UPDATE: A Covid-19 case correlation between malarial and non-malarial countries has been plotted by Dr. Roy Spencer, and the results are stunning – see below.
Encouraging news: three new medical studies show a commonly available anti-malaria drug known as chloroquine aka chloroquine phosphate is showing strong results against COVID-19 infections in both China and South Korea. Excerpts from three studies, including one published in Nature are below.

An Effective Treatment for Coronavirus (COVID-19)
Presented by: James M. Todaro, MD and Gregory J. Rigano, Esq.
In consultation with Stanford University School of Medicine, UAB School of Medicine and National Academy of Sciences researchers.
Translation by: Celia Martínez-Aceves (Yale B.S. Candidate 2021), Martín Martínez (MIT B.S. 2017)
Summary
Recent guidelines from South Korea and China report that chloroquine is an effective antiviral therapeutic treatment against Coronavirus Disease 2019. Use of chloroquine (tablets) is showing favorable outcomes in humans infected with Coronavirus including faster time to recovery and shorter hospital stay. US CDC research shows that chloroquine also has strong potential as a prophylactic (preventative) measure against coronavirus in the lab, while we wait for a vaccine to be developed. Chloroquine is an inexpensive, globally available drug that has been in widespread human use since 1945 against malaria, autoimmune and various other conditions.
Chloroquine: C18H26ClN3
Background
The U.S. CDC and World Health Organization have not published treatment measures against Coronavirus disease 2019 (“COVID-19”). Medical centers are starting to have issues with traditional protocols. Treatments, and ideally a preventative measure, are needed. South Korea and China have had significantly more exposure and time to analyze diagnostic, treatment and preventative options. The U.S., Europe and the rest of the world can learn from their experience. According to former FDA commissioner, board member of Pfizer and Illumina, Scott Gotlieb MD, the world can learn the most about COVID-19 by paying closest attention to the response of countries that have had significant exposure to COVID-19 before the U.S. and Europe.[1]
As per the U.S. CDC, “Chloroquine (also known as chloroquine phosphate) is an antimalarial medicine… Chloroquine is available in the United States by prescription only… Chloroquine can be prescribed for either prevention or treatment of malaria. Chloroquine can be prescribed to adults and children of all ages. It can also be safely taken by pregnant women and nursing mothers.”[2]
CDC research also shows that “chloroquine can affect virus infection in many ways, and the antiviral effect depends in part on the extent to which the virus utilizes endosomes for entry. Chloroquine has been widely used to treat human diseases, such as malaria, amoebiosis, HIV, and autoimmune diseases, without significant detrimental side effects.”[3]
The treatment guidelines of both South Korea and China against COVID-19 are generally consistent, outlining chloroquine as an effective treatment.
Specifically, according to the Korea Biomedical Review, in February 2020 in South Korea, the COVID-19 Central Clinical Task Force, composed of physicians and experts treating patients agreed upon treatment principles for patients with COVID-19.[4] In China, the General Office of the National Health Commission, General Office of the State Administration of Traditional Chinese Medicine as well as a Multi-Center Collaborative Group of Guangdong Provincial Department of Science and Technology and Guangdong Provincial Health Comp and the China National Center for Biotechnology Development have established effective treatment measures based on human studies.[5]
According to their research (reported in Clinical Trials Arena),
“Data from the drug’s [chloroquine] studies showed ‘certain curative effect’ with ‘fairly good efficacy’ … patients treated with chloroquine demonstrated a better drop in fever, improvement of lung CT images, and required a shorter time to recover compared to parallel groups. The percentage of patients with negative viral nucleic acid tests was also higher with the anti-malarial drug… Chloroquine has so far shown no obvious serious adverse reactions in more than 100 participants in the trials… Chloroquine was selected after several screening rounds of thousands of existing drugs. Chloroquine is undergoing further trials in more than ten hospitals in Beijing, Guangdong province and Hunnan province.”[6]
…
Chloroquine as a prophylactic (preventative) measure against COVID-19[11]
According to research by the US CDC, chloroquine has strong antiviral effects on SARS coronavirus, both prophylactically and therapeutically. SARS coronavirus has significant similarities to COVID-19. Specifically, the CDC research was completed in primate cells using chloroquine’s well known function of elevating endosomal pH. The results show that “We have identified chloroquine as an effective antiviral agent for SARS-CoV in cell culture conditions, as evidenced by its inhibitory effect when the drug was added prior to infection or after the initiation and establishment of infection. The fact that chloroquine exerts an antiviral effect during pre- and post-infection conditions suggest that it is likely to have both prophylactic and therapeutic advantages.”
The study shows that chloroquine is effective in preventing SARS-CoV infection in cell culture if the drug is added to the cells 24 h prior to infection.
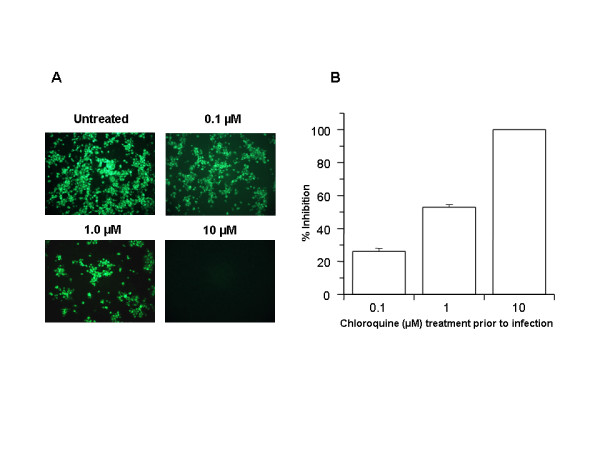
FIGURE 1
Prophylactic effect of chloroquine. Vero E6 cells pre-treated with chloroquine for 20 hrs. Chloroquine-containing media were removed and the cells were washed with phosphate buffered saline before they were infected with SARS-CoV (0.5 multiplicity of infection) for 1 h in the absence of chloroquine. Virus was then removed and the cells were maintained in Opti-MEM (Invitrogen) for 16–18 h in the absence of chloroquine. SARS-CoV antigens were stained with virus-specific HMAF, followed by FITC-conjugated secondary antibodies. (A) The concentration of chloroquine used is indicated on the top of each panel. (B) SARS-CoV antigen-positive cells at three random locations were captured by using a digital camera, the number of antigen-positive cells was determined, and the average inhibition was calculated. Percent inhibition was obtained by considering the untreated control as 0% inhibition. The vertical bars represent the range of SEM.
