UPDATE: A Covid-19 case correlation between malarial and non-malarial countries has been plotted by Dr. Roy Spencer, and the results are stunning – see below.
Encouraging news: three new medical studies show a commonly available anti-malaria drug known as chloroquine aka chloroquine phosphate is showing strong results against COVID-19 infections in both China and South Korea. Excerpts from three studies, including one published in Nature are below.

An Effective Treatment for Coronavirus (COVID-19)
Presented by: James M. Todaro, MD and Gregory J. Rigano, Esq.
In consultation with Stanford University School of Medicine, UAB School of Medicine and National Academy of Sciences researchers.
Translation by: Celia Martínez-Aceves (Yale B.S. Candidate 2021), Martín Martínez (MIT B.S. 2017)
Summary
Recent guidelines from South Korea and China report that chloroquine is an effective antiviral therapeutic treatment against Coronavirus Disease 2019. Use of chloroquine (tablets) is showing favorable outcomes in humans infected with Coronavirus including faster time to recovery and shorter hospital stay. US CDC research shows that chloroquine also has strong potential as a prophylactic (preventative) measure against coronavirus in the lab, while we wait for a vaccine to be developed. Chloroquine is an inexpensive, globally available drug that has been in widespread human use since 1945 against malaria, autoimmune and various other conditions.
Chloroquine: C18H26ClN3
Background
The U.S. CDC and World Health Organization have not published treatment measures against Coronavirus disease 2019 (“COVID-19”). Medical centers are starting to have issues with traditional protocols. Treatments, and ideally a preventative measure, are needed. South Korea and China have had significantly more exposure and time to analyze diagnostic, treatment and preventative options. The U.S., Europe and the rest of the world can learn from their experience. According to former FDA commissioner, board member of Pfizer and Illumina, Scott Gotlieb MD, the world can learn the most about COVID-19 by paying closest attention to the response of countries that have had significant exposure to COVID-19 before the U.S. and Europe.[1]
As per the U.S. CDC, “Chloroquine (also known as chloroquine phosphate) is an antimalarial medicine… Chloroquine is available in the United States by prescription only… Chloroquine can be prescribed for either prevention or treatment of malaria. Chloroquine can be prescribed to adults and children of all ages. It can also be safely taken by pregnant women and nursing mothers.”[2]
CDC research also shows that “chloroquine can affect virus infection in many ways, and the antiviral effect depends in part on the extent to which the virus utilizes endosomes for entry. Chloroquine has been widely used to treat human diseases, such as malaria, amoebiosis, HIV, and autoimmune diseases, without significant detrimental side effects.”[3]
The treatment guidelines of both South Korea and China against COVID-19 are generally consistent, outlining chloroquine as an effective treatment.
Specifically, according to the Korea Biomedical Review, in February 2020 in South Korea, the COVID-19 Central Clinical Task Force, composed of physicians and experts treating patients agreed upon treatment principles for patients with COVID-19.[4] In China, the General Office of the National Health Commission, General Office of the State Administration of Traditional Chinese Medicine as well as a Multi-Center Collaborative Group of Guangdong Provincial Department of Science and Technology and Guangdong Provincial Health Comp and the China National Center for Biotechnology Development have established effective treatment measures based on human studies.[5]
According to their research (reported in Clinical Trials Arena),
“Data from the drug’s [chloroquine] studies showed ‘certain curative effect’ with ‘fairly good efficacy’ … patients treated with chloroquine demonstrated a better drop in fever, improvement of lung CT images, and required a shorter time to recover compared to parallel groups. The percentage of patients with negative viral nucleic acid tests was also higher with the anti-malarial drug… Chloroquine has so far shown no obvious serious adverse reactions in more than 100 participants in the trials… Chloroquine was selected after several screening rounds of thousands of existing drugs. Chloroquine is undergoing further trials in more than ten hospitals in Beijing, Guangdong province and Hunnan province.”[6]
…
Chloroquine as a prophylactic (preventative) measure against COVID-19[11]
According to research by the US CDC, chloroquine has strong antiviral effects on SARS coronavirus, both prophylactically and therapeutically. SARS coronavirus has significant similarities to COVID-19. Specifically, the CDC research was completed in primate cells using chloroquine’s well known function of elevating endosomal pH. The results show that “We have identified chloroquine as an effective antiviral agent for SARS-CoV in cell culture conditions, as evidenced by its inhibitory effect when the drug was added prior to infection or after the initiation and establishment of infection. The fact that chloroquine exerts an antiviral effect during pre- and post-infection conditions suggest that it is likely to have both prophylactic and therapeutic advantages.”
The study shows that chloroquine is effective in preventing SARS-CoV infection in cell culture if the drug is added to the cells 24 h prior to infection.
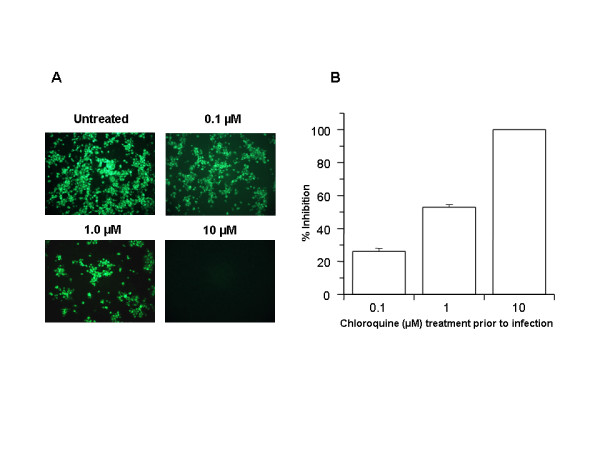
FIGURE 1
Prophylactic effect of chloroquine. Vero E6 cells pre-treated with chloroquine for 20 hrs. Chloroquine-containing media were removed and the cells were washed with phosphate buffered saline before they were infected with SARS-CoV (0.5 multiplicity of infection) for 1 h in the absence of chloroquine. Virus was then removed and the cells were maintained in Opti-MEM (Invitrogen) for 16–18 h in the absence of chloroquine. SARS-CoV antigens were stained with virus-specific HMAF, followed by FITC-conjugated secondary antibodies. (A) The concentration of chloroquine used is indicated on the top of each panel. (B) SARS-CoV antigen-positive cells at three random locations were captured by using a digital camera, the number of antigen-positive cells was determined, and the average inhibition was calculated. Percent inhibition was obtained by considering the untreated control as 0% inhibition. The vertical bars represent the range of SEM.
…
In addition, the study also shows that chloroquine was very effective even when the drug was added 3–5 h after infection, suggesting an antiviral effect even after the establishment of infection.
…
The UK has banned the export of Chloroquine[13]
As of February 26, 2020, the UK government has added chloroquine to the list of medicines that cannot be parallel exported from the UK. Chloroquine was never on this list before. This likely happened because of the growing body of evidence of chloroquine’s effectiveness against coronavirus.
