UPDATE: A Covid-19 case correlation between malarial and non-malarial countries has been plotted by Dr. Roy Spencer, and the results are stunning – see below.
Encouraging news: three new medical studies show a commonly available anti-malaria drug known as chloroquine aka chloroquine phosphate is showing strong results against COVID-19 infections in both China and South Korea. Excerpts from three studies, including one published in Nature are below.

An Effective Treatment for Coronavirus (COVID-19)
Presented by: James M. Todaro, MD and Gregory J. Rigano, Esq.
In consultation with Stanford University School of Medicine, UAB School of Medicine and National Academy of Sciences researchers.
Translation by: Celia Martínez-Aceves (Yale B.S. Candidate 2021), Martín Martínez (MIT B.S. 2017)
Summary
Recent guidelines from South Korea and China report that chloroquine is an effective antiviral therapeutic treatment against Coronavirus Disease 2019. Use of chloroquine (tablets) is showing favorable outcomes in humans infected with Coronavirus including faster time to recovery and shorter hospital stay. US CDC research shows that chloroquine also has strong potential as a prophylactic (preventative) measure against coronavirus in the lab, while we wait for a vaccine to be developed. Chloroquine is an inexpensive, globally available drug that has been in widespread human use since 1945 against malaria, autoimmune and various other conditions.
Chloroquine: C18H26ClN3
Background
The U.S. CDC and World Health Organization have not published treatment measures against Coronavirus disease 2019 (“COVID-19”). Medical centers are starting to have issues with traditional protocols. Treatments, and ideally a preventative measure, are needed. South Korea and China have had significantly more exposure and time to analyze diagnostic, treatment and preventative options. The U.S., Europe and the rest of the world can learn from their experience. According to former FDA commissioner, board member of Pfizer and Illumina, Scott Gotlieb MD, the world can learn the most about COVID-19 by paying closest attention to the response of countries that have had significant exposure to COVID-19 before the U.S. and Europe.[1]
As per the U.S. CDC, “Chloroquine (also known as chloroquine phosphate) is an antimalarial medicine… Chloroquine is available in the United States by prescription only… Chloroquine can be prescribed for either prevention or treatment of malaria. Chloroquine can be prescribed to adults and children of all ages. It can also be safely taken by pregnant women and nursing mothers.”[2]
CDC research also shows that “chloroquine can affect virus infection in many ways, and the antiviral effect depends in part on the extent to which the virus utilizes endosomes for entry. Chloroquine has been widely used to treat human diseases, such as malaria, amoebiosis, HIV, and autoimmune diseases, without significant detrimental side effects.”[3]
The treatment guidelines of both South Korea and China against COVID-19 are generally consistent, outlining chloroquine as an effective treatment.
Specifically, according to the Korea Biomedical Review, in February 2020 in South Korea, the COVID-19 Central Clinical Task Force, composed of physicians and experts treating patients agreed upon treatment principles for patients with COVID-19.[4] In China, the General Office of the National Health Commission, General Office of the State Administration of Traditional Chinese Medicine as well as a Multi-Center Collaborative Group of Guangdong Provincial Department of Science and Technology and Guangdong Provincial Health Comp and the China National Center for Biotechnology Development have established effective treatment measures based on human studies.[5]
According to their research (reported in Clinical Trials Arena),
“Data from the drug’s [chloroquine] studies showed ‘certain curative effect’ with ‘fairly good efficacy’ … patients treated with chloroquine demonstrated a better drop in fever, improvement of lung CT images, and required a shorter time to recover compared to parallel groups. The percentage of patients with negative viral nucleic acid tests was also higher with the anti-malarial drug… Chloroquine has so far shown no obvious serious adverse reactions in more than 100 participants in the trials… Chloroquine was selected after several screening rounds of thousands of existing drugs. Chloroquine is undergoing further trials in more than ten hospitals in Beijing, Guangdong province and Hunnan province.”[6]
…
Chloroquine as a prophylactic (preventative) measure against COVID-19[11]
According to research by the US CDC, chloroquine has strong antiviral effects on SARS coronavirus, both prophylactically and therapeutically. SARS coronavirus has significant similarities to COVID-19. Specifically, the CDC research was completed in primate cells using chloroquine’s well known function of elevating endosomal pH. The results show that “We have identified chloroquine as an effective antiviral agent for SARS-CoV in cell culture conditions, as evidenced by its inhibitory effect when the drug was added prior to infection or after the initiation and establishment of infection. The fact that chloroquine exerts an antiviral effect during pre- and post-infection conditions suggest that it is likely to have both prophylactic and therapeutic advantages.”
The study shows that chloroquine is effective in preventing SARS-CoV infection in cell culture if the drug is added to the cells 24 h prior to infection.
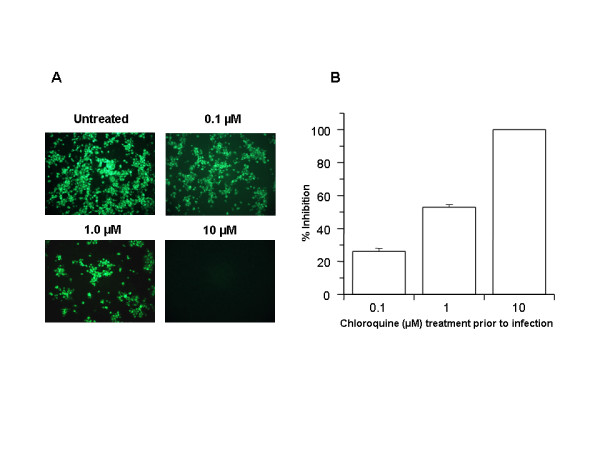
FIGURE 1
Prophylactic effect of chloroquine. Vero E6 cells pre-treated with chloroquine for 20 hrs. Chloroquine-containing media were removed and the cells were washed with phosphate buffered saline before they were infected with SARS-CoV (0.5 multiplicity of infection) for 1 h in the absence of chloroquine. Virus was then removed and the cells were maintained in Opti-MEM (Invitrogen) for 16–18 h in the absence of chloroquine. SARS-CoV antigens were stained with virus-specific HMAF, followed by FITC-conjugated secondary antibodies. (A) The concentration of chloroquine used is indicated on the top of each panel. (B) SARS-CoV antigen-positive cells at three random locations were captured by using a digital camera, the number of antigen-positive cells was determined, and the average inhibition was calculated. Percent inhibition was obtained by considering the untreated control as 0% inhibition. The vertical bars represent the range of SEM.
…
In addition, the study also shows that chloroquine was very effective even when the drug was added 3–5 h after infection, suggesting an antiviral effect even after the establishment of infection.
…
The UK has banned the export of Chloroquine[13]
As of February 26, 2020, the UK government has added chloroquine to the list of medicines that cannot be parallel exported from the UK. Chloroquine was never on this list before. This likely happened because of the growing body of evidence of chloroquine’s effectiveness against coronavirus.
China prioritizes internal use of Active Pharmaceutical Ingredients (APIs) including Chloroquine[14]
In early February, Chongqing Kangle Pharmaceutical was requested by the Ministry of Industry and Information Technology, Consumption Division to promptly increase the manufacturing and production of the active pharmaceutical ingredients chloroquine phosphate despite slowed production during the Chinese New Year.
