what happens down here in the Baja Mexico. The box only cost $15 OSDs.
I’m a little afraid to start taking them without my doctor’s OK. They just closed all the schools in Mexico.
– JPP
Be careful. There’s only a small margin between the therapeutic dose and the toxic dose, for this drug. You bought more than enough to kill yourself with it.
Cloroquine has a very long typical elimination half-life of 40-50 days. For malarial prophylaxis, it is taken weekly.
There is a tiny glimmer of hope (if confirmed) in the UK today’s total infected numbers (below expected) but too early to call end of exponential rise
http://www.vukcevic.co.uk/UK-COVID-19.gif
Please ignore above comment, there was an error in copying data from a website.
The graph has been corrected, it is the verbiage which is wrong.
My apology.
Comments from other threads:
“Copper Kills Coronavirus. Why Aren’t Our Surfaces Covered in It?
Civilizations have recognized copper’s antimicrobial properties for centuries. It’s time to bring the material back.”
Fast Company, Mar 16 · 5 min read
https://medium.com/fast-company/copper-kills-coronavirus-why-arent-our-surfaces-covered-in-it-b05d1219ebbf
COMMENT:
Dan Conine
Might be more prudent to just issue brass wire screen masks. Can’t hurt except maybe people will have green noses for a while. I’d be curious to the residual effects on Covid19 survival in their mucus. Copper does diffuse into a lot of stuff.
Can we still buy brass wire wool easily?
ANOTHER TIP:
Jerry2012I
Comments14 | + Follow
I carry a sprayer in my pocket. I spray the door handle before opening and after. Then I spray my hands . I touch nothing. I was raised by hospital educated people and it can be done. It is not perfect but close to it. I have not been sick with the flu, a cold, or any other viri in 30 years. I practice good hygiene. I even have bidets in the 3 bathrooms in my home. I use bleach to spray the toilets. It can be done.
Richard Epstein downplays Covid-19 effects and countermeasures—podcast
https://reason.com/podcast/richard-epstein-more-probable-than-not-total-number-of-deaths-at-under-50000/?utm_medium=email
We are starting to get widespread confirmation of Chloroquine prophylaxis – see:
https://www.mediterranee-infection.com/wp-content/uploads/2020/03/Hydroxychloroquine_final_DOI_IJAA.pdf
If it is any consolation, there are no reports from either China or Italy of patients who have been put on a respirator recovering. They just die more slowly, so it doesn’t make a huge difference. The virus causes your immune system to destroy your pneumonocytes, if it kills enough then you cannot recover.
In Germany they start clinical tests during next days with Chloroquine, gouvernement secured a greater quantity
The French media Le Figaro is happy to post articles doubting Raoult…
If he had been a vociferating teen with blond pigtails, he would have been received with more deference…
US Wuhan virus task force briefing this morning discussed Chloroquine and indicated it will be tested in an accelerated designed study for effectiveness against the virus. Also, blood plasma taken from healthy individuals that have had the Wuhan virus will be evaluated for preventative and therapeutic effects on those that have not yet had the virus or are currently expressing symptoms.
Study of convalescent plasma treatments for SARS showed a positive effect on outcomes. This was one treatment possibility that was mentioned a month ago in the WHO table linked below, along with other treatments, such as remdesivir. If there is one positive, it’s that studies are at least being initiated quickly.
https://www.who.int/blueprint/priority-diseases/key-action/Table_of_therapeutics_Appendix_17022020.pdf?ua=1
Immunoglobulins are a time tested treatment for a wide range of infectious diseases.
It is a part of every tetanus booster, for example.
Immunoglobulins is a protein component of blood plasma.
It is another word for antibodies.
Trump has just basically confirmed that hydroxychloroquine is the one they are (FDA) looking at to quickly resolve this mess. Watch the news ect next 3-4 days will be tested on 1000’s and my bet confirmed. This whole thing will be gone in 4 weeks as predicted buy back into your stock cheers and LOL. Thanks to Anthony for persisting with this post
He said that chloroquine and remdesivir have both been approved for usage in coronavirus patients.
It is unclear if he was saying remdesivir has been approved by the FDA or if he was referring to opening up the compassionate usage guidelines.
Chloroquine of course was already approved for other purposes, and so the safety profile does not need to be determined.
But it would be a mistake to overlook that the qualitative and quantitative results are still pending.
It would also be a mistake to overlook the value of getting treated early in the infection.
Once someone is in organ failure, chloroquine is contraindicated.
Remdesivir is not.
The worst off patients are being given remdesivir and are being cured.
It is a true antiviral, in that it directly interferes with/prevents viral replication.
See here:
https://www.msn.com/en-us/news/us/trump-calls-anti-malarial-drug-a-game-changer-for-coronavirus-but-the-fda-says-it-needs-study/ar-BB11qpC2?ocid=msedgntp
Nicholas
My impression from watching the president’s ‘presser’ this morning was that the avenue of use was going to be through the “compassionate usage guidelines.”