China prioritizes internal use of Active Pharmaceutical Ingredients (APIs) including Chloroquine[14]
In early February, Chongqing Kangle Pharmaceutical was requested by the Ministry of Industry and Information Technology, Consumption Division to promptly increase the manufacturing and production of the active pharmaceutical ingredients chloroquine phosphate despite slowed production during the Chinese New Year.
…
Conclusion
Chloroquine can both both prevent and treat malaria. Chloroquine can prevent and treat coronavirus in primate cells (Figure 1 and Figure 2). According to South Korean and China human treatment guidelines, chloroquine is effective in treating COVID-19. Given chloroquine’s human safety profile and existence, it can be implemented today in the U.S., Europe and the rest of the world. Medical doctors may be reluctant to prescribe chloroquine to treat COVID-19 since it is not FDA approved for this use. The United States of America and other countries should immediately authorize and indemnify medical doctors for prescribing chloroquine to treat COVID-19. We must explore whether chloroquine can safely serve as a preventative measure prior to infection of COVID-19 to stop further spread of this highly contagious virus.
Full study available here
Then there’s this second study:
Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studiesJianjun Gao, Zhenxue Tian, Xu Yang
Abstract
The coronavirus disease 2019 (COVID-19) virus is spreading rapidly, and scientists are endeavoring to discover drugs for its efficacious treatment in China. Chloroquine phosphate, an old drug for treatment of malaria, is shown to have apparent efficacy and acceptable safety against COVID-19 associated pneumonia in multicenter clinical trials conducted in China. The drug is recommended to be included in the next version of the Guidelines for the Prevention, Diagnosis, and Treatment of Pneumonia Caused by COVID-19 issued by the National Health Commission of the People’s Republic of China for treatment of COVID-19 infection in larger populations in the future.
https://www.jstage.jst.go.jp/article/bst/14/1/14_2020.01047/_article
Finally, there’s a new study in the prestigious journal Nature:
Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro
Excerpt:
Chloroquine, a widely-used anti-malarial and autoimmune disease drug, has recently been reported as a potential broad-spectrum antiviral drug.8,9 Chloroquine is known to block virus infection by increasing endosomal pH required for virus/cell fusion, as well as interfering with the glycosylation of cellular receptors of SARS-CoV.10 Our time-of-addition assay demonstrated that chloroquine functioned at both entry, and at post-entry stages of the 2019-nCoV infection in Vero E6 cells (Fig. 1c, d). Besides its antiviral activity, chloroquine has an immune-modulating activity, which may synergistically enhance its antiviral effect in vivo. Chloroquine is widely distributed in the whole body, including lung, after oral administration. The EC90 value of chloroquine against the 2019-nCoV in Vero E6 cells was 6.90 μM, which can be clinically achievable as demonstrated in the plasma of rheumatoid arthritis patients who received 500 mg administration.11 Chloroquine is a cheap and a safe drug that has been used for more than 70 years and, therefore, it is potentially clinically applicable against the 2019-nCoV.
Our findings reveal that remdesivir and chloroquine are highly effective in the control of 2019-nCoV infection in vitro. Since these compounds have been used in human patients with a safety track record and shown to be effective against various ailments, we suggest that they should be assessed in human patients suffering from the novel coronavirus disease.
A commonly available over-the-counter quinine source exists in Margosa Tree Bark and Cinchona succirubra, Peruvian Bark


Tablets of bark extract are widely available in tablet form, from many sources, including Amazon.com here.
There’s also quinine in Tonic Water, which is available just about anywhere at any grocery or liquor store and also at Amazon:
Tonic water is a soft drink containing quinine, which gives it a bitter taste. Quinine is a common treatment for malaria. Quinine comes from the bark of the cinchona tree.
UPDATE:
From Facebook, Dr. Roy Spencer adds this new information.- Anthony
On the subject of using antimalarial drugs for COVID-19 treatment, I’ve compared COVID-19 cases versus malaria incidence by country….
This is amazing. I downloaded all of the data for 234 countries, incidence of total COVID-19 cases (as of 3/17/2020) versus the incidence of malaria in those countries (various sources, kinda messy matching everything up in Excel).
RESULTS, Multi-country average malaria cases per thousand, COVID-19 cases per million, in three classes of countries based on malaria incidence:
- Top 40 Malaria countries: 212 malaria = 0.2 COVID-19;
- Next 40 Malaria countries: 7.3 malaria = 10.1 COVID-19
- Remaining (81-234) countries: 0.00 malaria = 68.7 COVID-19
Again, the units are Malaria cases per thousand “population at risk”, and COVID-19 cases per million total population.
In all my years of data analysis I have never seen such a stark and strong relationship: Countries with malaria basically have no COVID-19 cases (at least not yet).
Additional support for antimalarial drugs for COVID-19 treatment comes from this investigation linked below.
The map says it all: COVID-19 is where Malaria is not.

The company who makes chloroquine:
https://eenvandaag.avrotros.nl/amp/item/medicijn-uit-zeewolde-nu-onderdeel-van-voorlopig-behandeladvies-coronavirus/?__twitter_impression=true
Popma previously said the drug is quick and relatively inexpensive to make . “I can provide 17 million people with this drug, as well as the rest of Europe,” he said
Over the last month or so, when there is mentioned that China produces the raw ingredients to a large number of medicines used in the USA, also mentioned there is a shortage of one of the medicines but the name of the drug is not mentioned.
I wonder: is that drug in short supply named Chloroquine?
Does anyone know?
RiHoO8
I read a comment on twitter, that pakistan had sent chloroquine to china, in large numbers…
not sure but they also ramped up VitC production as they were using that as well
Id also suspect that the ASF outbreak killing so many pigs has made Heparin supplies harder to come by
its made from pig intestines. in china pretty much sole supplier no matter whos brand names on it.
like many of the overpriced drugs you think are made in usa and are not.
Does anyone know if ARB’s, such as Losatan, are being succesfully used. I would imagine ARB’s would block the entry path.
There is concern that ARBs and Ace inhibitors can make a person MORE susceptible by increasing the cells receptors.Apparently Advil may also do this.
https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(20)30116-8/fulltext
Meanwhile the CBC keeps the garbage rolling… with Bill McKibben…
https://www.cbc.ca/radio/thecurrent/the-current-for-march-12-2020-1.5494992/covid-19-pandemic-response-temporarily-combating-co2-emissions-but-systemic-change-needed-experts-urge-1.5495303
Is “icisil” a resurrection of “Nicholas McGinley “?
No
What comment disturbed you, btw?
The French have seen similar results with chloroquine.
https://www.connexionfrance.com/French-news/French-researcher-in-Marseille-posts-successful-Covid-19-coronavirus-drug-trial-results
The French have found similar results with chloroquine
https://www.connexionfrance.com/French-news/French-researcher-in-Marseille-posts-successful-Covid-19-coronavirus-drug-trial-results
I’m not sure why everyone is saying garlic is not effective, without pointing to any actual evidence.