…
Conclusion
Chloroquine can both both prevent and treat malaria. Chloroquine can prevent and treat coronavirus in primate cells (Figure 1 and Figure 2). According to South Korean and China human treatment guidelines, chloroquine is effective in treating COVID-19. Given chloroquine’s human safety profile and existence, it can be implemented today in the U.S., Europe and the rest of the world. Medical doctors may be reluctant to prescribe chloroquine to treat COVID-19 since it is not FDA approved for this use. The United States of America and other countries should immediately authorize and indemnify medical doctors for prescribing chloroquine to treat COVID-19. We must explore whether chloroquine can safely serve as a preventative measure prior to infection of COVID-19 to stop further spread of this highly contagious virus.
Full study available here
Then there’s this second study:
Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studiesJianjun Gao, Zhenxue Tian, Xu Yang
Abstract
The coronavirus disease 2019 (COVID-19) virus is spreading rapidly, and scientists are endeavoring to discover drugs for its efficacious treatment in China. Chloroquine phosphate, an old drug for treatment of malaria, is shown to have apparent efficacy and acceptable safety against COVID-19 associated pneumonia in multicenter clinical trials conducted in China. The drug is recommended to be included in the next version of the Guidelines for the Prevention, Diagnosis, and Treatment of Pneumonia Caused by COVID-19 issued by the National Health Commission of the People’s Republic of China for treatment of COVID-19 infection in larger populations in the future.
https://www.jstage.jst.go.jp/article/bst/14/1/14_2020.01047/_article
Finally, there’s a new study in the prestigious journal Nature:
Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro
Excerpt:
Chloroquine, a widely-used anti-malarial and autoimmune disease drug, has recently been reported as a potential broad-spectrum antiviral drug.8,9 Chloroquine is known to block virus infection by increasing endosomal pH required for virus/cell fusion, as well as interfering with the glycosylation of cellular receptors of SARS-CoV.10 Our time-of-addition assay demonstrated that chloroquine functioned at both entry, and at post-entry stages of the 2019-nCoV infection in Vero E6 cells (Fig. 1c, d). Besides its antiviral activity, chloroquine has an immune-modulating activity, which may synergistically enhance its antiviral effect in vivo. Chloroquine is widely distributed in the whole body, including lung, after oral administration. The EC90 value of chloroquine against the 2019-nCoV in Vero E6 cells was 6.90 μM, which can be clinically achievable as demonstrated in the plasma of rheumatoid arthritis patients who received 500 mg administration.11 Chloroquine is a cheap and a safe drug that has been used for more than 70 years and, therefore, it is potentially clinically applicable against the 2019-nCoV.
Our findings reveal that remdesivir and chloroquine are highly effective in the control of 2019-nCoV infection in vitro. Since these compounds have been used in human patients with a safety track record and shown to be effective against various ailments, we suggest that they should be assessed in human patients suffering from the novel coronavirus disease.
A commonly available over-the-counter quinine source exists in Margosa Tree Bark and Cinchona succirubra, Peruvian Bark


Tablets of bark extract are widely available in tablet form, from many sources, including Amazon.com here.
There’s also quinine in Tonic Water, which is available just about anywhere at any grocery or liquor store and also at Amazon:
Tonic water is a soft drink containing quinine, which gives it a bitter taste. Quinine is a common treatment for malaria. Quinine comes from the bark of the cinchona tree.
UPDATE:
From Facebook, Dr. Roy Spencer adds this new information.- Anthony
On the subject of using antimalarial drugs for COVID-19 treatment, I’ve compared COVID-19 cases versus malaria incidence by country….
This is amazing. I downloaded all of the data for 234 countries, incidence of total COVID-19 cases (as of 3/17/2020) versus the incidence of malaria in those countries (various sources, kinda messy matching everything up in Excel).
RESULTS, Multi-country average malaria cases per thousand, COVID-19 cases per million, in three classes of countries based on malaria incidence:
- Top 40 Malaria countries: 212 malaria = 0.2 COVID-19;
- Next 40 Malaria countries: 7.3 malaria = 10.1 COVID-19
- Remaining (81-234) countries: 0.00 malaria = 68.7 COVID-19
Again, the units are Malaria cases per thousand “population at risk”, and COVID-19 cases per million total population.
In all my years of data analysis I have never seen such a stark and strong relationship: Countries with malaria basically have no COVID-19 cases (at least not yet).
Additional support for antimalarial drugs for COVID-19 treatment comes from this investigation linked below.
The map says it all: COVID-19 is where Malaria is not.

The bio-chemistry behind the Chloroquine (Zinc Ionophore) treatment is well described by Dr Seheult on the MedCram Coronavirus Pandemic Updates 32 & 34.
Watch this to get a great education on how the virus replicates and why chloroquine will cure it in the cell.
Thanks for this. It appears Koreans are using this in combination with hiv type anti virals as both affect different parts of viral replication. One thing HUV brought the world was greater understanding of viruses.
I would be very cautious drawing conclusions about efficacy with the current data. Without doing well designed, randomized, blinded studies it is not at all certain that anecdotal observations of efficacy are true representations of a drug’s value. I am an infectious disease physician and no routine therapeutics are considered indicated as yet for covid-19 except in desperation for patients who are at risk of respiratory failure or death. The vast majority of patients are treated supportively and do just fine. It is too early to draw any conclusions about effective therapies.
I agree but what if a person is very old or has underlying conditions. Would you give it ?
There is zero “well designed, randomized, blinded studies”, or even real studies showing radon in homes is a cancer risk, but that never prevented your EPA from inciting home owners to perform expensive transformations to eliminate that risk. Who is at risk? Those who have “bad genes”? Could that be those who are at risk of breast cancer? See where I’m going?
The request for “well designed, randomized, blinded studies” before something is prescribed is capricious. Where is the evidence that the US treats cancer better than other nation, as peddled by Donald “Big Medicine” Trump? Where is the evidence that all these drugs given to children are not damaging their mind and long term health? I could go on and on and on and on.
“I could go on and on”
And you usually do.
Where is the evidence that the US treats cancer better than other nations?
Survival and cure rates
Where is the evidence that chemo therapies aren’t harming the long term health of children.
1) The studies as well as follow up studies.
2) Would you prefer to have the kids die, rather than have a very small risk of long term complications?
My wife had small cell lung cancer(smokers cancer) even though she did not smoke. That was 20 years ago, she got chemo and radiation therapy at the same time, yes it did affect her, but she is here 20 years later, thirteen years earlier my dad had the same cancer the treatment did not work on him he was a smoker it it was found late. He passed away nine months from his original diagnoses. It would have been nice had the treatment would have work no-mater what damage they would have done, if they had there a good chance he would have lasted twenty years longer. even five would have been nice. Chemo and radiation are a poor way to treat cancer but in most cases that all we got.
Mark is NIceGuy right about radon?
I have never really understood radon.
Radon is assumed to be a risk because it’s radioactive.
It’s a case of the old bug-a-boo, Linear No Threshold (LNT) thinking.
It is assumed that if a large dose of radiation is enough to kill one person, then if 1% that level of radiation is given to 100 people, there will be one extra cancer death.
If 1 millionth that level is given to 1 million people, there will still be one extra cancer death.
Of course the science shows that thresholds do exist and that low levels of radiation are not as dangerous as the activists want to believe.
“Survival and cure rates”
show that in the US people spend money to be drugged and cut and have their healthy lifetime wrecked by medical doctors with zero evidence of avoiding any cancer and lots of evidence of causing more cancer.
“Where is the evidence that chemo therapies aren’t harming the long term health of children.”
Are you willing to go through chemo right now, then?
