UPDATE: A Covid-19 case correlation between malarial and non-malarial countries has been plotted by Dr. Roy Spencer, and the results are stunning – see below.
Encouraging news: three new medical studies show a commonly available anti-malaria drug known as chloroquine aka chloroquine phosphate is showing strong results against COVID-19 infections in both China and South Korea. Excerpts from three studies, including one published in Nature are below.

An Effective Treatment for Coronavirus (COVID-19)
Presented by: James M. Todaro, MD and Gregory J. Rigano, Esq.
In consultation with Stanford University School of Medicine, UAB School of Medicine and National Academy of Sciences researchers.
Translation by: Celia Martínez-Aceves (Yale B.S. Candidate 2021), Martín Martínez (MIT B.S. 2017)
Summary
Recent guidelines from South Korea and China report that chloroquine is an effective antiviral therapeutic treatment against Coronavirus Disease 2019. Use of chloroquine (tablets) is showing favorable outcomes in humans infected with Coronavirus including faster time to recovery and shorter hospital stay. US CDC research shows that chloroquine also has strong potential as a prophylactic (preventative) measure against coronavirus in the lab, while we wait for a vaccine to be developed. Chloroquine is an inexpensive, globally available drug that has been in widespread human use since 1945 against malaria, autoimmune and various other conditions.
Chloroquine: C18H26ClN3
Background
The U.S. CDC and World Health Organization have not published treatment measures against Coronavirus disease 2019 (“COVID-19”). Medical centers are starting to have issues with traditional protocols. Treatments, and ideally a preventative measure, are needed. South Korea and China have had significantly more exposure and time to analyze diagnostic, treatment and preventative options. The U.S., Europe and the rest of the world can learn from their experience. According to former FDA commissioner, board member of Pfizer and Illumina, Scott Gotlieb MD, the world can learn the most about COVID-19 by paying closest attention to the response of countries that have had significant exposure to COVID-19 before the U.S. and Europe.[1]
As per the U.S. CDC, “Chloroquine (also known as chloroquine phosphate) is an antimalarial medicine… Chloroquine is available in the United States by prescription only… Chloroquine can be prescribed for either prevention or treatment of malaria. Chloroquine can be prescribed to adults and children of all ages. It can also be safely taken by pregnant women and nursing mothers.”[2]
CDC research also shows that “chloroquine can affect virus infection in many ways, and the antiviral effect depends in part on the extent to which the virus utilizes endosomes for entry. Chloroquine has been widely used to treat human diseases, such as malaria, amoebiosis, HIV, and autoimmune diseases, without significant detrimental side effects.”[3]
The treatment guidelines of both South Korea and China against COVID-19 are generally consistent, outlining chloroquine as an effective treatment.
Specifically, according to the Korea Biomedical Review, in February 2020 in South Korea, the COVID-19 Central Clinical Task Force, composed of physicians and experts treating patients agreed upon treatment principles for patients with COVID-19.[4] In China, the General Office of the National Health Commission, General Office of the State Administration of Traditional Chinese Medicine as well as a Multi-Center Collaborative Group of Guangdong Provincial Department of Science and Technology and Guangdong Provincial Health Comp and the China National Center for Biotechnology Development have established effective treatment measures based on human studies.[5]
According to their research (reported in Clinical Trials Arena),
“Data from the drug’s [chloroquine] studies showed ‘certain curative effect’ with ‘fairly good efficacy’ … patients treated with chloroquine demonstrated a better drop in fever, improvement of lung CT images, and required a shorter time to recover compared to parallel groups. The percentage of patients with negative viral nucleic acid tests was also higher with the anti-malarial drug… Chloroquine has so far shown no obvious serious adverse reactions in more than 100 participants in the trials… Chloroquine was selected after several screening rounds of thousands of existing drugs. Chloroquine is undergoing further trials in more than ten hospitals in Beijing, Guangdong province and Hunnan province.”[6]
…
Chloroquine as a prophylactic (preventative) measure against COVID-19[11]
According to research by the US CDC, chloroquine has strong antiviral effects on SARS coronavirus, both prophylactically and therapeutically. SARS coronavirus has significant similarities to COVID-19. Specifically, the CDC research was completed in primate cells using chloroquine’s well known function of elevating endosomal pH. The results show that “We have identified chloroquine as an effective antiviral agent for SARS-CoV in cell culture conditions, as evidenced by its inhibitory effect when the drug was added prior to infection or after the initiation and establishment of infection. The fact that chloroquine exerts an antiviral effect during pre- and post-infection conditions suggest that it is likely to have both prophylactic and therapeutic advantages.”