How would you interpret this?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4967842/
as positive and worth using, and I do;-)
and yes its being added to caged bird and other stock feeds to lower the abuse of antibiotics in feeds already
Trust your gut feelings. Mine, based around lots of research, are saying:
– Over the next 2 years most of us will be exposed to this infection (the past is a window into the future)
– There will be no preventative vaccine developed within this time frame
– The economic fallout will be much more severe (for society) than the condition
I contacted my bank this morning informing them that they will be first to have a default payment from my accounts. Utilities will be next. Cut off my electricity if you dare
I am self employed. If the building industry contracts I contract. I will feed my family whatever it takes. Leave the cave to find the food. Sorry sisters, you still need us
Governments around the world are trying to slow down the infection rate so that the health sector and financial institutions have more time to cope. Every aid package instigated by our NZ Government requires applications processing. None of the above mentioned institutions have the capacity to handle the surge which is coming
While I am of the high-risk age group I believe that time will show that they would have best let the pandemic run at its own pace while allow society to carry on as normal. Every action has an up and downside. Like war: collateral damage. It is unavoidable
Cheers
M
I tend to agree. I think when they cancelled the NBA over one guy getting it, that started all of this insanity.
But that may be a miscalcuation itself.
This is not just killing one percent of people over 80.
It is giving a lot of young people a very serious case of viral pneumonia, which is very often fatal without modern medical care. So when the beds run out, is when the death rate is spiking.
I saw some very clear graphics on that regarding Italy on CNBC today.
ICU beds run out, more people die.
And lots of young people get it, just not as a proportion of total illnesses. But if the total is 50% of the whole country or world, depending where you live, and it happens very quickly, that is a lot of people with pneumonia in a short time…too short to allow beds to clear.
Our system is not set up to care for hundreds of thousands of people needing around the clock support and care in a hospital.
Thanks for the article.
Garlic extract appears to inhibit Avian infectious bronchitis virus (IBV) in chicken embryos according to the article. That doesn’t mean that it would work for any other virus or if it would work in humans, though humans aren’t susceptible to infection by this IBV.
It might be a good idea to feed your chickens garlic. I suppose you could also eat garlic chicken and it would do no harm.
I am having a fun time reading the old posts here about the virus
and the comments.
Most instructive
It doesn’t really matter since most of us died over 40 years ago when we ran out of oil.
origin of the virus
https://www.nature.com/articles/s41591-020-0820-9
Nice article, dated today and interestingly their global deaths are off, they write with 4,373 deaths, and their footnote is from the 10th so they get a pass. Now, it’s about at 8,000 deaths, (as of this writing 7,933 per John Hopkins… Fantastic website link here with perhaps the best up to date numbers from the world. https://coronavirus.jhu.edu/map.html
Yummy. “In recent years, a number of new diseases that have caused severe illnesses in people have been traced back to bats. Bats are the suspected source of severe acute respiratory syndrome (SARS) virus, Ebola, Marburg virus, Hendra virus, and most recently Middle East Respiratory Syndrome (MERS) virus, to name a few.
In fact, bats are reservoirs for more than 60 viruses that can infect people, according to a 2013 study. The animals host more viruses per species than rodents.”
https://www.livescience.com/44870-bats-viruses-flight.html
And then, I found this: “In the New York Post, Steven Mosher, a regular critic of China’s population control measures, has stoked the leakage rumor, using an array of circumstantial clues that Chinese labs’ handling of deadly pathogens can’t be trusted.”
Is that you?
Steve Mosher is a Global Treasure, regardless of whether we sometimes disagree. His status has been elevated. Be careful when visiting China you don’t get disappeared. However, Steven Mosher is a different guy: https://www.google.com/search?q=steven+mosher+on+china&sxsrf=ALeKk01MwFrQmkta325j7m-0OP329xNxIQ:1584564872881&tbm=isch&source=iu&ictx=1&fir=TSbvAAZKi3cuGM%253A%252Cha_gm8-WbV3G_M%252C%252Fm%252F079d2l&vet=1&usg=AI4_-kQybFG2LXqAjfte63X9tQr5Nt3sqw&sa=X&ved=2ahUKEwiMh_yS9KToAhU6HjQIHSDbBs8Q_B0wEnoECAkQAw
Different Steven Mosher.
He acts the same way wonder if he has an arts degree as well.
so weird.
a few weeks back when infections in the us were at 68 and deaths were at zero
this dummy with an arts degree knew more than you.
hey, who knew you could get an education from life
Maybe.
The data is encouraging but not conclusive. Both chloroquine and remdesivir real trials are starting.
The epidemiological data is worse, and justifies the President’s next 15 day admonitions—even tho AW nixed my CtM update request.
Using the WE skewed DP sample, adjusting only the fatality/recovered denominator, the ‘worst case’ (explained in the nixed update post) CFR is 5.4%, up because of Italy from 5.0 yesterday. Just is.
in case anyone is curious, Hyland’s has a Leg Cramps product sold in most CVS and many super markets, contains Cinchona
Hydrochloroquine has been proven effective against CoV-19 as well as SARS in numerous trials. There is no doubt it works. Side-effects are rare and much less severe than death from viral pneumonia.
It’s a cure. You don’t need a vaccine if you have a cure. Even if many get infected, few will exhibit extreme symptoms, and those who do can be cured.
The panic should be over, finished, done with. This alleged pandemic is not worth rewriting the laws or blowing up the economy. There is a cure. Nobody has to die from this virus.
I know that a certain segment of society loves to panic, either for kicks or for evil control motives. People are prone to panic, especially the modern spoiled leisure-sated liberal sheeple and their lupine masters. Witness the idiotic CAGW panic that has persisted for 20 years.
But the corona virus panic should subside immediately. There is a cure! Get back to work! Put the Congress on permanent recess!
Where did you get this “many studies” nonsense.
From the article, it’s not a cure, it lessens the severity of the symptoms.
The “cure” for this virus, like every other virus, is your own immune response. The tricky part is not dying while your immune response cures you.
So if there is a pill that effectively stops most people from dying, the hysteria really should be over.
Sure, if you have untreated AIDS or you are the bubble boy, this isn’t going to “cure” you. Most people have an intact immune response.
Mike,
The results in humans are suggestive, not definitive, and nothing is proven.
Get real, stop misinforming people, Mike.
You blanket statement of unqualified success is not warranted.
IOW…you just made that up…so stop it!
COVID19 Treatment by HydroChloroquine & azithromycin
An Effective Treatment for Coronavirus (COVID-19)
Presented by: James M. Todaro, MD (Columbia MD, jtodaro2@gmail.com) and Gregory J. Rigano, Esq. (grigano1@jhu.edu)
https://twitter.com/RiganoESQ/status/1239780304082124800
Gautreta et al. (2020) Hydroxychloroquine and azithromycin as a treatment of COVID‐19: results of an open‐label non‐randomized clinical trial. International Journal of Antimicrobial Agents – In Press 17 March 2020 – DOI : 10.1016/j.ijantimicag.2020.105949
An Open Data Clinical Trial for COVID-19 Prevention
INTERVIEW – GREGORY RIGANO – co-author on study of Chloroquine, Advisor to the Stanford University School of Medicine
I miss Climate Change.