I’ve seen comments from doctors who say that few doctors will use hydroxy-chloroquine or chloroquine phosphate since there is no FDA approval of those drugs for this type of treatment.
amazing how fast they can OFFlabel approve things
and heres the other product for malaria
wether its at all the same in effect I dunno
but it works for malaria,
https://www.drugs.com/npp/sweet-wormwood.html
The news just came out, and you are whining that they haven’t given off label approval yet.
actually offlabel for plaquenil is already in place ie RA immune skin disorders etc in usa
ozspeaksup
As I recollect, wormwood was what made absinthe poisonous. But then, “The poison is in the dose.”
So is absinthe, therefore potentially better than gin and tonic as a treatment?
mario
I don’t know. I’ve never even tried it. I believe it is illegal in most jurisdictions.
Clyde: I had some in Monterrey a few years ago. I also got a bit drunk. It was hard to tell, but it seemed like a different kind of drunk. Was it placebo? I dunno, bit I needed a few Advil in the morning.
Absinthe has been available again in France for a few years now.
And here in the US too… I had some several years ago and posted about that higher up in this post.
Mario
I believe I remember reading that what is available in the US is created the same way as the original, but is not aged in wormwood casks as was the tradition.
OK, I decided to take the time to educate myself (or at least become as educated as Wikipedia allows): https://en.wikipedia.org/wiki/Absinthe
It certainly has a colorful history, if you will pardon the pun.
I did skim that… so sure we now cut corners but, it is mostly the same. And I was being a bit rhetorical with the question… like, I am not going to go start getting drunk unless this shelter in place goes a lot longer. Then maybe… sarc/ 🙂
Many traditional treatments for malaria work by interrupting the development cycle of the parasite (which is very complex). Wormwood may be working on a different mechanism than the antiviral one. Malaria is, after all, not a virus.
It is speculated that any malaria treatment that modifies two genetic mechanisms in the mosquito simultaneously will prevent it being able to mutate successfully around both. The problem is the mosquito which is unique in its inability to resist the pathogen. If we “fix” the mosquito’s normal body protection mechanisms the disease will disappear.
Legally any doctor in the US can prescribe any medication for anything that is appropriate in the judgement of that doctor, and this is not subject to any restrictions.
Doctors can prescribe any approved medication as they see fit.
That is the law.
But no one is gonna shield anyone from liability for giving something that harms them, or when something better was available.
It is important to know the specifics, or all you have is opinions.
Andy Pettullo is exactly right.
We already know the vast majority of patients recover.
So patients recovering proves exactly nothing, as does in vitro studies.
There is a very long list of stories that amply demonstrate why this is critically important to get right.
Now is not the time to get anything wrong.
It never is, but higher stakes means we need to be more careful, although surely we should also not be dragging feet.
At this point the panic is clearly more harmful than the disease, even to the elderly who are seeing their life savings evaporate. The worst case scenario of giving everybody chloroquine would be that it doesn’t change any clinical outcomes but a lot of people stop panicking because now they have a “cure” (although just a placebo). If it is effective, then it would be a huge benefit.
I suspect that we will be hearing more about this tomorrow in the FDA press conference.
If someone takes two much because “If one is good, two is better”, they may die.
Kids have died from as little as twice the recommended dose for an adult.
There are some people that must not take it.
So it could be given, but must be explained and understood by everyone as a powerful drug, which must be used carefully and as directed.
And that is impossible for some people, particularly people who are panicked and hypochondriacs to begin with.
Well, Nicholas, when I carelessly said “giving everybody chloroquine”, I meant administering the drug in a clinical setting, not giving them a bunch of pills to do with as they will. It is after all a prescription drug,
It’s stories like this that ought to put WUWT on the front page of every journalist’s bookmark list in the world. If there was any justice.
Mind you, it is well known that there is no justice…
Looks like there is a slight side effect with the chloroquine it might save you from the virus but you might go blind:
https://play.google.com/store/books/details/David_J_Browning_Hydroxychloroquine_and_Chloroquin?id=C3ceBAAAQBAJ&hl=en-US&gl=us
Dr Norman Page
For the 6 to ten days of treatment, Professor Didier Raoult the director of the Mediterranean Infection Institute in Marseille, has 40 years experience in the field of viruses and diseases….. He has taken chloroquine for long periods of time as he lived in africa, and states that if given the right dose for the symptoms, there is low chance of any aide effect… His clinical trial saw no effects in recovered patients
The risk of Hydroxychloroquine toxicity leading to progressive blindness appears to be very low (particularly in comparison to dying from acute respiratory failure within 21 days of coronavirus infection).
“ retinopathy is most influenced by daily dose and duration of use. Risk for toxicity is less with <5.0 mg/kg real weight/day for hydroxychloroquine and <2.3 mg/kg real weight/day for chloroquine[2]. Patients are at low risk during the first 5 years of treatment. At recommended doses, the risk of toxicity up to 5 years is under 1% and up to 10 years is under 2%, but rises to nearly 20% after 20 years. However, if a patient has not demonstrated toxicity after the 20-year point, he/she only has a 4% risk of developing toxicity the subsequent year.”
From the NIH https://www.ncbi.nlm.nih.gov/pubmed/32164085
You have to use it for years to have foveal damage. I’ve used it several times for several months back when it was the standard malaria prophylaxis. No side effects at all.
That means YOU have to, not necessarily any generic you.
The side effects are very well known. They are not listing them to be pedantic.
Side effects can be a bit rough if memory serves..
But it was way better than malaria
If this turns out to be valid — and is rapidly adopted as a recommended preventive, it might actually help flatten the curve in the US and elsewhere.
I’d give this a couple of weeks to see if it gains traction.
I have tested positive for malaria for most of my life, since being in North africa in the early 70s….tonic water is my treatment if I begin to feel a bit hinky…..
I don’t put a lot of faith in it Kip….studies about this came out months ago….and they are still not doing it
We’ve only known about this disease for months.
I’ve just ordered 3 x 60 tablets of Quinine Sulfate, might give it a try when the UK’s rate of infection (2000) reaches the current rate of France or Germany (6000+), hopefully the QS is less deadly than covid-19.
Apparently it is used for treating malaria caused by the protozoa Plasmodium falciparum and falciparum malaria resistant to the drug chloroquine
more details here
Chloroquine phosphate is what I use to treat my aquarium fish. I have a bunch on hand.
BTW, somewhat off topic, but does anyone actually know what the Covid-19 hospitalization rate is in the U.S.? This seems like extremely important information and I can’t track it down.
What is the product?
Do NOT eat that aquarium cleaner. It’s completely different and it’s toxic. A man and his wife tried it, he died, she’s critical.
I’ll stick with Zn+Quercetin+CoQ10+EGCG
See Medcram update #35
The raids in stores went for the wrong items. They left the over the counter supplements.
I noticed that all the vitamin C was gone at Walmart. Grape seed extract is loaded with vitamin C and is sold in capsules, and orange juice is readily available.
I expect they will make more vitamin C for the Walmart.
Where did CoQ10 come in all this? Seen Medcram and all this about Zinc and its ionophores to get it inside cells, but never saw anything about CoQ10 in there.
Good news about chloroquine. The cost for Corvid is greater than the medical issues.
The idiots that made up CAGW are activists. Activists cannot understand the big picture as they filter out facts and just repeat their propaganda.
Countries have two crises which they must all face due to Corvid.
Corvid isolation economic effects will wipe out roughly 15% the world GDP (based on China’s experience and effects on world tourism) a time when every developed country and their citizens are deeply debt.
The companies that are effected by Corvid isolation have debts and no revenue. Airline companies are laying off 50% of their staff. Tourism companies are closing.
The economic impact of Corvid isolation is until the developed world is vaccinated. Say 1 ½ years?