The study shows that chloroquine is effective in preventing SARS-CoV infection in cell culture if the drug is added to the cells 24 h prior to infection.
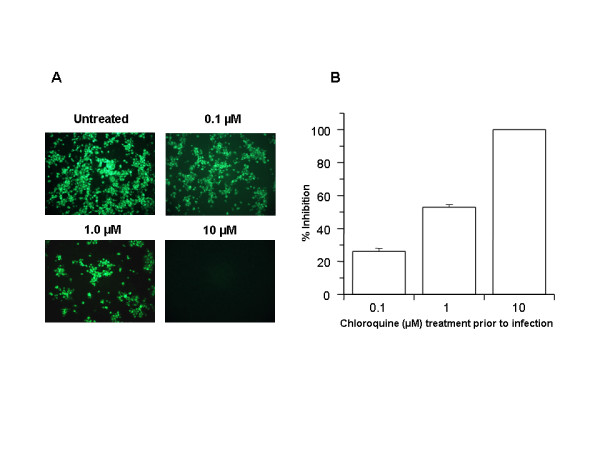
FIGURE 1
Prophylactic effect of chloroquine. Vero E6 cells pre-treated with chloroquine for 20 hrs. Chloroquine-containing media were removed and the cells were washed with phosphate buffered saline before they were infected with SARS-CoV (0.5 multiplicity of infection) for 1 h in the absence of chloroquine. Virus was then removed and the cells were maintained in Opti-MEM (Invitrogen) for 16–18 h in the absence of chloroquine. SARS-CoV antigens were stained with virus-specific HMAF, followed by FITC-conjugated secondary antibodies. (A) The concentration of chloroquine used is indicated on the top of each panel. (B) SARS-CoV antigen-positive cells at three random locations were captured by using a digital camera, the number of antigen-positive cells was determined, and the average inhibition was calculated. Percent inhibition was obtained by considering the untreated control as 0% inhibition. The vertical bars represent the range of SEM.
…
In addition, the study also shows that chloroquine was very effective even when the drug was added 3–5 h after infection, suggesting an antiviral effect even after the establishment of infection.
…
The UK has banned the export of Chloroquine[13]
As of February 26, 2020, the UK government has added chloroquine to the list of medicines that cannot be parallel exported from the UK. Chloroquine was never on this list before. This likely happened because of the growing body of evidence of chloroquine’s effectiveness against coronavirus.
China prioritizes internal use of Active Pharmaceutical Ingredients (APIs) including Chloroquine[14]
In early February, Chongqing Kangle Pharmaceutical was requested by the Ministry of Industry and Information Technology, Consumption Division to promptly increase the manufacturing and production of the active pharmaceutical ingredients chloroquine phosphate despite slowed production during the Chinese New Year.
…
Conclusion
Chloroquine can both both prevent and treat malaria. Chloroquine can prevent and treat coronavirus in primate cells (Figure 1 and Figure 2). According to South Korean and China human treatment guidelines, chloroquine is effective in treating COVID-19. Given chloroquine’s human safety profile and existence, it can be implemented today in the U.S., Europe and the rest of the world. Medical doctors may be reluctant to prescribe chloroquine to treat COVID-19 since it is not FDA approved for this use. The United States of America and other countries should immediately authorize and indemnify medical doctors for prescribing chloroquine to treat COVID-19. We must explore whether chloroquine can safely serve as a preventative measure prior to infection of COVID-19 to stop further spread of this highly contagious virus.
Full study available here
Then there’s this second study:
Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studiesJianjun Gao, Zhenxue Tian, Xu Yang
Abstract
The coronavirus disease 2019 (COVID-19) virus is spreading rapidly, and scientists are endeavoring to discover drugs for its efficacious treatment in China. Chloroquine phosphate, an old drug for treatment of malaria, is shown to have apparent efficacy and acceptable safety against COVID-19 associated pneumonia in multicenter clinical trials conducted in China. The drug is recommended to be included in the next version of the Guidelines for the Prevention, Diagnosis, and Treatment of Pneumonia Caused by COVID-19 issued by the National Health Commission of the People’s Republic of China for treatment of COVID-19 infection in larger populations in the future.