“Some say the world will end in fire; some say in ice…”
etc, etc.
Herbert
Not to worry! It will come back.
Climate change is so yesterday, we cancelled it due to lack of interest. Now it’s all about the toilet roll 🙂
We did not know we were living in paradise and had the time and money to spend on silly stuff that we called has called green in that time.
This is a paradigm change.
In a time of war there can only be one number one priority and that will be 20% unemployment.
Giving money to people does not bring back their jobs.
Let’s hope the vaccine comes soon. I would like to know more about the vaccine options.
So why no broader statements from “authority” saying that it is all but over. Not even peep from the MSM. Only wash your hands and stay inside.
Because it isn’t. Having a new treatment just means that hopefully, fewer people will die.
I am as hopeful as I could be that this is exactly as some seem to think, and a cheap and tested and easy to get drug will keep people from being infected and keep anyone from dying who does.
But I aint bettin’ the farm on it.
This is how alt medicine journals read, not serious studies from professionals.
They did not give one word about NEWS scores, or any of the language that is used in serious studies.
Here is the kind of language that is typically used:
“Primary Outcome Measures :
Time to Clinical Improvement (TTCI) [Censored at Day 28] [ Time Frame: up to 28 days ]
TTCI is defined as the time (in days) from initiation of study treatment (active or placebo) until a decline of two categories from status at randomisation on a six-category ordinal scale of clinical status which ranges from 1 (discharged) to 6 (death).
Six-category ordinal scale:
6. Death; 5. ICU, requiring ECMO and/or IMV; 4. ICU/hospitalization, requiring NIV/ HFNC therapy; 3. Hospitalization, requiring supplemental oxygen (but not NIV/ HFNC); 2. Hospitalization, not requiring supplemental oxygen;
1. Hospital discharge or meet discharge criteria (discharge criteria are defined as clinical recovery, i.e. fever, respiratory rate, oxygen saturation return to normal, and cough relief).
Abbreviation: IMV, invasive mechanical ventilation; NIV, non-invasive mechanical ventilation; HFNC, High-flow nasal cannula.”
“Secondary Outcome Measures :
Clinical status [ Time Frame: days 7, 14, 21, and 28 ]
Clinical status, assessed by the ordinal scale at fixed time points (days 7, 14, 21, and 28).
Time to Hospital Discharge OR NEWS2 (National Early Warning Score 2) of ≤ 2 maintained for 24 hours. [ Time Frame: up to 28 days ]
Time to Hospital Discharge OR NEWS2 (National Early Warning Score 2) of ≤ 2 maintained for 24 hours.
All cause mortality [ Time Frame: up to 28 days ]
Duration (days) of mechanical ventilation [ Time Frame: up to 28 days ]
Duration (days) of extracorporeal membrane oxygenation [ Time Frame: up to 28 days ]
Duration (days) of supplemental oxygenation [ Time Frame: up to 28 days ]
Length of hospital stay (days) [ Time Frame: up to 28 days ]
Time to 2019-nCoV RT-PCR negativity in upper and lower respiratory tract specimens [ Time Frame: up to 28 days ]
Change (reduction) in 2019-nCoV viral load in upper and lower respiratory tract specimens as assessed by area under viral load curve. [ Time Frame: up to 28 days ]
Frequency of serious adverse drug events [ Time Frame: up to 28 days ]”
It does not even sound like they ttried various dosages to see how much or how little was optimum…the first thing one has to do.
Maybe twice as much is better. Maybe half as much is better.
Maybe people getting identical care and placebo also did “better” than people not getting the drug.
There were words that rang bells for me…words like “curative”.
“An effective treatment”…dont listen to the dangerous lying shills of the oligarchy.
You are what you accuse others of being, Loydo.
Why else would these overpaid spruikers be telling such egregious, scripted lies, then a week later appear genuinely concerned? Because of these lies there are still millions who think Covid 19 is fake news, no worse than the flu, many of them will die.
Loydo you are a poor human being. Shame on you.
Loydo has no concept of shame, don’t waste your keystrokes.
Probably just gave him a self-righteous warm-fuzzy.
Loydo.. its a question of changing data. The spike in Italy changed the global view of the virus by showing how a spike would overwhelm health care facilities, and people were triaged to die alone.
It is possible to be wrong, based on weak data and personal values, then change ones mind with more data.
Too bad climate change alarmists can’t do that.
Loydo is a socialist who will do and say anything that she thinks will get her closer to more free stuff.
Whenever someone says something a liberal disagrees with, it instantly becomes a lie, and the person involved becomes part of a huge conspiracy.
They were presenting the data that was known at the time. That’s not lying, even if your bosses are now telling you to say so.
Isn’t it amazing how Loydo has jumped from lying about climate change to lying about the Wuhan Virus. It’s almost as if his pay masters sent out a memo telling him to change topics.
Loydo, can you explain THIS bald faced lie by Mr. Biden?
From The Federalist
Joe Biden Lies About Coronavirus Testing To Make Trump Look Bad
“….At Sunday night’s debate, Democratic presidential contender Joe Biden blatantly lied to the American public about the Trump administration’s handling of coronavirus testing in a pathetic attempt to push the false narrative that a lack of testing has endangered Americans.
“The World Health Organization offered the testing kits that they had available and to give it to us now,” Biden proclaimed.” “We refused it. We didn’t want to buy them,” the Democratic front-runner claimed.
Biden’s claim was false on many fronts and had previously been debunked on at least two occasions. First, during a March 7, 2020 press briefing, Secretary of Health and Human Services Alex Azar and Food and Drug Administration (FDA) Commissioner Stephen Hahn made clear that there were no World Health Organization (WHO) “testing kits.”
Hahn told reporters: “We’ve seen reports about a WHO test, and that WHO is distributing a diagnostic test to countries. And I want to be really clear about this: We’ve been in constant contact with WHO. The WHO does not have its own test that it is distributing globally. It has only posted on its website protocols from some test developers, including our own CDC.”
https://thefederalist.com/2020/03/17/joe-biden-lies-about-coronavirus-testing-to-make-trump-look-bad/
===================
There are plenty more politically motivated lies by democrats to post, but this one is a wide open lie exposure.
Really, your partisanship behavior is making you ignorant and stupid, here is a Forum Thread I started a couple days ago, exposing numerous democrat lies, backed by sourced evidence.
The democrats replies in the thread never responds to the list of ten from the article, they make deflecting replies instead, indicating they have NO counterpoint to offer.
PJ Media
10 Ways the Left Has Politicized the Coronavirus Pandemic
By Matt Margolis March 16, 2020
EXCERPT:
It was disgusting to see the way Joe Biden and Bernie Sanders politicized the coronavirus pandemic during their debate Sunday night. I expected as much, to be honest.