International air traffic has almost stopped … Hotels are closing. Movie theatres are all closed. All sporting events, all concerts, and so on.
Opel, Ford anf VW closed factories today in Germany.
Every major city, in the world, is now in virus isolation shutdown mode.
https://www.bbc.com/news/in-pictures-51914110
This is not an economic downturn.
This is a paradigm change.
Boeing cannot sell planes to bankrupt airline companies that have thousands of unused planes.
Tourists do not want to travel and cannot travel until there is a vaccine. International air travel is over until there is a vaccine.
There is no alternative to extreme isolation until there is a vaccine.
This is not the reduction of growth. This is the instant and long-term destruction of demand.
It is a frickin disaster.
Hard to see how it ends, but I am hoping a successful drug that helps most people with the most severe symptoms, in other words those about to die, will have a decent chance of turning it around quickly. The longer it drags on, the worse off we all will be.
This could literally be the worst economic disaster in the history of the world…another great depression.
I have no idea what the chances of that are, but it is for sure nothing like this has ever happened before.
I’m guessing there is some great NATURAL source that nobody is eating but everybody should.
So Gin and Tonic all round?
As a precautionary tactic of course.
Sure this might be aside track a red herring but the suggested precaution is mighty palatable to many..
Willis’s numbers from the cruise ship were quite interesting,we do seem to be panicking in a manner contrary to what the number seem to tell us.
However being hardwired for flight or fight a much publicized pandemic is hard to rationally respond to.
The Therapeutic Index of Plaquenil is fairly high (that’s a good measure of safety). Serious short term adverse effects are very uncommon (the chief concern of long term retinal toxicity is also fairly uncommon…and can be monitored for early detection)…so, I would not hesitate taking up to 300mg daily for Coronavirus prophylaxis (200mg daily should be effective from what I’ve read so far).
China and the UK are now hoarding these agents (chloroquine and hydroxychloroquine). I don’t know of any US domestic production capabilities…so the supply in the US may be limited, though it is a very commonly used drug.
It wouldn’t hurt to ask your physician to consider putting you on these agents if you begin having suspicious symptoms…and even just for prevention if your doctor is willing. This is not medical advice. I’m only suggesting advice and action you might ask for from your physician.
It seems very safe, especially compared to some of the other candidate drugs they are looking at.
Please note the contraindications and potential drug interactions:
https://www.pdr.net/drug-summary/Chloroquine-Phosphate-chloroquine-phosphate-3418
The side effects look lovely. I’ll pass.
It is actually a quite safe drug. I’ve taken it for longish periods (months) several times back when it was the anti malarial drug of choice. No side effects whatsoever.
Mefloquine is a lot worse, I personally don’t react to it, but I’ve known people go more or less psychotic from using it.
Some people took interferon and ribavirin with few side effects.
Others killed themselves.
It was so common that suicidal ideation was listed as a side effect, and everyone who got it was counselled prior to being given the stuff and quizzed regularly about thoughts of self harm.
Other got hemolytic anemia, and all sorts of other things.
Destroyed thyroid gland, diabetes,” too many to name, many quite severe and many people simply had to stop taking it. Most had to stop working for the full 24 or 48 weeks.
But hey some had nothing much happen.
I am not suggesting chloroquine has anything like that safety profile, just that you cannot call it safe and free of side affects simply because you did not have any.
recent one that young UK lass who threw herself out of a small plane in sth america
had been acting weird but no one twigged it ws the antimalarial meds
That, most probably, was the naughty one – Lariam.
A guy I knew took that, and had a fortnight [I think, this was about 1999] off work.
I have taken chloroquine perhaps a dozen times, and – for me – there has been no obvious side-effect.
YMMV.
Auto
Thanks for the link, but…
“Bradycardia, cardiac arrhythmias, cardiac disease, coronary artery disease, females, heart failure, hypertension, hypocalcemia, hypokalemia, hypomagnesemia, long QT syndrome, malnutrition, myocardial infarction, QT prolongation, thyroid disease
Use chloroquine with caution in patients with cardiac disease or other conditions…”
…being female is now a condition?
It is passed into breast milk and may be a mutagen and have teratogenic effects. It is also a possible carcinogen.
At first I thought it was a typo, but your explanation makes sense, thanks.
You trimmed part of the text. Let’s see it all, please.
the text I trimmed is from the post that I was responding to. The complete text is there: https://www.pdr.net/drug-summary/Chloroquine-Phosphate-chloroquine-phosphate-3418
These findings re zinc video are very interesting. In the 90’s I published 2 papers in Veterinary Immunology and Free Radical Research (Elsevier) data showing that even slight stress basically dropped serum zinc values ~100 percent over 2-3 days in sheep. Im surmising that in older people zinc levels need to be boosted. The chloroquine + Zinc story makes sense for treatment I am surmising of course as our research was with sheep but these recent publications seem to support the findings.
Dropped levels 100%?
100% means all of their zinc went away.
I am pretty sure anything which is a necessary nutrient will cause rapid if not instant death if 100% of it was eliminated.
Zinc is essential in over 300 enzymes and over 1000 transcription factors.
It is the second most abundant trace metal in the body after iron.
It is required in every enzyme class.
I think the actual number is not 100%
What were the symptoms of 100% Zn depletion? Asking for a friend.
So not even a pandemic can get the medical community and regulators to look at the research on vitamin supplements. That’s a shame that historians can write about later.
This is not new and has been known for over a decade.
https://aac.asm.org/content/53/8/3416
That quinine is effective against certain types of coronavirus may have been known for a decade. Whether it is effective against COVID-19 in particular would not have been.
“In conclusion, we demonstrate here that chloroquine shows strong in vitro and in vivo antiviral activities against HCoV-OC43. Moreover, treatment with daily doses of chloroquine has a long-lasting protective effect against lethal coronavirus OC43 infection in newborn mice.”
“ACKNOWLEDGMENTS
This work is part of the activities of the Euro-Asian SARS-DTV Network (SP22-CT-2004-511064) supported by the European Commission specific research and technological development program “Integrating and Strengthening the European Research Area.” This work was supported by a postdoctoral fellowship of the Fonds voor Wetenschappelijk Onderzoek (FWO)-Vlaanderen to Piet Maes.”
Hi C-no-evil: – Correct, not a new discovery. See this from 2005: “Chloroquine is a potent inhibitor of SARS coronavirus infection and spread”; free full text is on-line & it’s a relatively easy for non-technical readers to understand.
I see commentators expounding with “… but says who – need data …” & others crediting zinc, “… gotta be with zinc ….” Maybe older published research for this will be of interest to WUWT readers who are just hearing of this drug for coronaviruses.
I could not figure out if Zn and Quinine from tonic water work together to help cells through osmosis increase their Zn levels. Anyone able to provide answers on this topic? If yes, that would be great. I always take Zn supplements about 100% of recommended amount to keep levels from being too low in my body. I take more when sick.
Medcram update #35
Yes I watched that, but could not conclude whether taking small quinine doses via tonic watch provided the right form of quinine to make a difference.
The end of the video shows alternatives with the same biological explanation. Did you stop watching?
“The end of the video shows alternatives with the same biological explanation. Did you stop watching?”
I may have skimmed and thought I got what I needed from it. Thank you I will watch to the end and see if it answers questions about “forms if Quinine.”
There was also a researcher on the Laura Ingraham show on Fox News last night, who mentioned a study where 30 Covid-19 patients treated with chloroquine tested negative after a week, while 30 others given a placebo showed little improvement. Trouble is, Laura Ingraham liked to hear herself talk too much, and didn’t give the researcher enough time to explain the results of his study. I’m not sure whether the study presented by the researcher on Laura Ingraham’s show matches one of the three studies presented in the article above.