https://www.jstage.jst.go.jp/article/bst/14/1/14_2020.01047/_article
Finally, there’s a new study in the prestigious journal Nature:
Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro
Excerpt:
Chloroquine, a widely-used anti-malarial and autoimmune disease drug, has recently been reported as a potential broad-spectrum antiviral drug.8,9 Chloroquine is known to block virus infection by increasing endosomal pH required for virus/cell fusion, as well as interfering with the glycosylation of cellular receptors of SARS-CoV.10 Our time-of-addition assay demonstrated that chloroquine functioned at both entry, and at post-entry stages of the 2019-nCoV infection in Vero E6 cells (Fig. 1c, d). Besides its antiviral activity, chloroquine has an immune-modulating activity, which may synergistically enhance its antiviral effect in vivo. Chloroquine is widely distributed in the whole body, including lung, after oral administration. The EC90 value of chloroquine against the 2019-nCoV in Vero E6 cells was 6.90 μM, which can be clinically achievable as demonstrated in the plasma of rheumatoid arthritis patients who received 500 mg administration.11 Chloroquine is a cheap and a safe drug that has been used for more than 70 years and, therefore, it is potentially clinically applicable against the 2019-nCoV.
Our findings reveal that remdesivir and chloroquine are highly effective in the control of 2019-nCoV infection in vitro. Since these compounds have been used in human patients with a safety track record and shown to be effective against various ailments, we suggest that they should be assessed in human patients suffering from the novel coronavirus disease.
A commonly available over-the-counter quinine source exists in Margosa Tree Bark and Cinchona succirubra, Peruvian Bark


Tablets of bark extract are widely available in tablet form, from many sources, including Amazon.com here.
There’s also quinine in Tonic Water, which is available just about anywhere at any grocery or liquor store and also at Amazon:
Tonic water is a soft drink containing quinine, which gives it a bitter taste. Quinine is a common treatment for malaria. Quinine comes from the bark of the cinchona tree.
UPDATE:
From Facebook, Dr. Roy Spencer adds this new information.- Anthony
On the subject of using antimalarial drugs for COVID-19 treatment, I’ve compared COVID-19 cases versus malaria incidence by country….
This is amazing. I downloaded all of the data for 234 countries, incidence of total COVID-19 cases (as of 3/17/2020) versus the incidence of malaria in those countries (various sources, kinda messy matching everything up in Excel).
RESULTS, Multi-country average malaria cases per thousand, COVID-19 cases per million, in three classes of countries based on malaria incidence:
- Top 40 Malaria countries: 212 malaria = 0.2 COVID-19;
- Next 40 Malaria countries: 7.3 malaria = 10.1 COVID-19
- Remaining (81-234) countries: 0.00 malaria = 68.7 COVID-19
Again, the units are Malaria cases per thousand “population at risk”, and COVID-19 cases per million total population.
In all my years of data analysis I have never seen such a stark and strong relationship: Countries with malaria basically have no COVID-19 cases (at least not yet).
Additional support for antimalarial drugs for COVID-19 treatment comes from this investigation linked below.
The map says it all: COVID-19 is where Malaria is not.

No one cares anymore even if you show chloroquine and zinc or malaria incidence 100% correlations the powers to be are convinced about coronavirus and global warming and are basically going to cause the death of billions of people due to human stupidity as Einstein said. It happens every 50 years or so. 99% germans thought Hitler was a genious at the time. No one will even look at this stuff. Is it anywhere in mainstream?? It looks like Trump is just another idiot unfortunately who has fallen for this horse s@ur momisugly@@ur momisugly.
Nazis, Einstein, Illuminati Plot to Kill Us All, Billions dead every 50 years, Trump is the AntiChrist…
I think you touched all the bases on that comment!
Bravo!
If true this could be very good news.
Daily Telegraph: A rapid test for coronavirus which could give a result in just 30 minutes for people at home, has been developed by Oxford University.
The super sensitive test, which can picks up the virus in its very early stages when it might otherwise have been missed, could be rolled out to testing centres within a fortnight and could soon be available for home use.
Previous viral RNA tests took 1.5 to 2 hours to give a result slowing down the ability to respond quickly to the crisis.
The technology has been validated with clinical samples at Shenzhen Luohou People’s Hospital in China and has a 100 per cent success rate at picking up both positive and negative results.
Prof Zhanfeng Cui, the Director of the Oxford Suzhou Centre for Advanced Research (OSCAR) said it would initially be used at medical centres but the team hoped people would eventually be allowed to test themselves at home.