…
In addition, the study also shows that chloroquine was very effective even when the drug was added 3–5 h after infection, suggesting an antiviral effect even after the establishment of infection.
…
The UK has banned the export of Chloroquine[13]
As of February 26, 2020, the UK government has added chloroquine to the list of medicines that cannot be parallel exported from the UK. Chloroquine was never on this list before. This likely happened because of the growing body of evidence of chloroquine’s effectiveness against coronavirus.
China prioritizes internal use of Active Pharmaceutical Ingredients (APIs) including Chloroquine[14]
In early February, Chongqing Kangle Pharmaceutical was requested by the Ministry of Industry and Information Technology, Consumption Division to promptly increase the manufacturing and production of the active pharmaceutical ingredients chloroquine phosphate despite slowed production during the Chinese New Year.
…
Conclusion
Chloroquine can both both prevent and treat malaria. Chloroquine can prevent and treat coronavirus in primate cells (Figure 1 and Figure 2). According to South Korean and China human treatment guidelines, chloroquine is effective in treating COVID-19. Given chloroquine’s human safety profile and existence, it can be implemented today in the U.S., Europe and the rest of the world. Medical doctors may be reluctant to prescribe chloroquine to treat COVID-19 since it is not FDA approved for this use. The United States of America and other countries should immediately authorize and indemnify medical doctors for prescribing chloroquine to treat COVID-19. We must explore whether chloroquine can safely serve as a preventative measure prior to infection of COVID-19 to stop further spread of this highly contagious virus.
Full study available here
Then there’s this second study:
Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studiesJianjun Gao, Zhenxue Tian, Xu Yang
Abstract
The coronavirus disease 2019 (COVID-19) virus is spreading rapidly, and scientists are endeavoring to discover drugs for its efficacious treatment in China. Chloroquine phosphate, an old drug for treatment of malaria, is shown to have apparent efficacy and acceptable safety against COVID-19 associated pneumonia in multicenter clinical trials conducted in China. The drug is recommended to be included in the next version of the Guidelines for the Prevention, Diagnosis, and Treatment of Pneumonia Caused by COVID-19 issued by the National Health Commission of the People’s Republic of China for treatment of COVID-19 infection in larger populations in the future.
https://www.jstage.jst.go.jp/article/bst/14/1/14_2020.01047/_article
Finally, there’s a new study in the prestigious journal Nature:
Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro
Excerpt:
Chloroquine, a widely-used anti-malarial and autoimmune disease drug, has recently been reported as a potential broad-spectrum antiviral drug.8,9 Chloroquine is known to block virus infection by increasing endosomal pH required for virus/cell fusion, as well as interfering with the glycosylation of cellular receptors of SARS-CoV.10 Our time-of-addition assay demonstrated that chloroquine functioned at both entry, and at post-entry stages of the 2019-nCoV infection in Vero E6 cells (Fig. 1c, d). Besides its antiviral activity, chloroquine has an immune-modulating activity, which may synergistically enhance its antiviral effect in vivo. Chloroquine is widely distributed in the whole body, including lung, after oral administration. The EC90 value of chloroquine against the 2019-nCoV in Vero E6 cells was 6.90 μM, which can be clinically achievable as demonstrated in the plasma of rheumatoid arthritis patients who received 500 mg administration.11 Chloroquine is a cheap and a safe drug that has been used for more than 70 years and, therefore, it is potentially clinically applicable against the 2019-nCoV.
Our findings reveal that remdesivir and chloroquine are highly effective in the control of 2019-nCoV infection in vitro. Since these compounds have been used in human patients with a safety track record and shown to be effective against various ailments, we suggest that they should be assessed in human patients suffering from the novel coronavirus disease.
A commonly available over-the-counter quinine source exists in Margosa Tree Bark and Cinchona succirubra, Peruvian Bark


Tablets of bark extract are widely available in tablet form, from many sources, including Amazon.com here.
There’s also quinine in Tonic Water, which is available just about anywhere at any grocery or liquor store and also at Amazon:
Tonic water is a soft drink containing quinine, which gives it a bitter taste. Quinine is a common treatment for malaria. Quinine comes from the bark of the cinchona tree.
UPDATE:
From Facebook, Dr. Roy Spencer adds this new information.- Anthony
On the subject of using antimalarial drugs for COVID-19 treatment, I’ve compared COVID-19 cases versus malaria incidence by country….
This is amazing. I downloaded all of the data for 234 countries, incidence of total COVID-19 cases (as of 3/17/2020) versus the incidence of malaria in those countries (various sources, kinda messy matching everything up in Excel).
RESULTS, Multi-country average malaria cases per thousand, COVID-19 cases per million, in three classes of countries based on malaria incidence:
- Top 40 Malaria countries: 212 malaria = 0.2 COVID-19;
- Next 40 Malaria countries: 7.3 malaria = 10.1 COVID-19
- Remaining (81-234) countries: 0.00 malaria = 68.7 COVID-19
Again, the units are Malaria cases per thousand “population at risk”, and COVID-19 cases per million total population.
In all my years of data analysis I have never seen such a stark and strong relationship: Countries with malaria basically have no COVID-19 cases (at least not yet).
Additional support for antimalarial drugs for COVID-19 treatment comes from this investigation linked below.
The map says it all: COVID-19 is where Malaria is not.

Quinine, the drug for malaria and also apparently efficacious against coronavirus, is in Tonic water. Fortunately not many know this Sinai was able to get some in the shop today.