If chloroquine has been around for 75 years, and is safe for use against malaria, the FDA should strongly encourage immediate tests of chloroquine on hundreds of other patients known to be suffering from the Covid-19 virus, particularly those with severe cases in areas with high concentrations of infected people (the Seattle area and southeastern New York state). For those elderly Covid-19 patients on ventilators in hospitals, what do they have to lose from taking chloroquine?
If chloroquine can be shown to save some patients’ lives, and result in rapid cures of other patients, there should be a concerted effort to mass-produce chloroquine by any companies that know how to manufacture it as fast as possible and make it readily available to anyone tested positive for Covid-19.
We have all heard these horror stories of exponential growth in cases of Covid-19, of WHO declaring it a “pandemic”, of millions of Europeans holed up in their houses afraid to go out due to this dread disease, the stock market losing 30% in three weeks, “experts” telling us there won’t be a vaccine for 18 months, but Covid-19 has not yet killed 100 people out of 327 million Americans.
If a drug that has been around for 75 years and is safe for curing malaria can be shown to cure Covid-19 and save lives, it could be a serious game-changer, reducing the massive fear and letting people get on with their lives–if they get Covid-19, they get a prescription for chloroquine and get over it!
Immediate test my butt. If they have data that says it may help, start using it and let your clinical experience do the talking.
Once again, Government getting in the way of the solution.
There’s nothing like human guinea pigs. Boy is history replete with examples where that didn’t go so well.
icisil isn’t history full of successes too? Wasn’t the cure for an ulcer done by a guy who figured out how to give himself an ulcer then treat it with antibiotics?
Ulcer treatment was settled science beforehand 😉
In this case it has been tried on “human guinea pigs” for 75 years and is known to be very safe.
For malaria, not for respiratory diseases.
If it’s safe, it’s safe. Period.
The question is does it cure.
See my previous comment about this anti-malarial being hemolytic. I can’t see how that and respiratory diseases go together well.
It sounds like used as directed, for most people most of the time it is safe-ish.
But it is also fatal when overdosed.
How safe is safe?
Put it on the top shelf, if the therapeutic dose is 500mg.
Twice that amount is fatal for a child:
“Professionals FDA PIChloroquine
Print Share
Chloroquine
Generic Name: Chloroquine phosphate
Dosage Form: tablet
Medically reviewed by Drugs.com. Last updated on Oct 1, 2018.
OverviewSide EffectsDosageProfessionalInteractionsMore
On this page
Description
Clinical Pharmacology
Indications and Usage
Contraindications
Warnings
Precautions
Adverse Reactions/Side Effects
Overdosage
Dosage and Administration
How Supplied/Storage and Handling
References
Chloroquine Description
Chloroquine phosphate tablets, Chloroquine phosphate, USP, is a 4-aminoquinoline compound for oral administration. It is a white, odorless, bitter tasting, crystalline substance, freely soluble inwater.
Chloroquine phosphate tablets are an antimalarial and amebicidal drug.
Chemically, it is 7-chloro-4-[[4-(diethylamino)-1-methylbutyl]amino]quinoline phosphate (1:2) andhas the following structural formula:
C18H26ClN3.2H3PO4 Molecular Weight: 515.87
Each tablet contains 500 mg of Chloroquine phosphate USP, equivalent to 300 mg Chloroquine base.
Inactive Ingredients: colloidal silicon dioxide, dibasic calcium phosphate, hydroxypropylmethylcellulose, magnesium stearate, microcrystalline cellulose, polyethylene glycol, polysorbate80, pregelatinized starch, sodium starch glycolate and titanium dioxide.
Chloroquine – Clinical Pharmacology
Chloroquine is rapidly and almost completely absorbed from the gastrointestinal tract, and only a small proportion of the administered dose is found in the stools. Approximately 55% of the drug inthe plasma is bound to nondiffusible plasma constituents. Excretion of Chloroquine is quite slow,but is increased by acidification of the urine. Chloroquine is deposited in the tissues in considerable amounts. In animals, from 200 to 700 times the plasma concentration may be found in the liver,spleen, kidney, and lung; leukocytes also concentrate the drug. The brain and spinal cord, in contrast, contain only 10 to 30 times the amount present in plasma.
Chloroquine undergoes appreciable degradation in the body. The main metabolite is desethylChloroquine, which accounts for one fourth of the total material appearing in the urine;bisdesethylChloroquine, a carboxylic acid derivative, and other metabolic products as yet uncharacterized are found in small amounts. Slightly more than half of the urinary drug products can be accounted for as unchanged Chloroquine.
Microbiology
Mechanism of Action: Chloroquine, a 4-aminoquinoline, is an anti-protozoal agent. The precise mechanism by which Chloroquine exhibits activity is not known. Chloroquine, may exert its effect against Plasmodium species by concentrating in the acid vesicles of the parasite and by inhibiting polymerization of heme. It can also inhibit certain enzymes by its interaction with DNA.
Activity in Vitro and in Clinical Infections: Chloroquine is active against the erythrocytic forms of susceptible strains of Plasmodium falciparum, Plasmodium malariae, Plasmodium ovale, and Plasmodium vivax. Chloroquine is not active against the gametocytes and the exoerythrocytic forms including the hypnozoite stage (P. vivax and P. ovale) of the Plasmodium parasites.
In vitro studies with Chloroquine demonstrated that it is active against the trophozoites of Entamoeba histolytica.
Drug Resistance: Resistance of Plasmodium parasites to Chloroquine is widespread (see INDICATIONS AND USAGE, Limitations of Use in Malaria and WARNINGS).
Plasmodium parasites exhibiting reduced susceptibility to hydroxyChloroquine also show reduced susceptibility to Chloroquine.
Patients in whom Chloroquine or hydroxyChloroquine have failed to prevent or cure clinical malaria or parasitemia, or patients who acquired malaria in a geographic area where Chloroquine resistance is known to occur should be treated with another form of antimalarial therapy (see WARNINGS and INDICATIONS AND USAGE, Limitations of Use).
Indications and Usage for Chloroquine
Chloroquine phosphate tablets are indicated for the:
Treatment of uncomplicated malaria due to susceptible strains of P. falciparum, P.malariae, P. ovale, and P.vivax.
Prophylaxis of malaria in geographic areas where resistance to Chloroquine is not present.
Treatment of extraintestinal amebiasis.
Chloroquine phosphate tablets do not prevent relapses in patients with vivax or ovale malaria because it is not effective against exoerythrocytic forms of the parasites.
Limitations of Use in Malaria:
Do not use Chloroquine phosphate tablets for the treatment of complicated malaria (high-grade parasitemia and/or complications e.g., cerebral malaria or acute renal failure).
Do not use Chloroquine phosphate tablets for malaria prophylaxis in areas where Chloroquine resistance occurs, Resistance to Chloroquine phosphate tablets is widespread in P. falciparum, and is reported in P.vivax (see WARNINGS).
Concomitant therapy with an 8-aminoquinoline drug is necessary for treatment of the hypnozoite liver stage forms of P.vivax and P.ovale (see DOSAGE AND ADMINISTRATION).
Contraindications
Use of Chloroquine phosphate tablets for indications other than acute malaria is contraindicated in the presence of retinal or visual field changes of any etiology.
Use of Chloroquine phosphate tablets is contraindicated in patients with known hypersensitivity to 4-aminoquinoline compounds.