No false positives, and no false negatives? Too good to be true .. probably just a press release. By the way, what exactly does it test? Does it tell you “you have a virus now”, or “you had the virus some time ago”, or “you have never encountered the virus”?
Viral RNA tests generally indicate the virus is present on the surface that was swabbed.
Regarding Dr. Roy Spencer’s comment in OP:
I wish he would take that comment to its logical conclusion. What is he saying?
The institues of health in those countries no doubt have records of who is currently on Chloroquine Sulfate or other anti-malarial drugs. Isolate that cohort and distill the percentage who have come down with COVID-19 or other corona viruses.
Actually I wonder if this may have already been done but not acted upon over Big Pharma objections. You guys are burnin’ daylight!
His map is extremely misleading. This link has a far more nuanced map.
From Spencer’s map showing where coronavirus is, you’d think all of Canada and Alaska is affected. That’s just not true. Also, there are small outbreaks in Africa where Spencer shows none.
So, based on my link above, coronavirus tends not to be where malaria is and it also tends not to be in cold places. Once again, General Winter seems to be riding to Russia’s defense.
I commented above Indonesia and Malaysia alone throws his conclusion into chaos. The reason for winter having an effect seems to be social distancing it has been discussed in proper context by authorities.
There is also the claim type A blood groups are more hit based on early numbers out of China but we have no data on what the actual percentages are in the areas of China they just took world averages and it shows type A is over-represented in the deaths.
I think it may have something to do with the fact that countries with malaria are mostly poor countries, and may not have as many people travelling around the world and then going back to there.
Also, they may not have the best data gathering and up to the minute reporting.
And finally, it appears to not be true whatsoever that “COVID-19 is where Malaria is not.”
At least not when I look at maps of Malaria in the world, and FluHan-Wu.
I see almost complete overlap:
https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/world-map.html
https://i.insider.com/58137ff6b28a6477058b5958
Why would the use Chloroquine in areas where Malaria has become resistant to it??
https://www.ncbi.nlm.nih.gov/pubmed/12114045
The population density in Nunavut is 0.02 people per square kilometer.
My grouse is with the map. His numbers, on the other hand, are very plausible. If you take all the countries with no malaria as a group, they have a far higher incidence of coronavirus. Of course Greenland has no malaria and also no coronavirus. And Malaysia has both. IMHO, it’s the aggregate numbers that tell the story.
Malaria is endemic and being eliminated in increasingly large regions. or at least diminished.
This new virus is expanding from a localized point source, and is spreading via travelers and social contacts of a specific nature.
Correlation and causation?
How will these maps change over time?
How did they look two months ago?
Two months from now?
The red blob in europe looks quite dramatic. I wonder what this map would look like with common influenza…
Normal death rates per second and day month year please consider in light of current stupidity https://www.medindia.net/patients/calculators/world-death-clock.asp probably half are viral/bacterial respiratory/cardiac conditions which are NORMAL in older gents. This corona virus is a complete furffy
Normal death rates per second and day month year consider in light of current stupidity https://www.medindia.net/patients/calculators/world-death-clock.asp probably half are viral/bacterial respiratory/cardiac conditions which are NORMAL in older gents. This corona virus is a complete furffy
You mean furphy? Just sayin’
Yes too much gin cheers
Had to look that one up. I don’t suppose you’re from down under?
LOL: No, I read her post and thought the word was odd and Googled it… found the correct spelling. I live in Bay Area, CA.
Vitamin C (ascorbic Acid) has excellent proven effectiveness vs. viruses and in particular flu viruses. There are dozens of peer-reviewed articles demonstrating this. The most effective doses (around 1000 mg/every 4 hours) are a kind “drug effect” by “armoring” the cells against virus penetration. The high doses are necessary to maintain the blood concentration because the body very effectively eliminates it in the urine. The most effective forms that cause little or no stomach upset are the calcium, magnesium and/or zinc ascorbate forms.
Eliminating solid food and doubling or tripling non-sugar liquid intake (and eliminating white sugar) can and should kill the virus in less than 2 days. I have done this many times with the seasonal flu. It is a strong supplement to the immune system.
Here are some articles on the effect of vitamin C:
https://europepmc.org/article/med/25011511
https://iubmb.onlinelibrary.wiley.com/doi/abs/10.1002/biof.5520310101
https://journals.sagepub.com/doi/abs/10.3181/00379727-232-2320847
Good luck to us all in this mindless panic!!
Ian in Vancouver
I should have said that the exponent appears to be decreasing as seen on the log scale, however, large increases in cases have a ways to go, it’s just that cases will not double as quickly.