A public health crisis is no time for partisanship. Sadly, for the left, they saw the coronavirus pandemic was just another opportunity for them to take down Trump. From the Russian collusion hoax to the bogus impeachment, they’ve tried relentlessly to find something to not just damage him, but to end his presidency.
The left’s politicization of the coronavirus pandemic has taken many forms, and I’ve compiled the most significant examples below.
10. Wishing infection on Trump supporters
In a now-deleted tweet, liberal activist Susan Daniel declared, “For the record, if I do get the coronavirus I’m attending every MAGA rally I can.”
As bad as that was, Denver City Councilwoman Candi CdeBaca apparently thought it was appropriate to retweet the disgusting comment on her official Twitter account:
(Snip)
9. Prioritizing political correctness over the public health
Is political correctness in the middle of a pandemic helpful? It’s not. Getting offended by language is a distraction from the real problem, but that hasn’t stopped Democrats from doing just that.
There is no doubt that the coronavirus originated in Wuhan, China. Yet, at some point during the outbreak, the Democrats and the media decided that to refer to the virus as the “Wuhan virus” or the “Chinese virus” was racist–at least when Republicans said it. Democrats were triggered when congressman Dr. Paul Gosar announced he would self-quarantine and referred to the virus as the “Wuhan virus.” House Republican leader Kevin McCarthy was similarly accused of racism when he referred to it as the “Chinese coronavirus,” prompting Democrats to call for an apology.
https://pjmedia.com/trending/10-ways-the-left-has-politicized-the-coronavirus-pandemic/
===============
You need to drop your partisan behavior, go with the evidence instead.
Sunsetty
China no more asked for this virus than we did. Their people are dyeing just like ours. Why use a name that offends a whole nation at a time when we need to pull together to fight this virus. It has two official names. Corona and Covid-19. My suggestion is that in the interest of us all working together we use only those two names and leave the blame game out of this.
Simon: Most respectfully, We name diseases from where they originated so that we can understand the history and learn from what went wrong. Lyme disease for instance originated from Lyme Connecticut. China literally hid this disease from the world. Tracking how it spread, and where it went is literally as important as dealing with its consequences.
You are making this into a worse issue with a strawman stance. That is, trying to obfuscate where it came from for reasons that are not helpful.
Chinese propaganda is that our military brought it, and China wants us to not associate it with originating there. So let’s stop the Left wing propaganda and move forward with as little ignorance as possible.
Deal?
I would be all for “pulling together” with China except they keep lying, add to that they shipped people FROM Wuhan to Italy and other countries AFTER they knew full well there was a massive problem coming OUT OF WUHAN. Put that all together and I will continue to call it China Virus, government of China don’t like it they can suck my a$$. They knew as far back as November there was a major problem and HID it from the world AND their own people.
‘So let’s stop the Left wing propaganda and move forward with as little ignorance as possible.’
Simon doesn’t have that button – he’s pretty much left-wing propaganda all day, every day.
Mario
“Simon: Most respectfully, We name diseases from where they originated so that we can understand the history and learn from what went wrong.”
Really? Where did Spanish flu come from?
If we are going to get in to petty name calling maybe it should be called the Trump virus. He’s done more than anyone to make sure it is spread far and wide across the US by:
– Delayed testing
– denying/minimised the dangers
– cutting funding
– misinformed/lying to the public
Simon: you lost me at “Trump virus”. I gave you a shot, and you will no longer benefit from my help.
‘If we are going to get in to petty name calling maybe it should be called the Trump virus. ‘
Uh – yeah, that’s where the progressive left STARTED with this – and you turn around and call us petty.
You’re petty and dishonest. What we’ve done – as always – is respond to you pettiness and dishonesty.
Now go monitor your virus alerts – don’t walk in front of a bus while you’re doing it.
And another thing, you friggin’ clone – I love the way you phrase ‘Trump virus’ as if you came up with it on the spot.
That’s called ‘fronting’.
Funny that Loydo has missed the over-paid shills who pretty much have been parroting the same lies – verbatim – for years – oh like CNN, WAPO, NYT, etc.
They opened up their coverage on this virus as a dishonest, opportunistic attack campaign against Trump – the same spin on every news item for three straight years.
‘Scripted’. Wow. Hypocrisy just doesn’t say it.
Loydo – you’re an embarrassment to humanity.
The sheer lying bigoted smarm constantly being shoveled out by you and your personal gods is what fascism is made of.
a few weeks back when USA cases were at 68 folks like me took a ton of abuse for explaining this low number was the effect of doing no testing.
well a couple weeks have gone by
https://www.worldometers.info/coronavirus/country/us/
Say hello to what you see if you test.
in reality you probably have 60000 to 100000 cases in the US
Here’s another hint
Willis did a nice piece on Gompertz ( my favorite for looking at survival of Ice.)
Korea was a nice fit.
was.
outbreaks poppin up !( 2 areas in SK have yet to peak)
lets just say there were 3 more cases within 5 minutes of me this morning– I get text alerts that are tied to my location and the ‘distance’ window I set. make that 4, it just went off again.
Zombie Apocalypse… they’re coming for you Mosh.
https://youtu.be/4V90AmXnguw
@Steve Mosher… me too. Numbers will skyrocket with testing and that makes it hard to know what part is just measurements adding up vs the actual organic growth rate (or leveling or decline) of the cases. I am glad to hear you chime in here. I tried to ask what you thought of the numbers from China. Are their number of cases fairly accurate? If yes, did they really level off with their isolation measures etc?
“I tried to ask what you thought of the numbers from China. Are their number of cases fairly accurate? If yes, did they really level off with their isolation measures etc?”
I think all we can do is judge the numbers by using consistency tests.
there were some early issues with changing diagnostic criteria.
There are also some issues with “missed cases”
Ex Hubei province shows you what you can do with isolation. They flattened the curve enormously.
So, Hubei numbers: under counted cases, over estimated death rate
Ex Hubei: Shows what you can limit this thing to and death rate for a PREPARED
health system.
isolation measures are less severe now. Today Beijing had a record number of cases
11
All IMPORTS
Now ask yourself this. with only a few flights landing at PEK whats the probability
that 11 people will get off the plane with Covid?
rather shocking
Anyway ALL passengers landing in Biejing will do 2 weeks in Quarentine at their own
expense.
Steve Mosher: Thank you. It’s great having one of our own close to the action… like a war time reporter. I had a feeling that the inflated mortality rate was the driver behind this extreme response. Looks like US is coming down to around 1.6%… down from close to 4% a week or two ago. If it settles around 1%, that’s within the relm of Flu mortality rate of 0.1%. My problem is that I do not know how they are both calculated.
In Flu cases, do they “guess” the number of total cases to be about 0.1% of the death toll?
or do they count and use statistical fudging to guess the total Flu cases?
If it comes out that Covid 19 is indeed 10x worse or more than Flu, then perhaps this was all justified. If it’s on par, we should all know that and the world will get back to work.
As long as there are beds in the ICU, the CFR will stay to the low end.
ICU beds run out, CFR goes way up.