Warnings
Chloroquine-Resistant Malaria
Chloroquine phosphate tablets are not effective against Chloroquine-or hydroxyChloroquine-resistant strains of Plasmodium species (see CLINICAL PHARMACOLOGY, Microbiology). Chloroquine resistance is widespread in P. falciparum and is reported in P. vivax. Before using Chloroquine for prophylaxis, it should be ascertained whether Chloroquine is appropriate for use in the region to be visited by the traveler. Information regarding the geographic areas where resistance to Chloroquine occurs, is available at the Centers for Disease Control and Prevention (www.cdc.gov\malaria).
Patients infected with a resistant strain of plasmodia as shown by the fact that normally adequate doses have failed to prevent or cure clinical malaria or parasitemia should be treated with another form of antimalarial therapy.
Treatment of Exo-Erythocytic Forms of Malaria
Chloroquine does not treat the hypnozoite liver stage forms of Plasmodium and will therefore not prevent relapses of malaria due to P. vivax or P. ovale. Additional treatment with an anti-malarial agent active against these forms, such as an 8-aminoquinoline, is required for the treatment of infections with P. vivax and P. ovale.
Cardiac Effects
Cases of cardiomyopathy resulting in cardiac failure, in some cases with fatal outcome, have been reported in patients treated during long term therapy at high doses with Chloroquine (see ADVERSE REACTIONS and OVERDOSAGE). Monitor for signs and symptoms of cardiomyopathy and discontinue Chloroquine if cardiomyopathy develops. Chronic toxicity should be considered when conduction disorders (bundle branch block / atrio-ventricular heart block) are diagnosed. If cardiotoxicity is suspected, prompt discontinuation of Chloroquine may prevent life-threatening complications. QT interval prolongation, torsades de pointes, and ventricular arrhythmias have been reported. The risk is greater if Chloroquine is administered at high doses. Fatal cases have been reported. Chloroquine should be used with caution in patients with cardiac disease, a history of ventricular arrhythmias, uncorrected hypokalemia and/or hypomagnesemia, or bradycardia (<50 bpm), and during concomitant administration with QT interval prolonging agents due to potential for QT interval prolongation (see WARNINGS, PRECAUTIONS, Drug Interactions, ADVERSE REACTIONS and OVERDOSAGE)
Hypoglycemia
Chloroquine has been shown to cause severe hypoglycemia including loss of consciousness that could be life-threatening in patients treated with or without antidiabetic medications (see PRECAUTIONS, Drug Interactions). Patients treated with Chloroquine phosphate tablets should be warned about the risk of hypoglycemia and the associated clinical signs and symptoms. Patients presenting with clinical symptoms suggestive of hypoglycemia during treatment with Chloroquine should have their blood glucose level checked and treatment reviewed as necessary.
Retinopathy1
Irreversible retinal damage has been observed in some patients who had received Chloroquine. Significant risk factors for retinal damage include daily doses of Chloroquine phosphate greater than 2.3 mg/kg of actual body weight, durations of use greater than five years, subnormal glomerular filtration, use of some concomitant drug products such as tamoxifen citrate (see PRECAUTIONS), and concurrent macular disease.
A baseline ophthalmological examination should be performed within the first year of starting Chloroquine phosphate tablets. The baseline exam should include: best corrected distance visual acuity (BCVA), an automated threshold visual field (VF) of the central 10 degrees (with retesting if an abnormality is noted), and spectral domain optical coherence tomography (SD-OCT).
For individuals with significant risk factors (daily dose of Chloroquine phosphate greater than 2.3 mg/kg of actual body weight, subnormal glomerular filtration, use of tamoxifen citrate or concurrent macular disease) monitoring should include annual examinations which include BCVA, VF and SDOCT.
For individuals without significant risk factors, annual exams (including BCVA, VF and SD-OCT) can usually be deferred until five years of treatment.
In individuals of Asian descent, retinal toxicity may first be noticed outside the macula. In patients of Asian descent, it is recommended that visual field testing be performed in the central 24 degrees instead of the central 10 degrees.
It is recommended that Chloroquine be discontinued if ocular toxicity is suspected and the patient should be closely observed given that retinal changes (and visual disturbances) may progress even after cessation of therapy.
Central Nervous System Effects
Acute extrapyramidal disorders may occur with Chloroquine (see PRECAUTIONS, ADVERSE REACTIONS and OVERDOSAGE). These adverse reactions usually resolve after treatment discontinuation and/or symptomatic treatment.
Muscular Weakness
All patients on long-term therapy with Chloroquine should be questioned and examined periodically, including testing knee and ankle reflexes, to detect any evidence of muscular weakness. If weakness occurs, discontinue the drug.
Pediatric Accidental Ingestion
A number of fatalities have been reported following the accidental ingestion of Chloroquine, sometimes in relatively small doses (0.75 g or 1 g Chloroquine phosphate in one 3-year-old child). Patients should be strongly warned to keep Chloroquine phosphate tablets out of the reach of children because they are especially sensitive to the 4-aminoquinoline compounds (see OVERDOSAGE and ADVERSE REACTIONS).
Worsening of Psoriasis and Porphyria
Use of Chloroquine phosphate tablets in patients with psoriasis may precipitate a severe attack of psoriasis. When used in patients with porphyria the condition may be exacerbated. Chloroquine phosphate tablets should not be used in these conditions unless the benefit to the patient outweighs the potential risks.
Usage in Pregnancy
Usage of Chloroquine during pregnancy should be avoided except in the prophylaxis or treatment of malaria when the benefit outweighs the potential risk to the fetus. Radioactively tagged Chloroquine administered intravenously to pregnant pigmented CBA mice passed rapidly across the placenta and accumulated selectively in the melanin structures of the fetal eyes. It was retained in the ocular tissues for five months after the drug had been eliminated from the rest of the body2. There are no adequate and well-controlled studies evaluating the safety and efficacy of Chloroquine in pregnant women.
Precautions
Hematological Effects/Laboratory Tests
Complete blood cell counts should be checked periodically if patients are given prolonged therapy (see ADVERSE REACTIONS).
Chloroquine may cause hemolysis in glucose-6 phosphate dehydrogenase (G-6-PD) deficiency. Blood monitoring may be needed as hemolytic anemia may occur, in particular in association with other drugs that cause hemolysis (see ADVERSE REACTIONS).
Auditory Effects
In patients with preexisting auditory damage, Chloroquine should be administered with caution. In case of any defects in hearing, Chloroquine should be immediately discontinued, and the patient closely observed (see ADVERSE REACTIONS).
Use in Patients with Hepatic Impairment
Since Chloroquine phosphate tablets are known to concentrate in the liver, it should be used with caution in patients with hepatic disease or alcoholism or in conjunction with known hepatotoxic drugs.
Central Nervous System Effects
Chloroquine may increase the risk of convulsions in patients with a history of epilepsy.
Drug Interactions
Antacids and kaolin: Antacids and kaolin can reduce absorption of Chloroquine; an interval of at least4 hours between intake of these agents and Chloroquine should be observed.
Cimetidine: Cimetidine can inhibit the metabolism of Chloroquine, increasing its plasma level. Concomitant use of cimetidine should be avoided.
Insulin and other antidiabetic drugs: As Chloroquine may enhance the effects of a hypoglycemic treatment, a decrease in doses of insulin or other antidiabetic drugs may be required.
Arrhythmogenic drugs: There may be an increased risk of inducing ventricular arrhythmias if Chloroquine is used concomitantly with other arrhythmogenic drugs, such as amiodarone or moxifloxacin.
Ampicillin: In a study of healthy volunteers, Chloroquine significantly reduced the bioavailability of ampicillin. An interval of at least two hours between intake of ampicillin and Chloroquine should be observed.