See Eschenbach’s recent article on the Gompertz Curve. It seems that many of the hot spots are showing a decline in the rate of infection.
Hope someone will take a closer look at the statements of Dr Wodarg on the coronavirus alarmism. Alarmism – for whatever reason – forces people to make irrational and foolish decisions which can only hurt them and those they love.
In answer to a recent question Dr Wodarg said:
I consider the border closures, the cancellation of major events, the closure of schools and kindergartens and the quarantine measures that go beyond the scope practiced in previous years to be medically and epidemiologically unjustifiable. They are not indexed, are based on a falsifying application of an insufficiently validated test and, due to the neglect of important principles of evidence-based disease control, lead to the grossly negligent damage to liberties, property and health.
https://publikumskonferenz.de/blog/2020/03/18/loesung-des-corona-problems-panikmacher-isolieren/?utm_source=Nachrichten-Fabrik.de&utm_content=link
A positive result is being achieved in China with the use of Avigan, a Fuji developed drug.
https://asia.nikkei.com/Spotlight/Coronavirus/China-says-Japan-developed-drug-Avigan-works-against-coronavirus
Study from France:
COVID-19
On 16 March 2020, Professor Raoult announced that a trial involving 24 patients from the south east of France supported the claim that chloroquine was an effective treatment for COVID-19. 600mg of hydroxychloroquine (brand name Plaquenil) was administered to these patients every day for 10 days. While chloroquine has a long safety record, the patients were closely monitored for drug interactions and potential severe side effects. The drug appeared to be responsible for a “rapid and effective speeding up of their healing process, and a sharp decrease in the amount of time they remained contagious”. Professor Raoult said: “We included everyone who was in agreement [to be treated], which was almost everyone. Two towns in the protocol, Nice and Avignon, gave us [infected] patients who had not yet received treatment…We were able to ascertain that patients who had not received Plaquenil (the drug containing hydroxychloroquine) were still contagious after six days, but of those that had received Plaquenil, after six days, only 25% were still contagious.”
https://en.wikipedia.org/wiki/Didier_Raoult
How would you like to be an old person in the control group who received no quinine?
Based on the article and prompted by Dr Roy Spencer update, I went to my friendly Pharmacist here in La Paz, Mexico and was able to Buy for $15 USDs 30 150 mg tablets of Chloroquine over the counter.
I’m not going to take any of them unless I get a doctor permission … but at least I won’t get malaria …
From the article:
“As per the U.S. CDC, “Chloroquine (also known as chloroquine phosphate) is an antimalarial medicine… Chloroquine is available in the United States by prescription only… Chloroquine can be prescribed for either prevention or treatment of malaria. Chloroquine can be prescribed to adults and children of all ages. It can also be safely taken by pregnant women and nursing mothers.”[2]
CDC research also shows that “chloroquine can affect virus infection in many ways, and the antiviral effect depends in part on the extent to which the virus utilizes endosomes for entry. Chloroquine has been widely used to treat human diseases, such as malaria, amoebiosis, HIV, and autoimmune diseases, without significant detrimental side effects.”[3]”
JPP
Lots of side effects from large doses of quinine – look them up – I did yesterday. Did not save the page.
Drinking a tonic water right now. Probably too little to help.
Hopefully, they will work out dosage and optimum time to take to minimize side effects.
This virus problem is a paradigm change until there is a vaccine or very effective treatment.
This virus problem is going to make living in any large city hell. People have no idea what is to come. Add in 20% unemployment.
London is starting to shutdown their underground stations. A large city with no transport and no services is pathetic.
In small cities people can travel by car to get services at limited locations.
Drugs.com lists a lot of side effects from Chloroquine:
From a comment up thread:
https://www.drugs.com/cdi/chloroquine.html
I don’t think I am going to take it even though I have 30 capsules of it…
Thanks to Nicholas McGinley March 18, 2020 at 2:22 pm comment. . .
https://wattsupwiththat.com/2020/03/17/an-effective-treatment-for-coronavirus-covid-19-has-been-found-in-a-common-anti-malarial-drug/#comment-2940930
JPP
Some malaria treatments use 600mg tablets John.
You may find little impact from your 150mg tablets.
Say 80 ppm quinine in Tonic Water in a 330ml (330gm) standard pop can .
Hope I get this right: ~80ppm quinine * ~330g, tonic water = 0.0264 gm quinine = 26.4 mg per 330ml can of Tonic Water.