Other good advice.
https://www.facebook.com/521723652/videos/10158289063493653/
There is also anti-malaria Quinine sulphate, tell your doctor you got bad leg calf cramps at night. in USA its known as Qualaquin.
FDA warning: This drug can cause very bad and sometimes life-threatening blood problems. Long-lasting kidney problems have happened in some people who get certain blood problems. This drug is not approved for nighttime leg cramps. If you have questions, talk with the doctor.
A much better way is to keep a jar of pickle relish handy. My local storekeeper told me that last year when I was complaining about leg cramps. She explained that her son’s football team kept a jar of mustard and pickle relish on hand to alleviate leg cramps. I have been using the pickle relish ever since as needed.
I have also concluded that a main reason for my getting the cramps is when I drink coffee to late into the evening. When I cut back to only morning coffee then the cramps stay away. However, I can hobble out of bed to get a teaspoon of relish, and minutes later when I am back in bed the cramps stay gone. The vinegar is the main ingredient I believe.
Quinine sulphate was the “magic bullet” which cured my mother’s leg cramps, when nothing else would. But it wasn’t until she found an elderly doctor to prescribe it that she discovered that fact. Most young doctors will not prescribe it for leg cramps, because the FDA warns against it. If you google-search for why that is the case you’ll find this:
That’s apparently based on papers like this one:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4347765/
That paper says that quinine is only “modestly effective” for leg cramps. That might be true “on average,” but I know for a fact that in one particular case it was very effective.
That said, because of the risk of side effects, it should be a last resort.
Great Hope!
I searched for CDC Coronavirus Chloroquine, and it pulled up a website with clinical guidance. The weird thing is that Chloroquine is only mentioned in a footnote at the bottom, and in the text that cites the footnote, it only talks about Remdesivir. Apparently the same paper that found both Remdesivir and chloroquine to be effective against Coronavirus was good enough evidence to mention Remdesivir to clinicians but not good enough evidence to mention chloroquine???
The only reason chloroquine appears on the page is because it was in the TITLE of the scientific article.
Really bizarre if you ask me.
Chloroquine is an approved drug and so has readily available supplies and the safety profile is well characterized.
It is not safe for everyone, and the dosage window is tight (the amount that kills is not much more, far less than an order of magnitude, than the dose that cures), but for those in whom it is not contraindicated it can be given.
Remdesivir is showing great promise and has passed several clinical safety trials in previous outbreaks of another illness, it is a broad spectrum antiviral, and has powerful activity against many viruses in humans, in vitro, and in animal studies.
But it has not been approved by the FDA or in any country…yet.
It is being widely used on a compassionate usage basis, and in many clinical trials.
Because of limited supply, it is being reserved for the most critically ill patients.
Those in organ failure, and those with severe pneumonia.
IOW…the ones about to die.
It has been shown to be highly effective in anecdotal reports in compassionate use.
It is currently illegal to report results of clinical trials of remdesivir, and also unethical.
If it is working on 100% of the most severely ill patients, they are not allowed to say.
This was even mentioned specifically in the press conference today.
So you have to read between the lines.
Makes sense…
Recommendations from South Korea, where they had very low death rates.
I would assume if this works, this is also the reason for the Chinese super low numbers.
They could if they wanted to treat at entire small region of the country with the drug.,
http://joannenova.com.au/Treatment Guidelines from South Korea[7]
If patients are young, healthy, and have mild symptoms without underlying conditions, doctors can observe them without antiviral treatment;
If more than 10 days have passed since the onset of the illness and the symptoms are mild, physicians do not have to start an antiviral medication;
However, if patients are old or have underlying conditions with serious symptoms, physicians should consider an antiviral treatment. If they decide to use the antiviral therapy, they should start the administration as soon as possible: … chloroquine 500mg orally per day.
As chloroquine is not available in Korea, doctors could consider hydroxychloroquine 400mg orally per day (Hydroxychloroquine is an analog of chloroquine used against malaria, autoimmune disorders, etc. It is widely available as well).
The treatment is suitable for 7 – 10 days, which can be shortened or extended depending on clinical progress. Notably, the guidelines mention other antivirals as further lines of defense, including anti-HIV drugs.
Can’t tell you how angry I am, especially after reading
James Delingpole’s article in Breitbart about this today!
Really, the CDC knew about Chloroquine back in 2005!!!
He was spot on!!!
Maybe try reading about virology from people with the training to know what they are talking about.
What you just said is identical, IDENTICAL, to warmistas who say “Exxon knew about global warming back in the 1970s!”
And your anger has as much basis in fact as that of Greta.
Right. Medical problem sorted!
Now, what do we do about saving face for the establishment bureaucrats, who were just about to get their hand on untold trillions and unprecedented power over their populations…?
“Now, what do we do about saving face for the establishment bureaucrats, who were just about to get their hand on untold trillions and unprecedented power over their populations…?”
Answer: We re-elect Donald Trump. I trust him to rein things in towards freedom and prosperity and the well being of the USA and leader of the free world by example.
If you know anyone who has a 3D or more printers let them know that they are in demand now.
Perry Russom NBC10 Boston
·
2h
Just got off phone with Dr. Peter Slavin, president of Mass General. He is looking for anyone with a 3D printer to help make masks. He says there is a formula online. “I would hope companies across the country…would start making masks later this afternoon.”
@NBC10Boston
https://mobile.twitter.com/PerryNBCBoston/status/1240690362441560066
I am certain all hospitals could use them.
There is one standard in science: Evidence.
Evidence is not what people want to be, or what is expedient, or fits with one’s worldview best, or conforms with one’s hopes, dreams, desires, or fears.
Pointing out that only evidence can discriminate between objective reality and opinions is not a rant, and is not advocacy of the opposite side of any argument…unless that argument is that some things are just too important to stick to science, and some feelings are too compelling to be allayed by mere logic, and some dangers are just too scary to stick to what we KNOW to be true, rather than what we are AFRAID might be true.
There is not one standard for medical science and another for climate science, at least there should not be.
To the extent there is, it is because some people find it expedient to dispose of the careful adherence to the scientific method and what can be objectively demonstrated to be true.