You remarked, “Chloroquine … was already approved for other purposes, and so the safety profile does not need to be determined.” Yes and no. Consider Reyes Syndrome. It shows up AFTER the medication (in this case, aspirin) has been used to treat the symptoms of a viral infection. The medical community also needs to be sure that a side-effect of using chloroquine isn’t a life-long problem analogous to Reyes Syndrome. It might be necessary to use chloroquine (assuming it is actually effective) until something better comes along. But, just because it has been used with acceptable side-effects for malaria prevention and arthritis doesn’t mean that there might not be problems associated with using it on the corona virus. Again, a need for caution.
Anxious elders rush in where angels fear to tread.
Good points.
All cause mortality is the true measure of what works and what does not.
Of course long term side effects and adverse events are exactly the sorts of things which can only be revealed by following patients over a long period of time in well designed trials.
And also why even when people are dying (which they always have been from every cause), we still have taken years before approving new medications.
The bad things that occur when long term results in a large number of people over extended intervals of time, make it clear that “What have we got to lose” is a very bad standard for treating patients.
And if something does work, we want to numbers, to provide a baseline for improvement…as we will surely not want to stop looking until 100% of people can be saved, and that will likely require combinations of drugs.
Folks are reporting a 100% cure rate for the COVID-19. I’m told that the FDA just released for public use due to administration pressure.
Breadth of concomitant immune responses prior to patient recovery: a case report of non-severe COVID-19
https://www.nature.com/articles/s41591-020-0819-2
No other respiratory pathogens were detected. Her management was intravenous fluid rehydration without supplemental oxygenation. No antibiotics, steroids or antiviral agents were administered. Chest radiography demonstrated bi-basal infiltrates at day 5 that cleared on day 10 (Fig. 1b). She was discharged to home isolation on day 11. Her symptoms resolved completely by day 13, and she remained well at day 20, with progressive increases in plasma SARS-CoV-2-binding IgM and IgG antibodies from day 7 until day 20 (Fig. 1c and Extended Data Fig. 1).
https://www.nature.com/articles/s41591-020-0819-2
Quinine is the main ingredient in number of Quinine salts
from Wikipedia:
Quinine base in various salts
Name Quinine base equivalence
Quinine base 100 mg
Quinine bisulfate 169 mg
Quinine dihydrochloride 122 mg
Quinine gluconate 160 mg
Quinine hydrochloride 111 mg
Quinine sulfate dihydrate [(quinine) 121 mg
These four vitamin supplements are cheap.
Zn, vitamin D, quercetin, and EGCG (from green tea)
Well, also COQ10 is good to have.
These are ionophores to help get Zn inside the cell to disrupt replication of the virus.
Great News !!!!!!
The President is on our side and he has the guts to make things happen.
The President will, if he understands the issue, make things happen.
https://www.foxnews.com/politics/trump-fda-experimental-drugs-coronavirus
Trump announced at a White House press briefing that chloroquine, a drug designed for use in malaria, has been FDA approved and will be made available by prescription “almost immediately.” He said it was one of a number of antiviral therapies to limit the symptoms of the virus that the administration is trying to get to Americans as quickly as possible.
But has it been approved by the CDC ??
JPP
The CDC does not approve drugs and is not involved in the process.
The agency that does is called the FDA.
Chloroquine is approved by the FDA for several conditions.
The parallels between this conversation and those regarding CO2 caused global warming are striking.
I am counting a lot of people who have thrown the logic they have championed regarding climate science right out the window, and are now borrowing the logic of the warmistas.
In case no one noticed, or wondered…that is why Steven Mosher is laughing at this thread.
In WWII when the bombs were falling and people were being blown up, the Federal authorities did not advise that subway tunnels were not approved bomb shelters, so thjey cannot be used.
The FDA, CDC, etc, have been asleep on this for months.
There are a lot of reasons, but he biggest one is the failure to multitask. That showed up in the development of a test kit. Canada had each Province doing its own developments, plus Ottawa, so the odds of success were multiples higher. Then there is the production of masks, etc.,
With regard to using anti viral drugs, they needed to have asked the medical community to treat suspected cases as a malaria case from the get go. Pakistan advised on its use in December I read. Better safe than sorry.
Now we shut down an economy and will cause untold deaths due to depression, and who knows, a rise in violent crime among desperate people.
The FDA was not prepared. Trump was prepared, witness the ban on travel from Wuhan. After that, all the failures were among the “professionals”. Sad.
The economy will be restarted in two weeks, count on it. In WWII they did not stop the war economy because bombs killed people every day. People had to be fed, housed, clothed, and that required people to work, not cower in basements.
Bureaucracy is yet again proving itself to be inept, slow and ineffective at doing anything, and now they want everyone to fall upon our knees and worship them for simply doing, finally, what they should have done months ago.