I also spoke about the way S. Korea tested.
It was a world of difference.
We have not seen the last chapter of this book, and we may have only seen the Foreword.
I sincerely hope not. It is possible one or more of these treatments will be effective enough to make a difference.
But they are treatments, not vaccines. We will not have a vaccine soon enough, unfortunately.
This malaria drug, if it will really prevent anyone from every getting infected, and if it is really so safe it can just be passed out like bottles of aspirin (which is also very toxic, as is acetaminophen) then it will become a question of “How fast can they make it, and who will get it until there is plenty for everyone, and is that soon enough to matter”.
A lot of ifs and maybes.
This disease does a slow burn under the radar for, it appears, as much as a month or more, and then it starts showing up as patients with pneumonia at the emergency room.
I would not be so sure any country has this licked and that is that.
Two to four doublings make a huge difference and that is the uncertainty that we are dealing with. Here’s good commentary from a professor of medicine, of epidemiology and population health, of biomedical data science, and of statistics at Stanford University.
https://www.statnews.com/2020/03/17/a-fiasco-in-the-making-as-the-coronavirus-pandemic-takes-hold-we-are-making-decisions-without-reliable-data/
Scissor: This article captures what I have felt for a long time now. It’s a worthy read! People think I am nuts because I typically am skeptical of running with the herd. Thank you!
St. steve complains about things that never happened. Again.
Nobody abused you because you were calling for more testing.
Correct the only thing he got abused for was making stupid statements like Vitamin D was somehow going to improve your chances of survival. Then he started with other stupid statements like his arts degree somehow made him an expert. At the moment he sounds more like an unhinged doomsday prepper than anything else.
“St. steve complains about things that never happened. Again.
Nobody abused you because you were calling for more testing.”
really? and this is just a sample.
https://wattsupwiththat.com/2020/03/07/coronavirus-israeli-health-ministry-wants-to-add-the-usa-to-its-quarantine-list/#comment-2934025
https://wattsupwiththat.com/2020/03/07/coronavirus-israeli-health-ministry-wants-to-add-the-usa-to-its-quarantine-list/#comment-2933134
https://wattsupwiththat.com/2020/03/07/coronavirus-israeli-health-ministry-wants-to-add-the-usa-to-its-quarantine-list/#comment-2933347
https://wattsupwiththat.com/2020/03/07/coronavirus-israeli-health-ministry-wants-to-add-the-usa-to-its-quarantine-list/#comment-2933222
Steven,
My guess is that the cases in the US, if it were somehow possible to find out how many people have been exposed and either never got sick, had mild illness and recovered, or got very sick but thought they had the flu…etc…that total cases in well over a million.
The state of New York is estimating several tens of thousands in that state alone.
I am figuring it very simply: People all over the entire country who have no known contact with anyone who is infected are turning up with the disease.
All socioeconomic strata, all sorts of occupations, just a broad cross section, and spread all the way out.
So there are chains of transmission occurring…as of weeks ago…in every part of the US, and it is a big place.
I am hoping the number is very large. The larger it is, the more obvious it is that most people have nothing to worry about, and also the more reason to think closing down the country is causing more harm than the virus.
If tens to many hundreds of thousands have been exposed, and the numbers in serious trouble or dying is what it is, then the ratio of infection to dire outcome is low.
And if that many have it, it is obvious it spreads so easily it will probably take total lock down to stamp it out.
But I see no way to test enough people to find out or even estimate, unless it is done in a systematic way and not based on self reporting, but more like the way a poll is done.
Question for you: Do a lot of people in China, Japan, and South Korea, have face masks in a drawer somewhere, all the time?
The first thing they did in China, or one of them, was make everyone wear a mask when outside. And at work too it seems.
That is a lot of masks.
How often are they changed?
Are they dirt cheap?
How do they have enough for everyone without running out?
Here of course, one of the first things they did was scold anyone who bought masks and said do not buy them and you do not need to wear them so don’t.
I cannot help thinking that maybe was a really bad idea.
And also that the US has less masks than some cities in Asia.
If there were 60,000 to 100,000 cases in the U.S. on the 17th, then the virus is more easily transmitted and less virulent, in terms of deaths. It would actually be good news in terms of getting this thing over with sooner and with fewer primary deaths (it’s still important to avoid overburdening the healthcare system). Your guess is unfortunately not likely correct.
Certainly, testing now can confirm whether a patient has the virus or not, and testing was limited initially, but death (the severest of outcome) is obvious. CDC compiles all kinds of relevant statistics that can be used to assign excess deaths.
Independently, a plot of reported cases using current methodology vs deaths is linear over the past week and a half for the U.S. and increases are consistent with observations from other countries.
‘I get text alerts that are tied to my location and the ‘distance’ window I set. make that 4, it just went off again.’
I guess that sort of abject cowardice is to be expected from an alarmist.
I wonder what it’s like to go around that afraid all the time?
BTW – I wonder how all that high-density, mass-transit, collectivist philosophy is working out?
That’s nice because the high speed trains of the future will consist of individual pods. This may result in trains being so long that some will get there before they left.
“‘I get text alerts that are tied to my location and the ‘distance’ window I set. make that 4, it just went off again.’
I guess that sort of abject cowardice is to be expected from an alarmist.
I wonder what it’s like to go around that afraid all the time?
BTW – I wonder how all that high-density, mass-transit, collectivist philosophy is working out?”
##################
HUH? Afraid?
Lets see.
The other day I was planning on going to Mapo to get my hair cut.
Alarm went off I saw the location, in Mapo, and decided to go to inchon instead.
AFRAID? hell no, INFORMED, hell yes.
or last week. My friend was going to go into our local hospital. Nothing serious.
Alarm went off. Ah shit some traveller had presented in ER with COVID.
No worries, just go to another hospital.
AFRAID? hell no, INFORMED, hell yes.
So weeks ago I told you all not to panic, but to plan.
USA wasnt even at 50 cases.
You all laughed. and called me alarmist.
As I explained, don’t panic, prepare!
But Ya’ll pointed to a a small number of cases, called it a hoax, blah blah blah.
Say hello to Mr exponential
AFRAID? hell no, INFORMED, hell yes.
How many of you sold short? Waaa. I am guessing none.
AFRAID? hell no, INFORMED, hell yes.
“BTW – I wonder how all that high-density, mass-transit, collectivist philosophy is working out?”
Dunno,
have a look
https://www.worldometers.info/coronavirus/country/south-korea/
But you see dumbass, They planned. They ran “war games” about this thing back in Decemember.
Imagine that!
But then they live a few miles from a Nutjob with Missiles in North Korea
AFRAID? hell no, INFORMED, hell yes.
“”BTW – I wonder how all that high-density, mass-transit, collectivist philosophy is working out?”
Dunno, have a look
https://www.worldometers.info/coronavirus/country/us/
Oh shit.
I sold short Steven.
Sort of. I had/have puts.
More leverage.
Also I suggested a look at call options for Gilead.
That was well over a month ago.
Look at the value of those options now.