Cyclosporine: After introduction of Chloroquine (oral form), a sudden increase in serum cyclosporine level has been reported. Therefore, close monitoring of serum cyclosporine level is recommended and, if necessary, Chloroquine should be discontinued.
Mefloquine: Co-administration of Chloroquine and mefloquine may increase the risk of convulsions.
The blood concentrations of Chloroquine and desethylChloroquine (the major metabolite of Chloroquine, which also has antimalarial properties) were negatively associated with log antibody titers. Chloroquine taken in the dose recommended for malaria prophylaxis can reduce the antibody response to primary immunization with intradermal human diploid-cell rabies vaccine.
Praziquantel: In a single-dose interaction study, Chloroquine has been reported to reduce the bioavailability of praziquantel.
Tamoxifen: Concomitant use of Chloroquine with drugs known to induce retinal toxicity such as tamoxifen is not recommended (see WARNINGS).
Pregnancy
See WARNINGS, Usage in Pregnancy.
Nursing Mothers
Because of the potential for serious adverse reactions in nursing infants from Chloroquine, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the potential clinical benefit of the drug to the mother.
The excretion of Chloroquine and the major metabolite, desethylChloroquine, in breast milk wasinvestigated in eleven lactating mothers following a single oral dose of Chloroquine (600 mg base). The maximum daily dose of the drug that the infant can receive from breastfeeding was about 0.7% of the maternal start dose of the drug in malaria chemotherapy. Separate chemoprophylaxis for the infant is required (see DOSAGE AND ADMINISTRATION).
Pediatric Use
See WARNINGS and DOSAGE AND ADMINISTRATION.
Geriatric Use
Clinical studies of Chloroquine phosphate tablets did not include sufficient numbers of subjects aged 65and over to determine whether they respond differently from younger subjects. However, this drugis known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug maybe greater in patients with impaired renal function. Because elderly patients are more likely to havedecreased renal function, care should be taken in dose selection and it may be useful to monitorrenal function.
Adverse Reactions
The following adverse reactions have been identified during post-approval use of Chloroquine or other 4-aminoqunoline compounds. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Ocular disorders: Maculopathy and macular degeneration have been reported and may be irreversible. Irreversible retinopathy with retinal pigmentation changes (bull’s eye appearance) and visual field defects (paracentral scotomas) in patients receiving long-term or high-dosage 4-aminoquinoline therapy have been reported (see WARNINGS). Visual disturbances (blurring of vision and difficulty of focusing or accommodation); nyctalopia; scotomatous vision with field defects of paracentral, pericentral ring types, and typically temporal scotomas (e.g., difficulty in reading with words tending to disappear, seeing half an object, misty vision, and fog before the eyes) have been reported. Reversible corneal opacities have also been reported.
Immune system disorders: Urticaria, anaphylactic reaction including angioedema.
Ear and labyrinth disorders: Nerve type deafness; tinnitus, reduced hearing in patients with preexisting auditory damage.
Musculoskeletal and connective tissue-disorders: Sensorimotor disorders, skeletal muscle myopathy or neuromyopathy leading to progressive weakness and atrophy of proximal muscle groups, depression of tendon reflexes and abnormal nerve conduction.
Gastrointestinal disorders: Hepatitis, increased liver enzymes, anorexia, nausea, vomiting, diarrhea, abdominal cramps.
Skin and subcutaneous tissue disorders: Erythema multiforme, Stevens-Johnson syndrome, toxic epidermal necrolysis, exfoliative dermatitis. Pleomorphic skin eruptions, skin and mucosal pigmentary changes; lichen planus-like eruptions, pruritus,; drug rash with eosinophilia and systemic symptoms (DRESS syndrome); photosensitivity and hair loss and bleaching of hair pigment.
Blood and lymphatic system disorders: Pancytopenia, aplastic anemia, reversible agranulocytosis, thrombocytopenia and neutropenia. Hemolytic anemia in G6PD deficient patients (see PRECAUTIONS).
Nervous system disorders: Convulsions, mild and transient headache, polyneuropathy, acute extrapyramidal disorders (such as dystonia, dyskinesia, tongue protrusion, torticollis) (see WARNINGS and OVERDOSAGE).
Neuropsychiatric disorders: Neuropsychiatric changes including psychosis, delirium, anxiety, agitation, insomnia, confusion, hallucinations, personality changes, depression, and suicidal behavior.
Cardiac disorders: Hypotension, electrocardiographic changes (particularly, inversion or depression of the T-wave with widening of the QRS complex), and cardiomyopathy (which may result in cardiac
failure and in some cases a fatal outcome).
Cardiac arrhythmias, conduction disorders such as bundle branch block / atrio-ventricular block, QT interval prolongation, torsade de pointes, ventricular tachycardia and ventricular fibrillation have been reported with therapeutic doses of Chloroquine as well as with overdose. The risk is greater if Chloroquine is administered at high doses. Fatal cases have been reported (see WARNINGS, Cardiac Effects and OVERDOSAGE).
Metabolic and Nutritional disorders: Hypoglycemia (see WARNINGS).
Overdosage
Signs and Symptoms: Chloroquine is very rapidly and completely absorbed after ingestion. Toxic doses of Chloroquine can be fatal. As little as 1 g may be fatal in children. Toxic symptoms can occur within minutes."
"Pediatric Accidental Ingestion
A number of fatalities have been reported following the accidental ingestion of Chloroquine, sometimes in relatively small doses (0.75 g or 1 g Chloroquine phosphate in one 3-year-old child). Patients should be strongly warned to keep Chloroquine phosphate tablets out of the reach of children because they are especially sensitive to the 4-aminoquinoline compounds (see OVERDOSAGE and ADVERSE REACTIONS).
Worsening of Psoriasis and Porphyria
Use of Chloroquine phosphate tablets in patients with psoriasis may precipitate a severe attack of psoriasis. When used in patients with porphyria the condition may be exacerbated. Chloroquine phosphate tablets should not be used in these conditions unless the benefit to the patient outweighs the potential risks."
Here is the link for that info:
https://www.drugs.com/pro/chloroquine.html#s-34088-5
Oops!
I only copied and pasted a small part of that page, but it posted the entire thing.
Sorry.
Makes it impossible to quickly spot the part I was pointing out.
Mods, if you want, please snip all but the past part of that really long label data.
I only meant to post the last two paragraphs starting with “Overdosage”.
I am sorry for not checking….do not know how that happened.
Here is the part I wanted to point out:
Overdosage
Signs and Symptoms: Chloroquine is very rapidly and completely absorbed after ingestion. Toxic doses of Chloroquine can be fatal. As little as 1 g may be fatal in children. Toxic symptoms can occur within minutes.”
“Pediatric Accidental Ingestion
A number of fatalities have been reported following the accidental ingestion of Chloroquine, sometimes in relatively small doses (0.75 g or 1 g Chloroquine phosphate in one 3-year-old child). Patients should be strongly warned to keep Chloroquine phosphate tablets out of the reach of children because they are especially sensitive to the 4-aminoquinoline compounds (see OVERDOSAGE and ADVERSE REACTIONS).
Worsening of Psoriasis and Porphyria
Use of Chloroquine phosphate tablets in patients with psoriasis may precipitate a severe attack of psoriasis. When used in patients with porphyria the condition may be exacerbated. Chloroquine phosphate tablets should not be used in these conditions unless the benefit to the patient outweighs the potential risks.”
The FDA doesn’t like it because it doesn’t put money in pockets of lobbyists.