There is science, and there is everything else.
There is evidence, and there are opinions and beliefs.
There is what we know, and what he hope and feel.
In any case, this is hardly the first issue in which we have seen people abandon the mantle of rationality.
Credibility is like integrity and trust and honesty.
Once squandered, to some degree it is gone forever.
[riiiiight, meanwhile the FDA is moving forward with it. – mod
“There is evidence, and there are opinions and beliefs.
There is what we know, and what he hope and feel”
This is the crux of any good debate. Feelings be damned in my opinion. If and only if we can agree on what is fact, then and only then can a cogent discussion follow.
That said, there is plenty of evidence of many things. The problem arises when we decide who can determine whether or not there is evidence. That is where things get murky. Is it the FDA? Are they pure? Are they the only ones capable of truth and non political viewpoints? Appeals to authority are not what they are cracked up to be.
I try not to argue feelings and morality… but rather in what was said, done, what is vs what someone feels must be. This is in contrast to arguing from use of “opinion articles” which lead to harmful strawman arguments based on others’ opinions and distortions. Get rid of the strawmen!
Citing FDA approval is not an appeal to authority.
An appeal to authority would be something like saying that we know something is true because so and so said it and he is a well known researcher.
The results of clinical trials are published openly.
The deliberations of the FDA are somewhat of a black box at times, and some have said they act capriciously at times.
I do not know about all of that.
I do know they cite their evidence, which is published by the people running the trials.
The protocol for trial is rigorously written and followed assiduously.
The FDA does not oversee trials, that is a separate entity called the DSMB.
https://www.nidcr.nih.gov/research/human-subjects-research/interventional-studies/data-and-safety-monitoring-board-guidelines
If you are not familiar with a typical result of how a clinical trial is reported, I can show you as many as you like.
They do not use language like: The patients that got treatment X showed that X had”‘certain curative effect’ with ‘fairly good efficacy’ … patients treated with chloroquine demonstrated a better drop in fever, improvement of lung CT images, and required a shorter time to recover compared to parallel groups.”
It consists of numbers, scores, percentages, descriptions of selection and exclusion criteria, the exact care that each group got, how it was determined that the comparator group was equivalent.
Such a determination might include measurements of viral load, or various criteria used to assess patients in a critical care setting.
The results are quantified and precisely described.
The number of subjects in each cohort is given, as well as how many might have dropped out, how many in each group died, how long each group of patients were on oxygen, respirators, total time until discharge, follow up assessments of each patient, all cause mortality, and exactly how the status changed over time at various intervals for each group, as determined by an objective and carefully enunciated set of parameters.
The very act of triaging patients to give the worst off one treatment and those who were not that bad another, means that the results of these two groups are not comparable.
If people who were the sickest were separated out at the admitting room door, and the results of the people who were not as bad off and thus got chloroquine were compared to published rates of survival of patients from some other set of data, like we see reported in some of this work, it is meaningless.
Even having the people giving the care deciding and even knowing who got what and then those same people are evaluating the progress of the patients subjectively, invalidates the results.
They are no longer objectively determined.
Anyone who wants can ask and I will give the historical reference cases for why the double blind standard is universally acknowledged as the only way to have a chance of an unbiased result.
Hi Nicholas: I thought your post was very prescient. However, I was tossing out questions that undoubtedly will get asked…, more rhetorical than anything. I did not mean to give the impression that I was taking an emotional stance against the FDA. They are fallible, but their mission is for a very good cause.
I think mostly, my meandering point was that most people do not argue based on concrete facts, instead they hear something they believe is true and argue as if it were true.
By the way, your patience with us is pretty commendable. Thank you!
Here is how a comparative open label study is written up.
Percentages, confidence intervals, sample sizes, adverse events, lost to follow up, percent who achieved sustained virological response, etc:
https://www.clinicaltrials.gov/ct2/show/results/NCT02607800?recrs=e&rslt=With&cond=Hepatitis+C&map_cntry=US&map_state=US%3AFL&phase=2&draw=2
Thank you Nicholas!
Mod,
I am not sure what you are mocking about what I said, but I am pretty sure you have not read everything I have written carefully.
I want you to find one single thing I said and quote it right here, that is at odds with anything the FDA has said.
I wonder if you are aware of the FDA clarification that it gave after the press conference today (which I watched every word of and applaud), in which they more or less had to contradict the President.
The President is a great leader, and I was supporting him here on this site when most people mocked me for it, long before most people gave him much of a chance.
But he is not the most precise speaker when it comes to details of technical matters, or as it happens, regulatory ones.
He said the FDA had approved two drugs.
He named the two we have been discussing here, as most of us knew he would.
He correctly noted that one has already been approved.
I myself made a point of noting that the drug that is the subject of this thread is approved by the FDA and any doctor can write a prescription for it.
I have been saying for some time that Remdesivir is the most promising candidate for saving lives, all else being equal.
But all else is not equal.
Not even close.
It is currently illegal for anyone involved in the regulatory process or the development or testing of remdesivir to give an opinion of efficacy or how the trials are coming. It is a proprietary drug owned by a publicly traded company.
They are not allowed to say much.
They are not allowed to say what they know, nor is the FDA head.
The FDA moves on applications and approvals.
All that the FDA can do for chloroquine is approve it for an additional usage, but until there are clinical trial results, or it is labelled for that usage by some manufacturer, i wonder what they can in fact do?
That is one reason the FDA was forced to clarify the actual case after the press conference.
This is not mentioned in the Fox News reported you linked to.
I work hard to inform readers here.
I have never gotten a single word of encouragement or support from anyone involved with the site.
I do not care about that…I have my own reasons for what I do and the things I say.
But I have defended this site and never said anything scornful or spiteful to anyone involved with the site.
I think you owe me an apology, but I do not expect one.
I expect more of the same.
But I would ask you, if you think I do not know what I am talking about, or if I have said anything which is factually or technically or scientifically incorrect, to please state so right here, and provide a quote.
I will even say please.
Please show me what I said that has earned your scorn.