I never said anything like what you are pointing out, but I know many did.
But some others were calling it a bioweapon.
I have been making extensive comments on every thread on this subject starting with Rud Istvan’s first one. I do not recall if I commented earleir than that here, but I have posted some stuff I wrote elsewhere long before anyone here was talking about it.
I was one of a very few people who knew that what we are seeing now was a very real possibility.
I also called for a very serious situation with the economy and was laughed at.
I said a few weeks ago, maybe a little less, that when a drug that treats it is found to be successful, we will see the largest stock market rally in history.
We have seen that as well, and we will see more of it, but the selling is not over yet either.
Today is triple witching…expirations of futures etc…rebalancing…
Expect crazy volume and huge moves, and a giant explosion at the close…some orders must be made in the form “market on close” by law or stated guidelines.
I know you have decided not to reply to me, so no worries.
I broke my promise not to comment any more here just for you.
Stay safe.
Mr. Mosher: So being informed excludes being afraid? Did Inchon have no cases from before the one ding from Mapo? Anyway, having some fear about this does not make one a coward, means having sense.
But in your life’s education, have you come across a story about a boy who cried wolf? We’ve seen you here crying wolf for many years re: AGW and ignore the facts that adjustments all tend toward your bias. Ignore all signs of benefits to humans of CO2 for plants and warming, while refusing to see that the green solutions to this CO2 crisis are far worse than any problem it could cause. So please forgive us if we hear you say “wolf” again.
You say “plan”. Okay, let’s plan. Let’s say fighting a contagious disease (this one or the next- you agree there will be a “next” right?) is easier when our electric grid is at it’s most reliable. How shall we plan that? It’s clear to any who look that coal, NG (even oil at $20/barrel) is reliable grid worthy cost effective elec. production, and up-front capital costs for wind/solar more costly and need backup. Freeing up money to test for Wuhan virus on bigger scale. What’s the plan?
I wonder – dumbass – how many things in that range are more likely to kill you than coronavirus. .
Yeah, I’m sticking with coward – but I think ‘dumbass’ a nice addition too.
Careful not to step in front of a bus while you’re checking all those virus alerts.
Touched a button, didn’t I?
And by the way, I’m sticking with ‘coward’ – your entire life has been about spreading amorphous terror and paranoia – and then control-freaking over it – you deserve your life.
The Best Gin and Tonic in the World:
10 oz bottle of Tonic* water
4.5 oz (3 shots) gin**
1 oz. Triple Sec
High Ball Glass with ice.
Pour the Triple Sec and the Gin into a suitable mixing container*** and stir,
Add the Tonic Water and stir.
Pour the libation into the glass with ice.
*I prefer Schweppes.
**Tanqueray is my favorite.
***I use a 16oz Pyrex Measuring Cup. Remember the recipie calls for 15.5 oz of ingredients.
I’ll have 2 of those, shaken not stirred, if you please.
As one gets older one relates more and more with those that lived through traumatic events in history. Recently I went through every available doc on WW1. It became as those boys and girls, Mums and Dads, were right here and now.
Toughen up folks. They did.
This is nothing new within human history.
Two other medications along with Chloroquine: Nivaquin and Camaquin. Not certain of the spelling.
Seismic crews working in the tropics learned all about the taste of these tablets. Me? Papua/New Guinea, later Borneo – in the 1960’s.
I wonder why this news is all over scientific journals, and yet there is a deafening silence from the mainstream media…?
That’s because journalists don’t read websites like this and they set up contact systems that completely insulate them from the general public. Try contacting a journalist on a modern newspaper; it is all but impossible.
Every British media organization has been fully informed about this (by me), yet they continue to ignore it.
Generating national hysteria is so much more fun and profitable for them, so why end the party?
Congratulations Sasha, I tried to inform the Telegraph and utterly failed to speak to anyone. I am glad someone has done it.
See 1:36:10 of Presidential News Conference today in the Washington Post video:
https://www.youtube.com/watch?v=e7QRV4IEf9k
The President evidently asked about Chloroquine this morning during his briefing with scientists. It’s on the radar at least. The answer given by Dr. Birx underplayed its potential by suggesting Chloroquine has only been tested in vitro and in animals. She’s wrong.
It was apparently utilized widely as part of Korea’s nation-wide regimen in mid-February, and afaik, part of their successful “bending” of their own curve of infections. Thus there should be a large body of “in vivo” human test subjects from which to derive medical evidence – not “proof” of efficacy, but enough indication to begin a very large, voluntary test here in U.S.
She’s trying to please the Pres with her nods to his declarations in every sentence, but this, imo, is a failure to dig a little deeper.
I spoke to a board-certified infectious disease specialist who says big pharma and its minions would not like the idea of a dirt cheap pill, taken 2 x’s / day along with a vitamin Zinc that might slow or stop this virus, especially when they have billions riding on expensive remedies still bogged down in various phases of testing with the FDA.
This doctor said, “Now is the time for NIH and VA to step in with funding a clinical trial ASAP.” He went on to say, “If I got the virus I would be strongly tempted to take either chloroquine or hydroxychloroquine if I could get my doctor to prescribe it for me.”
Such a prescription would be considered “off use”, and docs might not do it for fear of complications. It also might not work at all. But I have to wonder why WHO cannont gather that information from both Chinese (who wrote the initial reports on Chloroquine treatment) and S. Koreans, who used it broadly, to synthesize statistical findings of its use – and effectiveness – in those countries.
Go to clinical trials dot gov and see how many trials the Chinese are conducting.
It is a lot.
Evidently they do not think this stuff is the answer.
Trials like that have to eliminate confounding factors, so they cannot give chloroquine to people in trials for other things.
Read between the lines.
This stuff might help some people with some of their symptoms.
But unless it is quantified and compared with something else in a double blind trial, anyone familiar with all of the facts knows it is very hard to be very sure of anything.
Most people getting close attention and supportive care survive…the vast majority.
Some people get well quickly, some take a long time to get well. Some die quickly. Some die after a long time of being sick, sometimes they were very sick the whole time, sometimes it seemed like they were not too bad off and then they suddenly took a turn for the worse and died.
Without documentation and numbers, it is not much more than a reason to take a close look at it…IOW do some damn clinical trials.
Ultimately, it is very likely combinations of drugs will be required, and also some way to identify people quickly and get them started.
Many who survive will have reduced function, perhaps for life in some cases.
There are decades and decades of reasons for doing things a certain way, and many reasons to be skeptical until a result is quantified and confirmed by multiple cohorts and the data reviewed by someone not involved in the care of the patients or the production of the drug.
As for anyone worried no one is studying this…there are at least three studies for this stuff to treat Wuhan Flu.
And many many in using to for other viral infections, like AIDS and such, and to see how it may help with vaccines, etc.
There are always people checking on things, and others who get real excited by a preliminary result and extrapolations or expectations and even wishful thinking>
Nothing wrong with being optimistic.