Nicholas McGinley: First, I am grateful to you, taking time to post here. Your information and call for caution brought some abuse, you handled it well. After all this reading, I still find you too cautious on quinine and such, but will defer to you because your posts prove you know far more than most, including me, on this subject. Please forgive us grasping for a quick solution, but it’s a hell of a situation (I’m sure you agree) with elements of panic (not seen here). In the end, docs and nurses are surely doing their own “testing” regardless of what we think. They will try it because, as opposed to some brand new chemical mix, they will know the history of chloroquine as safe for vast majority.
Second, I like the idea that Mr. Mosher is laughing at us. If we point out that co19 is a real emergency unlike climate emergency, he will point out that he has never said climate emergency, instead he calls for caution and planning. So I asked him to help plan future electric production. Have you any thoughts there? I know you’re busy.
P.S.- I try to learn from Mr. M. but he earns some of the abuse he gets IMO.
Paul,
Thank you for the kind words.
Sorry it took me so long to find your comment here…these discussions overlap and I do not have it set so I get notices when I get a reply.
In any case, I am not against chloroquine, just against assuming anything based on sketchy data.
We need quantified results, not tens of thousands of anecdotal reports.
In any case, it seems we ought to have some results, at least preliminary ones, in the near future, and trust me when I say…I am as hopeful as anyone that this stuff is a miracle.
Having followed biopharma research for many years, I know that clinical trials often give disappointing results, and also they often give mixed and difficult to parse results.
Very rarely does any drug prove highly effective in an infected individual.
At this point many days have gone by, and people are dying in ever higher numbers in the countries that adopted a chloroquine (or is it hydroxychloroquine…I confess I have not done a good job of paying close attention to the distinction) standard of care for all patients deemed to be seriously at risk, except for those in the worst condition, who are being prioritized to remdesivir.
So people are dying in ever greater number…which could mean it is not working, or it could mean it helps people who are not going to die by dialing down cytokine release syndrome (aka cytokine storm), improving the inflammatory response, and thus helping people while not being strictly speaking an antiviral.
I have posted here and there about clinicaltrials.gov site listings of the malaria drugs from the past two decades against several viruses, and none found any benefit, at all.
There were dozens of such studies using both forms of the drug.
And there was a large animal model study using the SARS virus, which tested a large number of drugs, including several quinine derivatives, one of which was chloroquine…and chloroquine was found to specifically not have antiviral activity in vivo, although it did have the well know anti inflammatory and immunomodulating effects it is used for in lupus and RA patients.
Also how a general anti viral property could have ever been overlooked in drugs that have been used by millions all over the world for many decades, is hard to account for.
So there is reason…ample reason…to be skeptical.
In fact we should always be skeptical about such things…but also hopeful.
There are reasons to be hopeful.
But we need to recall why we have known for a long time that only double blind clinical trials are scientific evidence.
People treating patients are very bad at deciding such things…which is why the double in double blind is a requirement.
We need great info, especially when the stakes are so high.
Because…there are other drugs for inflammation and to treat cytokine storm…we would not want people to be getting an inferior treatment.
Ultimately, I suspect none of the drugs being tested is going to show 100% efficacy.
If remdesivir was that good, the studies would have been unmasked by now, I think.
And if chloroquine was that good…I do not think we would still be seeing hundreds per day dead in countries that have been using it for several weeks now.
Yes, for use in an emergency.
BTW, we don’t need to wait the warmer season, especially because we spend most time indoors. Just crank up AC to increase air temperature and humidity.
This poor man’s means to reduce transmission oft respiratory viruses is now shown to work against #COVID19.
https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3551767
But the warmunists would never let say that anything gets better with warmer air
Thank you, Mr. Watts, this article, the contents, information, has been verified by the course of events.
And, most important, the word is getting out, I understand President Trump has stated as such.
From today’s Johns Hopkins Center for Health Security Situation Report:
WHO LAUNCHES MULTINATIONAL TRIAL FOR COVID-19 TREATMENTS The WHO announced that it will soon launch a major trial of prospective COVID-19 treatments . The trial, referred to as the SOLIDARITY trial, will assess possible therapies to treat COVID-19 infections across at least 10 countries. Trial countries include Argentina, Bahrain, Canada, France, Iran, Norway, South Africa, Spain, Switzerland, and Thailand. Four trial arms consisting of drugs or combinations of drugs will be tested against a control arm consisting of standard supportive care. The trial arms will consist of remdesivir; a combination of lopinavir and ritonavir; lopinavir, ritonavir, and interferon-beta; and chloroquine. All 4 options have shown some evidence of effectiveness against SARS-CoV-2 in either in vitro or animal models. After the announcement, research was published that indicates studies in China that assessed lopinavir-ritonavir treatment combinations did not find strong results in the study population.