Nicholas
You said, “I have never gotten a single word of encouragement or support from anyone involved with the site.” That has changed tonight. I support you. You impress me as being one of the few who knows what he is talking about and is giving useful information and advice. I think that we we are observing is a lot of wishful thinking from people who are scared.
Reminds me of the unknown knowns, the known knowns, the unknown unknowns, the known unknowns, etc.
Nicholas,
Well said.
[mod — from the link you provided: “FDA Commissioner Stephen Hahn explained during the press conference it would be allowed under what’s known [as] “compassionate use” — where doctors can request to use the experimental drug and get permission from the FDA to give to patients. Hahn also said he didn’t want to give “false hope” but said he was hopeful about the treatments.”
Anthony,
You saved lives with this post. Maybe a lot of them. Ive been spamming threads with it for days, contacting conservative authors who have closer contact with the pres. I don’t think the president hears this so quickly without your work.
Roy Spencer as well. The correlations were absolutely convincing. Climate bloggers again!!
Such a huge debt of gratitude for you and what you do.
Please tell me why I do not see what he is talking about whatsoever when I look at the maps next to each other.
I see almost complete overlap:
https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/world-map.html
https://i.insider.com/58137ff6b28a6477058b5958
Well done Jeff
+10
Thanks for this very informative post.
In France, Prof. Didier Raoult, infectiologist and professor of microbiology (one of the first having tested the Chloroquine effect on SARS-COV-2 and proposed to use it against this virus) is not a quack as some believe. He is a reknowed infectiologist and he’s member of the scientific council of the French public health.
Most French epidemiologists and physicians know those first promising results of Chloroquine and it has been asked that a very quick “official” scientific test was done to validate those promising results, which will indeed be done a priori at European level.
One of the chiefs of Salpêtrière Hospital in Paris told to LCI journalists today – when asked on this subject – that those official tests are to begin very quickly and that the results could be known in 3 weeks from now. The usual duration of such tests is one year of even more, he said, so for once, the health administration is actually accelerating the movement.
He also clarified that until those tests are performed and the results clearly established, the fact that some physicians have spread such partial and not validated information was not a good idea nore in accordance with the usual scientific process.
He joked : now we will lack toilet paper, pasta AND Chloroquine.
Fingers crossed for very quick and positive results.
I get alerts from teh FDA whenever they have news releases.
Today I got this one in the early afternoon:
“The FDA has been working closely with other government agencies and academic centers that are investigating the use of the drug chloroquine, which is already approved for treating malaria, lupus and rheumatoid arthritis, to determine whether it can be used to treat patients with mild-to-moderate COVID-19 to potentially reduce the duration of symptoms, as well as viral shedding, which can help prevent the spread of disease. Studies are underway to determine the efficacy in using chloroquine to treat COVID-19.
“President Trump’s aggressive response and bold actions to keep Americans safe from COVID-19 bought us precious time to advance therapeutics and other necessary tools,” said HHS Secretary Alex Azar. “Today’s actions show that HHS and the United States are leading the world in these efforts. Disseminating information about promising off-label uses of drugs we already have, investigating their effectiveness, and pursuing other therapeutics will help give American healthcare providers the tools they need to save lives. As we have always seen when America has faced a serious threat, American industry, academic institutions and government are coming together to deliver us what we need to win.”
The FDA wants to assure the American public that the agency continues to work with partners across the U.S. government and regulated industry to expedite the development and availability of critical medical products to prevent and treat this novel virus, including repurposing existing therapies that may help treat patients with COVID-19.
“As is true for most medical situations, the great American innovators in academia and industry have engaged with us about treatment options. We are extremely encouraged by the interest and promise in the development of the COVID-19-related therapies. We understand and recognize the urgency with which we are all seeking prevention and treatment options for COVID-19. FDA staff are working expeditiously on that front” said FDA Commissioner Stephen Hahn, M.D. “We also must ensure these products are effective; otherwise we risk treating patients with a product that might not work when they could have pursued other, more appropriate, treatments. At the same time, we will engage with domestic manufacturers to ramp up production of this product to mitigate any potential supply chain pressures. If clinical data suggests this product may be promising in treating COVID-19, we know there will be increased demand for it. We will take all steps to ensure chloroquine remains available for patients who take it to treat severe and life-threatening illnesses such as lupus.”
While there are no FDA-approved therapeutics or drugs to treat, cure or prevent COVID-19, there are several FDA-approved treatments that may help ease the symptoms from a supportive care perspective.”
This is precisely what I have been saying here, including the part about not waiting to ramp up production.
And this:
“The FDA is working closely with innovators in their work to expedite these efforts, including leveraging scientific information about the virus and trials currently being conducted in other countries such as China, Japan, South Korea and Italy as well as in the U.S.
Quickly after the emergence of this virus, the FDA began working directly with partners and innovators to foster the development of medical countermeasures against COVID-19, and we are continuing to provide regulatory flexibility, advice, guidance, and technical assistance. The FDA continues to work with interested sponsors to help expedite any additional clinical trials for COVID-19 medical countermeasures that may be appropriate. The FDA is able to, and has been, turning around requests very quickly to assist in initiating clinical trials.
For example, last month, the National Institutes of Health (NIH) began a randomized controlled trial for the treatment of COVID-19 patients with the investigational antiviral drug remdesivir. The FDA has been working with the drug sponsor, Gilead Sciences Inc.External Link Disclaimer, to find multiple pathways to both study the drug under the FDA’s investigational new drug requirements, and thus collect helpful data about the efficacy of the drug, as well as provide the drug to patients under emergency use. The FDA is committed to continuing to make use of its expanded access program to allow the emergency use of this product for those patients, when appropriate. To date, the agency has already granted about 250 patients access to this product. The data collected from the expanded access program may contribute to the agency’s understanding of the drug, but controlled clinical trials are needed to determine if it safe and effective for the treatment of COVID-19 infection.
The FDA’s efforts to facilitate the development of these therapies are squarely focused on ensuring these medical countermeasures meet the agency’s world-respected gold standard, relying on data from adequate and well-controlled trials to most efficiently determine if an experimental treatment can safely and effectively benefit patients.