But there is science, and there is everything else.
https://clinicaltrials.gov/ct2/results?term=chloroquine&cond=Coronavirus
Trump is going to have a news conference in the moringing with the FDA and it looks like he will be addressing these issues, perhaps lifting some regulations that might stand in the way of testing all these different methods.
That Malaria/Covid-19 comparison of Roy Spencer’s is pretty striking. Keep your fingers crossed.
Given what ‘quick’ means to the FDA, it might be easier to relabel COVID-19 as “Chinese malaria virus”
Not quite. The Daily Mail has this article:
https://www.dailymail.co.uk/news/article-8117891/The-promising-therapies-tested-coronavirus-patients.html
No it’s because they are being responsible, the effectiveness has not been scientifically tested. Just because some quack doctor says something and claims something doesn’t make it so …. a lesson that in climate science we have seen over and over.
You need proper clinical trials before giving false hope and that is the process that will be underway.
Belgium appears to have come out with a recommendation to use Chloroquine – in marked contrast to other countries who are maintaining an official silence. It must now be considered as the leading contender for Covid-19 treatment. Clinical trials are starting to report successes. The mainstream media and central governments are still silent.
https://epidemio.wiv-isp.be/ID/Documents/Covid19/COVID-19_InterimGuidelines_Treatment_ENG.pdf
I’ve had a read of the Belgian document. In recent weeks, I’ve become quite adept and reading and judging technical documents outside my field of expertise. It looks to me as though this is good, proper and professional work from the Belgians – something we all need a lot more of in all disciplines, not just in medicine.
The kicker for me is at the bottom of page 4: “It is important for the clinician to be aware that the critical period for complications is 5 to 7 days after symptom onset.” That tallies with my own experience, as I’m more and more coming to suspect that I actually had this thing (very mildly) way back at the end of January, around the same time that the first UK confirmed case was reported. The worst part was the cough on the seventh day, after the initial mild fever/cold had already run its course.
Given that onset period, their treatment recommendations in Table 2 on page 5 seem to hit the mark exactly. Looking at Annex 2, the Dutch also seem to be getting it right. I think they ought to be circulating this to every physician in Europe.
Exactly what I noticed, and a few colleagues.
One put’s it down to the “usual” colds, but somehow more persistent and thoroughly aggravating.
Never had pneumonia, or a bad ‘flu (fingers crossed), but began to wonder about that.
I am beginning to wonder if I had it in mid-February. Woke in the night with a huge fever, woke again hours later with ‘fever gone’, blinding headache for two days, serious dose of the runs. I still have the low energy levels that I associate with flu recovery.
I am holding my breathe every morning ans timing it. So far the times are getting longer, I will be back to the 3 minutes of my swimming days at this rate. If it suddenly starts to get worse I know I am starting pneumonia.
Dodgy,
Read it more carefully.
It says what everyone has known for weeks and the CDC has been saying and lots have talked about.
Remdesivir is not widely available in sufficient quantity, and is being reserved for the most severe cases.
If remdesivir is not available, give (hydroxy)chloroquine. If remdesivir becomes available, switch to it.
What must now be considered is that remdesivir is the leading candidate for a drug that will save lives of patients with Wuhan Flu.
For being who are having organ failure, it says, it is preferable not to use chloroquine since:
“However, since the clinical
efficacy of
(hydroxy)chloroquine is not
demonstrated, caution is
required in case of kidney/
liver/cardiac failure, and abstention in such situations is
preferred”
Nothing new here.
But it is summarized in a very organized way.
I think it is a sure bet that every ER in the world has a similar document guiding care.
Look at annex 2: In all four countries, Remdesivir is the preferred treatment for the most severe patients.
Once it is approved, which it seems very likely to be, it will be the first choice for everyone if it is the best drug for the purpose.
Unless someone would rather save some money I guess.
The problem could be supply, but as I reported here over a month ago, Gilead has, since January, enlisted several facilities around the world to manufacture remdseivir, and switched one US factory from something else to full time remdesivir production, and another in the US that was idle was activated for purpose and has also been making it 24/7 since January…so hopefully there is plenty.
Gilead is being cautious with teh protocol because they have decades of experience with making sure that once they know…they KNOW, and can prove it beyond doubt.
It sounds to me like they have known it for months, and have said all they can, legally and ethically.
Read between the lines.
There are people who are very smart and very experienced in virology, new drug approval, and how and why antiviral medications work and when.
I am sure of a few things, and among them is that this entire situation will have moved the whole world way ahead in the fight against infectious diseases, just as AIDS, HCV, and Ebola have done previously.
Ten years from now things will be different.
There is also a chance that remdesivir will be found to be inferior to choloroquine.
But who they are giving what at this stage makes me think some knowledgeable people know some things they are not at liberty to say right now.
I do not think the Swiss are giving their people something based on profit motive.
Maybe I am naive.
But I tend to think some people are more intelligent than they are greedy or heartless.
“The problem could be supply, but as I reported here over a month ago, Gilead has, since January, enlisted several facilities around the world to manufacture remdseivir, and switched one US factory from something else to full time remdesivir production, and another in the US that was idle was activated for purpose and has also been making it 24/7 since January…so hopefully there is plenty.”
That’s good news.
Just to be clear, this set of guidelines makes it clear exactly why anecdotal evidence will often give a skewed perspective.
The sickest people are being triaged to receive a different treatment.
So that means the people getting the malaria drug are not as bad off to begin with.
And only the worst off are at risk of dying.
And bias like this will not let a valid comparison to be made…it is the definition of comparing apples and oranges.
The Ebola trials was a perfect analogy for this entire discussion.
One treatment worked great.
But two others were even better.
The one that works great was therefore deemed to not be the best choice.
I think everyone wants to best choice.
We also need to know when the stuff that is cheap pills will be preferred, and how much benefit it provides.
Only quantified results from objectively performed study can reveal these important details.
How can anyone know at this point which is better and should be the stuff factories are cranking out?
Is vitamin C in high dose IV better than chloroquine?
Only a study can tell us.
If they are equal, which is better?
The ultrasafe for everyone vitamin, or the kind of safe stuff that is OK for many but very dangerous for a few?
If remdesivir is the best choice, can it be made into a pill?
The sooner the first questions have an answer, the sooner other questions can be looked at…like which two things used together is best of all?
We need a baseline of data to find out.
Random anecdotal evidence will never reveal precisely what is best and when.
Update of the Belgium document for use by ER personnel: Note that the document has been extensively revised and a bunch of far more cautious language has been added, as of 3-24-20.
https://epidemio.wiv-isp.be/ID/Documents/Covid19/COVID-19_InterimGuidelines_Treatment_ENG.pdf
In case anyone is tempted to home medicate:
” the margin between the therapeutic and toxic dose is narrow and chloroquine
poisoning has been associated with cardiovascular disorders that can be
life-threatening (Frisk-Holmberg et al., 1983). Chloroquine and hy-
droxychloroquine use should therefore be subject to strict rules, and
self-treatment is not recommended.”
https://doi.org/10.1016/j.antiviral.2020.104762