So a 150 mg quinine tablet would be equivalent to drinking 6 cans of tonic water.
I doubt you will have any side effects from a 150mg tablet – try a weight-adjusted portion on the cat.
Regards, Allan
https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfCFR/CFRSearch.cfm?fr=172.575
Sec. 172.575 Quinine.
Quinine, as the hydrochloride salt or sulfate salt, may be safely used in food in accordance with the following conditions:
Uses Limitations
In carbonated beverages as a flavor Not to exceed 83 parts per million, as quinine. Label shall bear a prominent declaration of the presence of quinine either by the use of the word “quinine” in the name of the article or through a separate declaration.
Reportedly Chloroquine works much better than raw quinine for this virus. But have a G&T anyway!
Has anyone seen anything about this on the news ? CNN, CBS, NBC, ABC, Fox, Etc. Mark levin quoted from the article on his radio show tonight … I don’t know if it was the WUWT article though and he didn’t mention the Update
Gregory Rigano was interviewed on Fox New’s Tucker Carson program tonight
discussing this treatment and new trials.—->
https://www.washingtonexaminer.com/news/malaria-drug-sees-promising-signs-as-future-coronavirus-treatment
I’m of the opinion that this is a manufactured hoax.
Yes, it was on Fox tonight. The study was pretty small, obviously needs to be replicated. Anything that gets me off this couch, as well as a couple billion other people back to work and play, Hurry! There is some money at stake as well, as trillions evaporate from the stock markets worldwide….
COVID19 Treatment by HydroChloroquine & azithromycin
An Effective Treatment for Coronavirus (COVID-19)
Presented by: James M. Todaro, MD (Columbia MD, jtodaro2@gmail.com) and Gregory J. Rigano, Esq. (grigano1@jhu.edu)
https://twitter.com/RiganoESQ/status/1239780304082124800
Gautreta et al. (2020) Hydroxychloroquine and azithromycin as a treatment of COVID‐19: results of an open‐label non‐randomized clinical trial. International Journal of Antimicrobial Agents – In Press 17 March 2020 – DOI : 10.1016/j.ijantimicag.2020.105949
An Open Data Clinical Trial for COVID-19 Prevention
INTERVIEW – GREGORY RIGANO – co-author on study of Chloroquine, Advisor to the Stanford University School of Medicine
Correlation does not prove causation.
Could it be that malaria and the use of these drugs are linked to higher temperatures and it is these higher temperatures that are not virus friendly?
I have seen several references to higher temps killing this virus.
Tim
You remarked, “I have seen several references to higher temps killing this virus.” Indeed, the reason people develop a fever appears to be the body making the host an inhospitable place for the invader. It would stand to reason that ambient temperatures over 106 deg F would be even more hostile to this and other viruses.
According to Science Daily:’ An analysis of public genome sequence data from SARS-CoV-2 and related viruses found no evidence that the virus was made in a laboratory or otherwise engineered ‘.
From the Smithsonian Magazine Nov 2017:
” Is China Ground Zero for a Future Pandemic? “.
https://www.smithsonianmag.com/science-nature/china-ground-zero-future-pandemic-180965213/
It is true though, that before it had ever been encountered in the wild it was first created in a lab!
https://www.nature.com/news/engineered-bat-virus-stirs-debate-over-risky-research-1.18787
And while it may not have been “engineered” as such, the odds that it didn’t come from the Wuhan lab that was experimenting with the virus on live animals are millions to one! The lab has live infected species in cages and the chance of crossover, was intentional!
It is true though, that before it had ever been encountered in the wild it was first created in a lab!
https://www.nature.com/news/engineered-bat-virus-stirs-debate-over-risky-research-1.18787
And while it may not have been “engineered” as such, the odds that it didn’t come from the Wuhan lab that was experimenting with the virus on live animals are millions to one! The lab has live infected species in cages and the chance of crossover, was intentional!
The Telegraph:
On Tuesday evening, the President of Italy’s Liguria region Giovanni Toti said the area had seen ‘the first real case of coronavirus cured’, a 79-year-old man who was treated with remdesivir. He is due to return to his home in Lombardy soon.
Bruce Aylward of the World Health Organization said : “There’s only one drug right now that we think may have real efficacy. And that’s remdesivir.”
apology, ‘bold’ text, left in error
Hi, Vuk
Maybe, but Remdesivir isn’t going to be available to most of those who are at risk, and certainly won’t be suitable for prophylaxis. I’ve spent a long time reading this whole thread and, although I think Dr Spencer may have gotten rather too excited about the malaria link – which looks much less clear than he states – I would be very happy to take a maintenance dose of chloroquine for a few weeks – if I could get it.