Innovators are looking at products in a variety of areas, including the assessment of antiviral drugs that might treat the specific virus, as well as host targets, such as interleukin-6 (IL-6) receptor inhibitors that may be helpful in reducing lung inflammation and improving lung function in COVID-19 patients, thereby potentially slowing the progression of severe respiratory symptoms. Regeneron Pharmaceuticals Inc.External Link Disclaimer has announced the initiation of a randomized controlled clinical trial of sarilumab, an antibody to the IL-6 receptor, to assess whether the modification of the inflammatory response by this treatment provides benefit to COVID-19 patients.”
Again, I have made similar comments on many threads over the past several weeks.
https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-continues-facilitate-development-treatments?utm_campaign=031920_PR_Coronavirus%20%28COVID-19%29%20Update%3A%20Chloroquine&utm_medium=email&utm_source=Eloqua
ConUSians
If I were you, even if you feel so far away from any danger, I would have a closer look at what currently happens in Italy, instead of playing scientist with your childish chloroquine thoughts.
In Italy, the situation is so dramatic that in hospitals, the personal inbetween lacks even the time to count the deaths.
At night, convoys with the dead accompanied by the Italian army drive out of some cities because their crematoriums can no longer cope with dead people cremation.
If you do not miss out, CONUS will experience something that is about a thousand times what is happening in Italy.
Simply because you Americans have not been able until today to build a public health system: not ‘America first’ is the rule in your country, but rather ‘Me first’.
*
Just look at this page:
https://www.worldometers.info/coronavirus/#countries
and sort them according to new cases of infection.
Why according to new cases, and not according to new deaths?
Simply because the new cases more and more fill the hospitals until they move into trash mode, and the personnel itself gets infected.
You don’t believe me? So what!
Best greetings from Germany which was sleeping a bit too long, but by far not as long as you all will continue to do…
J.-P. D.
Thank you for your kind wishes. Best wishes to you as well.
Look at how low the mortality rate is in Germany. Any thoughts as to why considering the number of cases?
“Simply because you Americans have not been able until today to build a public health system: not ‘America first’ is the rule in your country, but rather ‘Me first’.”
And if this doesn’t happen you will no doubt declare America’s system superior, right?
“Simply because you Americans have not been able until today to build a public health system: not ‘America first’ is the rule in your country, but rather ‘Me first’.”
What motivates you to attack Americans? What did we ever do to you? You sound bitter for some reason.
As for “me first”, it looks like even the “Me!Me!Me!” generation of American beachgoers is getting the message and are observing President Trump’s request to not gather in groups larger than 10 people on the beaches during Spring Break (lots of little groups of ten now). That seems to me like they are acting in an unselfish way.
I heard today that an American company that makes Chloroquine is donating 30,000,000 doses of it to the cause.
That doesn’t sound like a selfish American action to me.
I could go on for days like this, recounting the generosity and selflessness of Americans during this Wuhan virus crisis, or during any other crisis you can think of.
You don’t like Americans. That’s ok. That’s not required.
I love Americans, and for very good reasons, which you apparently cannot see, going by your attitude. That’s sad. I think you are missig something: an appreciation for some of your fellow human beings. Stereotyping a whole nation of 330 million (or so) people is a lazy way of thinking, imo, and is certainly not accurate.
+330,000,000
kudos!
And by the “Me!Me!Me!”generation, I should have said “generations” because our beachgoers were made up of all ages. The Me!Me!Me! generation is made up of people of a certain mental outlook (selfishness), not a specific age.
And we should cut the beachgoers a little bit of slack. Four days ago, the guidance was for people to hold down gatherings to 250 people, and then the next day the number was lowered to 50 people and then the next day it was lowered to 10 people, so there’s a chance some of the people on the beach didn’t get the latest memo. They seem to be conforming now.
The company that donated the chloroquine pills was Bayer (not sure if that is an “American” company, it’s so hard to tell anymore:) and the amount they donated was stated as 30 million doses in one report and 3 million in another, so I don’t know what the exact number is but it was an act of generosity no matter the amount or the origin..
Bindidon
Looks like you are a genius.
But you have not figured out why they are dying in Italy.
There is a reason that it has peaked in China and Korea, but I will let you figure it out.
Quatsch!
Sounds like somebody’s upset the USA is doing well in the face of danger.
Don’t believe you? Nein, no one cares what you think in the first place.
Du kannst mich, besserwisser!
Bindidon
When did Germany ban travelers from China? Trump did so at the end of January.
As to the American health system, you seem unaware that many Canadians (who can afford it) abandon the public health care in their country and come to the US because they don’t want to wait two or three years.
You give the impression that you are not objective about your evaluation of the US. For example, the chart that you provide a link to shows total number of new cases, without accounting for population. However, it seems that I have seen the same lack of objectivity with respect to climate issues.
Bindidon
I have read elsewhere that Germany uses a different method of attributing death. Perhaps you are comparing apples and grapefruit with your assumptions about the quality of public health systems.
This is from one month ago, … https://www.clinicaltrialsarena.com/news/coronavirus-covid-19-choroquine-data/
Mega dittos to Anthony Watts. WUWT has sparked awareness worldwide. I don’t know about millions, but certainly tens of thousands of lives will be saved because WUWT had the courage and perspicacity to report on the science before anyone else.
And the tenacity. For more than a decade WUWT has been the leading science blog/website in existence, despite financial hardship and unrelenting and hugely unwarranted criticism and attacks.
Now when the need is greatest, WUWT has risen to the task. The whole world owes Anthony Watts an enormous debt of gratitude.
God bless you, Rev.
I hope the people who visit this site understand what WUWT has accomplished. I hope you will be very generous with your donations, and encourage others to contribute as well.
And a personal message to Bill Gates, Mark Zuckerberg, Jeff Bezos, Mark Cuban, Sergey Brin, and all you other silicon billionaires:
This is what a global health breakthrough via the Internet looks like. Right here, right now.