It really is sad how paranoid so many people have gotten.
There isn’t a shred of evidence that the FDA, or anyone else, is dragging their feet on this issue.
“Trouble is, Laura Ingraham liked to hear herself talk too much, and didn’t give the researcher enough time to explain the results of his study.”
That is a problem for several hosts on Fox. About the time the guest gets to the good stuff, the host jumps in and starts talking over them. It’s extremely irritating and rude on the part of the host. If you are going to a hard break, that’s different, interupt them, but usually that is not the case.
Shut up, Sean! Shut up, Laura! I find myself saying that a lot when listening to their shows.
Steve
“Safe” is a relative term. Almost anything is better than malaria. However, in that context, it does not mean that chloroquine is without side-effects for all users.
The word is preventive.
There is also Quinine Sulfate, often used to relieve leg cramp. It has some mild-ish side effects, possibly worth considering by senior citizens with a bad case of infection with Covid-19, since apparently there is no other effective medication.
More here: https://www.webmd.com/drugs/2/drug-869/quinine-oral/details
“What Conditions does Quinine Sulfate Treat?
– malaria caused by the protozoa Plasmodium falciparum
– falciparum malaria resistant to the drug chloroquine”
I take quinine sulphate tablets to prevent night time cramp in the footss
More published reviewed proof Hydroxychloroquine as a treatment of COVID-19: results of an open-label non-randomized clinical
trial
(1) Yao X, Ye F, Zhang M, Cui C, Huang B, Niu P, et al. In Vitro Antiviral Activity and
Projection of Optimized Dosing Design of Hydroxychloroquine for the Treatment of Severe
Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin Infect Dis. 2020 Mar 9. pii:
ciaa237. doi: 10.1093/cid/ciaa237. [Epub ahead of print]
(2) Colson P, Rolain JM, Raoult D. Chloroquine for the 2019 novel coronavirus SARS-CoV2. Int J Antimicrob Agents. 2020 Feb 15:105923. doi: 10.1016/j.ijantimicag.2020.105923.
[Epub ahead of print]
(3) Wang M, Cao R, Zhang L, Yang X, Liu J, Xu M, et al. Remdesivir and chloroquine effectively inhibit the
recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res 2020;10-0282.
(4) Colson P, Rolain JM, Lagier JC, Brouqui P, Raoult D. Chloroquine and hydroxychloroquine as available
weapons to fight COVID-19. Int J Antimicrob Agents. 2020 [Epub ahead of print]
(5) Gao J, Tian Z, Yang X. Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of
COVID-19 associated pneumonia in clinical studies. Biosci Trends 2020 Feb 19. doi:
10.5582/bst.2020.01047. [Epub ahead of print]
(6) Armstrong N, Richez M, Raoult D, Chabriere E. Simultaneous UHPLC-UV analysis of
hydroxychloroquine, minocycline and doxycycline from serum samples for the therapeutic drug monitoring
of Q fever and Whipple’s disease. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2017: 1060, 166-172.
Because intracytoplasmatic zinc inhibits coronavirus coding of cytoplasmic RNA polymerase, one would think that In older patients, Zinc should be supplemented with the chloroquine which allows zinc to enter the cytoplasm. My two cents worth. Perhaps this treatment should be implemented on older patients with the virus to prevent any further deaths. This is my personal view and I take no responsibility for it so I leave this to the medical professional experts to avoid getting into trouble cheers. In any case in my view the incidence and prevalence of this virus is extremely low compared to any other diseases, viruses such as influenza or normal death rates in older gents and has been completely overblown. The main viral culprit here is social media and politicians which will cost billions and misery worlwide for a nothing burger virus which will in any case stimulate worldwide immunity such as sars ect. Again my personal 2 cents view. We shall see in 2 weeks time LOL.
The UK’s chief scientific adviser said
“If we can get this down to 20,000 and below, that is a good outcome in terms of where we would hope to get to with this outbreak. It is still horrible, it is still an enormous number of deaths and it is an enormous pressure on the health service.”
The average annual flu deaths are about 6-8,000
It is not known if immunity would automatically follow the infection.
Of course it would. That is how viral infections resolve. If antibodies do not develop, the infection becomes overwhelming and the subject dies. The question is whether the immunity is long lasting, and whether viral mutation creates a strain which is not destroyed by the antibodies which exist (see seasonal influenza).
The problem with chloroquine is dose related retinal toxicity. This is highly unlikely in the doses used for malarial prophylaxis, but arises where used in therapeutic doses for rheumatic diseases. Doses below 4 mg per Kg per day are fairly safe. Hydroxychloroquine is safer.
It seem like the Chinese and Koreans are successfully using intravenous Vitamin C which is well known for improving our immune system – maybe we should all increase its use as a preventative. https://truth11.com/2020/03/11/vitamin-c-to-treat-covid-19-coronavirus/
A 50c tablet once a day of Chloroquine or similar is a lot easier is proven effective and gives less profit to big pharma than intravenous vitamin injections, which is probably why they are trying to obfuscate its use against COVID-19.
Do you have any actual evidence that drug companies are trying to discourage anyone from using this treatment?
Coronavirus: it’s time to debunk claims that vitamin C could cure it
http://theconversation.com/coronavirus-its-time-to-debunk-claims-that-vitamin-c-could-cure-it-132803
Didn’t sound like the author debunked anything to me. Vitamin C, among other important functions, helps reduce oxidized glutathione back to it’s active state. Glutathione is the primary anti-oxidant in the lungs, not to mention the entire body, and is up to 1000 times more abundant in the lungs than other parts of the body. Which makes sense because it is the most vulnerable part of the body exposed to oxidizing agents. The body is nothing more than a complex of biochemical reactions, so it just makes basic good sense that it can’t function correctly without requisite nutrients. Enough vitamin C may be obtained from the diet for normal functions, but oxidative stress quickly depletes it. If it’s not replaced in a timely manner, problems will develop.
The author sounds like a shill for big pharma. People who write like that are clueless how they contradict themselves, in this case almost in the same paragraph. The worst harm of vitamin C IVs he can come up with in one paragraph can also occur with what he promotes in the next paragraph.
Maybe he is, and his link to “wellness influencers” doesn’t even concern vitamin C, it concerns vitamin D.
If he had some problem with a study, he should have said what the problem is. It’s somewhat disappointing that much of modern medicine is anecdotal, just like his piece.
Once again, you see what your biases require you to see.
There is nothing contradictory in those two statements. Both statements also happen to be 100% true.
SNIP . Alan, you’re new here so I’ll explain. We do not allow personal attacks on other posters or profanity in comments. Stick to refuting the argument with factual without the personal attack or speculative musings on the motives of the person commenting. Yes, we try but sometimes attacks slip through, it is not the policy here. MOD So many trained medical pill pushers give the line ‘expensive pee’. Well many if not most of today’s medicines are derived from plants and are basically vitamins themselves. Some doctors or wannabe docs arrogantly downplay anything natural that can help because that puts them out of a job and also lowers the sales of the drug companies that sponsor the colleges where they were trained. Here’s some documented evidence of the effect of C versus SARS: https://academic.oup.com/jac/article/52/6/1049/731701
https://www.cell.com/trends/immunology/comments/S1471-4906(03)00286-2
and this article: https://healthcare-in-europe.com/en/news/seeking-a-covid-19-antidote-the-potential-of-ace2.html
that states: ….whilst other reports indicate that Chinese scientists have seen success in delivering high intravenous doses of Vitamin C to seriously infected patients (The journal Caduceus also reports that large shipments of Vitamin C are now enroute to that country).
SNIP