Can’t really understand Nicholas McGinley’s long rants discouraging its use. All that he says about clinical trials is true, of course, but looks to be a complete mismatch to the situation most elderly people will find themselves in. The possible downsides with chloroquine don’t seem to add up to very much at all in the context of what we now face. Nicholas must be some kind of bureaucrat, I guess.
Situation in UK with chloroquine seems confused. Not sure it was even a prescription job, but now seems to have been embargoed by the government. At any rate, seems to have disappeared. Maybe they are keeping for health workers? No information on it at Govt helplines.
I expect to get some Quinine sulphate in a day or two, will read carefully any paperwork attached and anything from authoritative sources on the web and give it a cautious low dose try, increasing intensity gradually if get infected.
“….and anything from authoritative sources on the web…”
Aha! I think I see your problem right there…..
DG no fear, i.e. as in nhs.uk, .gov.uk, etc, my wife works for one of the London’s teaching hospitals.
I’ve been around the web for some time, first worked with Ceefax and then ORACLE at their very start driven by PDP-9 beast bit on Prestel too, all some years before the www came along.
POTUS thinks it’ll fine 🙂
Mothcatcher,
I can assure you I have nothing to do with government or anything related.
And I also did not discourage usage of anything.
You should read more carefully and not read INTO my words.
If I am advising caution or jumping to conclusions, it is from the point of view of keeping an open mind until real data is in hand, and not deciding, like many early commentators had, that chloroquine is a cure and that is that.
Looking at the guidelines gives a perfect example of what I am saying: The worst off patients were given one treatment, and those not as bad off were given something else.
This is exactly the sort of disparity that double blind studies overcomes.
I never said, ever, that anyone should not give or take the stuff.
I did not say a single word that is unwarranted, nor did I ever say…EVER, not to take anything.
I spoke rationally and factually, and expressed the need to be hopeful but cautious and open minded.
I would appreciate if you characterized what I said accurately.
If you think I said what you say I said, quote it right here.
Mothcatcher
I also suggested caution because of a personal bad experience with quinine. However, if I should get COVID-19, and my condition was critical, I would agree to a regimen of quinine, under immediate supervision and monitoring by the physician, whom I would advise about my low tolerance for the drug. I think that all that Nicholas and I are saying is that it is probably premature to assume that we have a solution to the problem at hand and that there are no issues with its widespread use. If you saw President Trump’s ‘presser’ today you would have noted that the head of the FDA has reservations and insists that permission be granted for its off-label use, and that its use follow a protocol that will add to the body of medical knowledge. Quinine, despite having been used for 45 years, is not as benign as aspirin. But, then even aspirin has some known issues, such as internal bleeding and Reyes Syndrome.
David Ho one of the country’s to HIV researchers said he doubted HIV anti virals would work, he placed more confidence in remdesivir.
“….I downloaded all of the data for 234 countries, incidence of total COVID-19 cases (as of 3/17/2020) versus the incidence of malaria in those countries (various sources, kinda messy matching everything up in Excel)….”
It has already been stated that data on infection (and even deaths) is going to be sparse and subject to major errors. For deaths alone in Third World countries it is unlikely that precise testing will be undertaken to confirm Covid-19 as opposed to the many other respiratory tract infections extant.
So I expect the error bars for such an exercise to be huge… and correlation does not prove that the cause is anti-malarial medication…
Chloroquine contraindication: Bradycardia <50 BPM. Also elderly.
I just checked to see if I was still alive at 40 BPM and 71 years.
Thanks to Anthony Watts for keeping this posting as top priority. Some mainstream are beginning to divulge this news which may stop this human induced self imolation.
I agree. Our problem is NOT a proven deadly epidemic.
We have a coronavirus epidemic of the kind that happens in higher latitude countries every winter. This infective agent is novel, and there is inadequate information to determine whether the impact (when Covid-19 becomes established) will be extreme, or indistinguishable from regular winter flu.
It is interesting to note that the disabling impact of a flu-like disease in the human body is not due to the viral reproduction, but rather due to the immune system’s response – which may, in the case of a cytokine storm, “destroy the body in order to save it”.