Open up your wallets, guys. Make some big donations to Watts Up With That.
Right here, right now. Show your appreciation. Do it anonymously if that floats your boat, but do it today. Make a real difference. You cannot find a better cause to support.
Thank you.
Mike Dubrasich
“If … CONUS will experience … .”
So, J.-P.D., what has not happened in the U.S.A. will happen if we don’t hand over our excellent physician-patient-driven healthcare industry to the government to run.
Resting as it does on 100% speculation and not one piece of evidence, the court in Bindidon v. The United States of America just held for the Defendant.
Re: “Me first.”
Given all the evidence in the daily news of American generosity in the past week and in numerous publications of American generosity over the course of its history (look up such topics as The Marshall Plan and U.S. spending on NATO equipment for starters),
there is a prima facie case for NOT Me First.
Thus, the burden of proof lies with you.
So far, you have produced no evidence at all.
(apologies for being a bit too “legalistic – I am a depressed, very disappointed, lawyer (7 years of college for nothing…) – I cheer myself up for a little while by writing this way)
Finally, being the typical American that I am #(:))
I want to THANK you Germans for giving us Luther … and Bach… and Beethoven … and Einstein … and von Braun (to name only a few – not to mention Christmas trees and the Waltz and German Chocolate Cake 🙂 )
It’s about 6AM in Germany. How about if we start over and begin Spring walking arm in arm, smiling… friends…
Bitte?
Your American Ally for Science Truth,
Janice
(please forgive any typos above – typing this on a phone (grrr, do-not-like-typing-on-a-phone!))
“It’s about 6AM in Germany. How about if we start over and begin Spring walking arm in arm, smiling… friends…”
I agree, Janice! Let’s all be friends.
Good to see you posting again, Janice. 🙂
Hi Tom,
Thank you, so much. You made my day start off (when I read your friendly greeting while I made my breakfast earlier this morning) with a smile. 🙂 Really needed that. I am facing the sad reality that someone dear to me has, apparently, ghosted me. Someone who I never thought would do that… Heavy heart, these days…
**************
“Speech is civilization itself. The word, even the most contradictory word, preserves contact — it is silence which isolates.”
Thomas Mann
**************
I think, if he knew how isolated I already am, he might relent and speak… and… maybe not…
Anyway! Just wanted you to know how much your kind note meant.
I was also pleased to see you reassure Nicholas M. about the hugely frustrating technical difficulties around here. Arrrgh.
You made excellent points above, btw.
Take care.
Your friend and sister American,
Janice
Anthony Watts and all the “mods”.
This will be my last comment on this site.
I do not mind being insulted or mocked, but your passive aggressive methods of preventing me from replying to people until days later when everyone has moved on is more than I can stand.
The two reasons I am bothering to say anything are, firstly, so I will not be tempted to reconsider, since I really have enjoyed commenting here and I thought at least some people liked to hear at least a few things I have said from time to time, and secondly, because I am sure there are numerous individuals whose day I can make a little happier knowing I will not be around to call them out on their BS.
I wonder how many days will go by before this or any of the many comments you have blocked will be posted, if ever?
Nicholas
I don’t think that your comments are being blocked or even delayed anymore than anyone else. It is a recent peculiarity of the blog that comments are slow to be posted. It seems that is because most go into moderation, and the volunteer moderators are probably overwhelmed with the number of comments.
the delay happens to all of us.
Yes, that is what’s happening. You will get an email notification with posts, that may not show up online yet. Moderators are doing the best that they can. Hey, MUCH better than WebEx!!!
It’s the comment software, Nicholas. I’m posting this message at 7:27am, but there is about a 95 percent chance that my post will not appear on WUWT until about 8:04 am.
If one of your posts doesn’t show up, wait until the top of the hour and then refresh your page and it should be there. If it takes more that a couple of hours to show, then there is probably some other reason for the delay like going into moderation.
The Mods are apparently tweaking the comment software possibly as a prelude to installing new comment software so we are seeing some strange behavior at WUWT. One thing that is happening with me is the standard message is appearing at the bottom of the page requesting that I click and allow cookies to be set by the site, but the message comes and goes so fast I don’t have time to click on it. Apparently, it doesn’t affect the operation of the website for me as I just carry on as usual.
In other words, Niclolas, I don’t think anyone is picking on you and I don’t think you should go away over that misconception.
A well-written parting promise, but one I’d appreciate you reneging on.
For years, I’ve only read the articles here, never the discussions, but branched out after Rud Istvan’s initial post on the Wuhan virus. Think there are somewhere around a dozen posters, maybe a few less, that give good value for the time of reading their posts on this subject, and you’ve been consistently near the top.
Take care.
Guess I should read all the way down. Mods, I don’t think he should have got the “riiiiiight” comment from you. Yes, he seems unduly cautious about a long-term mostly safe substance, but he brought alot of good info and insight, too. He was consistently earnest and did not deserve that tone. My 2 cents.
Won’t forget to thank Mr. Watts, don’t know where else we’d get this level of education, including McGinley’s posts.
I don’t think that chloroquinine is used that much any more. the side effects can be nasty and people in malaria countries don’t take anti-malaria medicine on a continuous basis as it will do more damage than the malaria does.
I took it decades ago in a malaria zone. I wouldn’t take it again.
“I don’t think that chloroquinine is used that much any more.”
According to a doctor on tv this morning, there are a *lot* of doctors in the U.S. and around the world who are using this drug on their Wuhan virus patients.
Although the FDA has not opened the door officially to use it , it is being authorized through the “compassionate use” rule and doctors are using it.
In the next couple of weeks we should be seeing a lot of stories about how this drug is working in patients. Fingers crossed!
for malaria, the link is related to countries that have malaria zones. so if that isn’t accurate what else isn’t accurate?
what went wrong
https://www.buzzfeednews.com/article/benking/coronavirus-covid-19-testing-errors-cdc
Told you guys.
Now, what is STILL going wrong?
In Korea our positive rate is .05%
Korea tests like ******. contact trace and test.