Similarly, Western societies are in danger of causing greater damage by their reaction to this threat – perhaps even destroying themselves. As below, so above…
In the body, various methods of suppressing the immune system when it overreacts are part of the medical armoury. For Society, papers such as the ones WUWT links to above must provide a similar function – that of allaying the panic and bringing decision-makers back down to earth…..
In I think less than a fortnight, WUWT has gone from total denial that there is a problem to jumping on the latest “miracle cure”. What’s worse, is that politicians, like our own in Scotland were doing the same. First totally ignoring it and then only very late realising they ought to have done something like order ventilators for the thousands of patients who will need them.
Because the big problem in this epidemic, as I have been saying for about 6weeks on various media, is the critical shortage of ICU beds and particularly ventilators. The other huge problem is the complacency of politicians who had more than 6 weeks to prepare and didn’t really start doing anything till last week.
MY ADVICE
For most people the risk is relatively low, however, if you get ill during the “peak” and that peak has been allowed to burn like a wildfire, then no matter your supposed health-care plan, you are extremely unlikely to get much medical help if any. So, whether you like your gov or not do head the warnings to self-isolate, etc.
For information, I have set up a new website for the UK: CV19.uk
If it is any consolation, there are no reports from either China or Italy of patients who have been put on a respirator recovering. They just die more slowly, so it doesn’t make a huge difference. The virus causes your immune system to destroy your pneumonocytes, if it kills enough then you cannot recover.
Source?
KREMLIN SAYS RUSSIA “WOULD LIKE TO SEE CRUDE PRICES HIGHER”
By Dina Khrennikova, Ilya Arkhipov and Olga Tanas on 3/18/2020
https://www.worldoil.com//news/2020/3/18/kremlin-says-russia-would-like-to-see-crude-prices-higher
[excerpt]
“We’re very closely monitoring the situation on global oil markets, analyzing the situation, trying to make forecasts for the near- and mid-term future,” Peskov said. “Russia will form its position on any potential new cooperation with OPEC depending on the outcome of the analysis”, he said.
I ran an oil project in the Former Soviet Union that was later sold to the Chinese for US$4.2 billion. Let me translate the above Russian political statement into English:
“Ve are losing our a$$es and ve vill do anyzing to get higher oil prizez!!!”
In short, Russia just blinked. They precipitated this oil price crash by refusing to cooperate with the Saudis, so they knew the exact timing, probably shorted the shares of energy companies in the west, made a fortune, and now want to get their oil revenues back to normal.
This would explain the Diamond Princess Mysteries …. most passengers had malaria med before they got on the ship!
https://wattsupwiththat.com/2020/03/16/diamond-princess-mysteries/#comment-2941339
Read Willis Eschenbach article, and my lady suggested this is the most likely explanation why the infection data skewed on the ship.
You must act immediately. It is better to use preparations that are made from plasma. They can be obtained from people who have recovered. Treatment must be as early, as possible at an early stage.
If treatment is already undertaken in severe cases, we lose control over pneumonia.
Note that flu-type virus epidemics appear to be less prevalent in warm countries – possibly because the virions cannot survive the major infective path of resting on surfaces until another host touches them if the surfaces and the air temperature is hot.
These countries have their own endemic diseases – malaria, for example – which thrive in their climates.
If this is the case, noting that one country has endemic Malaria, but no Covid-19 does NOT indicate that Malaria prophylactics are effective against Covid-19, but simply that Covid-19 (and other similar diseases) just do not spread well in these countries….
It’s interesting that the body temperature of pangolins is in the low 90F range and for bats it is variable, very low during resting and especially low during hibernation but can be well over 100F during flight (core temperature).
Part of our immune response is to use fever against viruses. In any case, there is something to warmth to suppress viruses and it was an especially bad idea to eat bats and to keep pangolins and bats together in a market.
Yes, I’m hopeful that the heat, or more likely, direct sunlight is playing a big part in far fewer cases in the tropics. There may be many cases in southern hemisphere, but perhaps it’s the air con in the more wealthy spots, that’s allowing the bug to flourish. What I can’t figure out, is the lack of clarity here. It can’t be too difficult to carry out a simple experiment. 3 sample surfaces. One in direct sunlight, next in 85 degrees and the other in an airconed room. How long does it take to kill the bug in each case? Seems to me, it would be very useful for us to know that.
Nice comic.
It turns out that a liter of tonic water is probably only a fraction of a therapeutic dose. If one had to drink 6 or 10 liters of tonic water a day they might rather have the virus. The placebo effect is real, however, so maybe a teaspoonful would do.