WHY? because a majority of the spread comes from people who dont have symptoms. Same in China
todate we have traced 80% of infections. Trace, find contacts, test more people
USA still requires symptoms to test, so your positive rate is something like 15%
here is a hint.
Tests cost less than shutting your economy down
or sheltering in place.
talk later I’m going out to enjoy a nice restaurant
[Language, Mosh. Mod]
This might be good news.
We need more than one piece of good news to defeat Corvid-19.
A method of directly producing antibodies.
No vaccine. A method that directly produces antibodies.
The US military medical research institute has been working with private industry to develop antibodies that could be direct injected into a person to get an response in 20 minutes.
If it worked and could be mass produced, it could remove our fear of getting Corvid-19.
https://www.foxnews.com/media/dr-jacob-glanville-antibody-neutralize-coronavirus
The completed drug is going to go to the USAMRIID [United States Army Medical Research Institute of Infectious Diseases]. So that’s the U.S. military and they’re gonna be testing it for its ability to neutralize the virus.
“At the same time, that drug was going to go to Charles River Laboratories, which is a international contract research group, which is going to test the safety of that drug,” Glanville said. “Both of those pieces of information come together so that we can produce batches, go through some red tape, and then do the first human studies that we’ll do on 200 to 600 people in the summer, probably in July.”
Thanks for that information, William.
Introduced antibodies, both natural and engineered, look like a good avenue of attack against this virus.
Dr Spencer: Could the difference between malaria and non-malaria infections be due to the airborne transmission of covid-19 and mosquito transmission of malaria?
Hannity just used this map on his show. Hope WUWT or Dr. Spencer get use fees.
I think I am going to tell my doctor that the family and I are going to travel for a few months to a malaria based country and see if I can get a prescription for that drug.
I bet there is a scramble on for this drug right now. Happily, it is cheap and easily produced so supply should not be a big problem.
Roy Spencer remarked, “The map says it all: COVID-19 is where Malaria is not.”
Since the people living in the countries where malaria is prevalent often cannot afford to take quinine prophylactically, and long-term use can have serious consequences, I see the maps as suggesting that the actual correlation is with the climate and not with chloroquine. The inferred correlation with chloroquine appears to be spurious.
Roy
Malaria got its name from the Italians — meaning bad (swamp) air. Malaria was once endemic throughout much of the northern hemisphere. It was mosquito eradication programs in the developed countries that eliminated malaria.
To sort out the confounding influences, I think that one should correlate the per capita use of chloroquine for each country with the prevalence of COVID-19, not with the presence or absence of malaria.
@ur momisugly Nicholas McGinley
I have been following your posts right through and agree on almost every point you make. Research the heavy side of viruses and attempts to develop vaccinations or blanket cures. They all say the same thing. Development for a new virus takes months, usually years.
For those who want to delve into deep microbiology of Covid-19 buy the latest Economist magazine. It does cover some subjects very well. Ignore the climate change BS
I will be taking no precautions. My conclusion from extensive research is that unless the virus dies a rapid death we will all be exposed sooner or later. It may as well be sooner. If medical staff are getting infected with all their knowledge and protective gear we are piddling against the wind to think we can stay clear.
I got my seasonal flu vaccination yesterday compliments of the northern hemisphere. They characterise the variety that you up north were exposed to in your current winter. The vaccine is formulated then it is sent down south. We always come second. It is us that will be walloped in about 2 months time. When My sniffle starts it may well be Covid-19 or a stupid little cold. If it is Covid-19 I have a 90% chance of getting through I recon. I am not expecting a cure. I have had worse odds in life. A good life its been too.
Thank you WUWT with continuing this topic. You are my first port of call each morning. It is definitely the most fascinating global situation I have experienced throughout my life. I agree with others. We have overpopulated the planet. We cannot rule nature entirely. Thank the gods
Cheers
M
Michael Carter: There may be other things you can do. Here’s a pretty interesting article about the antimicrobial/antiviral effects of copper:
https://www.vice.com/en_us/article/xgqkyw/copper-destroys-viruses-and-bacteria-why-isnt-it-everywhere?utm_source=pocket-newtab
When Covid-19 causes severe pneumonia in people over 60, only prayer remains.
…and medicine….
I am very sorry but only prayer.
A big thank you to this website; a beacon of common sense and positive thinking.
This article in today’s Guardian explains a great deal about why the Covid 19 numbers out of Italy have spooked Europe but shows the world a clear path out of this entirely avoidable shambles:
https://www.theguardian.com/commentisfree/2020/mar/20/eradicated-coronavirus-mass-testing-covid-19-italy-vo
The Italian numbers have been skewed by mainly testing those with symptoms, whereas most infected, 70% or more, have no symptoms.
Lesson: Everyone should be tested.
Conclusion: The Italian numbers, and all other numbers, almost certainly inflate, by a significant order of magnitude, the risk of Covid 19 to public health.
The way forward:
‘In the UK, authorities could still identify and isolate clusters, and test everyone who has come into contact with those infected.’
‘…. eradicate the virus through extensive testing of both symptomatic individuals and all of their social contacts – including relatives, friends and neighbours. In this way, we catch out the disease before it has the chance to spread – and, most importantly, before the carrier has the chance to unwittingly pass it on to other people.’
So, hopefully, the entire world can join the United States in a big party on 04 July.
Your very good health!
I have read about 2 different ways in which chloroquine May work.
– reduces change of virus entering cell via ACE2
– gets more zinc in the cell which stops replication
Regarding ACE2, I have read the virus may have other ways to enter the cell via other receptors. I’m not sure if this actually happens or is just a theory, or if virus entering cell with other receptors is more efficient for it vs ACE2.
Some articles say parts of virus genome suggests it can enter cell in other ways.
One thing is we don’t want patients taking chloroquine unless they are under doctor supervision and are isolated until virus clears body. Otherwise a patient might stop taking chloroquine when they feel better but still have virus. The reason is we do not want the virus to mutate in the body to a new form that gets around the chloroquine and then the drug becomes ineffective for this new strain and the new strain spreads.
Meant “reduce chance of virus entering”