Guest post by Rud Istvan
Introduction
The Wuhan coronavirus potential pandemic has been much in the news recently. ctm discussed my doing an update to a rather long comment a few weeks ago. I first agreed but then demurred until now.
The reasons for agreeing were the numerous analogies (below) to climate change ‘science’ and ‘prognostications’—albeit on usefully shortened testable time frames like this year, not 2100. Examples below include assuming we know what we actually don’t based on models, and reporting worst case but unlikely scenarios as ‘likely” because ‘if it bleeds, it leads’.
First reason for originally demurring was that the factual situation was too fluid for rational qualitative analysis—alarmist rumors were flying all over, like from ‘reputable’ UK research groups who modeled an R0 near 4 (horrible, as defined below). Pure unsubstantiated alarmism, just like AGW prognostications.
Second reason (ironically), I came down with a wicked, likely coronavirus (less runny nose, more sore throat and cough) cold last week and am still recovering at day nine. So was too sick to even think about a guest post until yesterday evening day 8. Finishing this draft today merely proves that I am finally recovering on day 9 and that it probably was a human common cold corona virus since the typical rhino duration is ‘only’ 5 days, not 9-10.
Qualifications
None, if you are a CAGW ‘believer’. I am not a microbiologist, a virologist, or an infectious disease MD. A CAGW/skeptic ‘critique’ all too familiar at WUWT.
But, I served as CEO for a decade of a small private company that attempted (unsuccessfully for reasons beyond the scope of this post) to commercialize a novel topical antimicrobial PERSISTENT against all bacteria, all fungi, and many viruses including all colds, influenza and pinkeye. I had to teach myself the topic and its medical ramifications in order not to mislead my investors or misuse their several million dollars. Plus, we formed a pre-eminent science advisory board on infectious disease. Plus, in the 2009 swine flu scare, my corporate board forced interactions with NIH (Dr. Fauci), CDC, the FDA, and even the National Security Council (special briefing in the EOB at the WH, 2 hours, spooky)—because our FDA regulatory guy DIED in June 2009 from the swine flu contracted while on a cruise vacation to Mexico with his family (more below).
Those not interested in the background science sections can skip to the last sections of this longish comment, where the intervening basic science is applied to Wuhan coronavirus without further explanation.
Basic Virology
What follows perhaps oversimplifies an unavoidably complex topic, like sea level rise or atmospheric feedbacks to CO2 in climate science.
There are three main types of human infectious microorganisms: bacteria, fungi, and viruses. (I skip important complicating stuff like malaria or giardia.) Most human bacteria are helpful; the best example is the vast gut biome. In human disease some bacteria (typhoid, plague, tetanus, gangrene, sepsis, strep) and certain classes of fungi (candida yeasts) can cause serious disease, as do some human viruses (polio, smallpox, measles, yellow fever, Zika, Ebola).
There are two basic forms of bacteria (Prokaryotes and Archaea, neither having a genetic cell nucleus). Methanogens are exclusively Archaean; most methanotrophs are Prokaryotes. Membrane bound photosynthetic organelle containing cyanobacteria are the evolutionary transition from bacteria to all Eukaryotes (cells having a separate membrane bound genetic nucleus) like phytoplankton, fungi, and us. Both Prokaryote and Eukaryote single cell (and all higher) life forms have a basic thing in common—they can reproduce by themselves in an appropriate environment.
Viruses are none of the above. They are not ‘alive’; they are genetic parasites. They can only reproduce by infecting a living cell that can already reproduce itself. The ‘nonliving’ viral genetic machinery hijacks the reproductive machinery of a living host cell and uses it to replicate virions (individual virus particles) until the host cell ‘bursts’ and the new virions bud out in search of new hosts.
There are two basic virus forms, and two basic genetics.
Form
1. Viruses are either ‘naked’ or ‘enveloped’. A naked virus like cold causing rhino has just two structural components, an inner genetic whatever code (only the two basic types–DNA and RNA–are important for this comment) and an outer protective ‘capsid’ protective viral protein coat. An example is cold producing rhinovirus in the family picornavirus (which also includes polio).
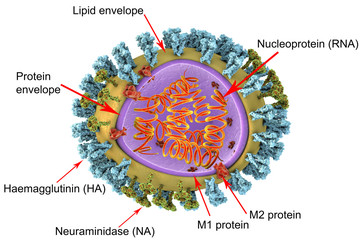
2. Enveloped viruses like influenza and corona (Wuhan) include a third outer lipid membrane layer outside the capsid, studded with partly viral and partly host proteins acquired from the host cell at budding. These are used to infect the next host cell by binding to cell surface proteins. The classic example is influenza (internal genetic machinery A or B) designated HxNy for the flavor of the (H) hemagglutinin and (N) neuraminidase protein variants on the lipid membrane surface.
Conceptual images of both virion forms follow from CDC.
Naked Rhino Enveloped Influenza
![clip_image002[1]](https://i0.wp.com/wattsupwiththat.com/wp-content/uploads/2020/02/clip_image0021.png?resize=215%2C210&quality=75&ssl=1 "clip_image002[1]")
![clip_image004[1]](https://i0.wp.com/wattsupwiththat.com/wp-content/uploads/2020/02/clip_image0041.png?resize=233%2C222&quality=75&ssl=1 "clip_image004[1]")
Genetic Type
The second major distinction is the basic genetics. Viral genetic machinery can be either RNA based or DNA based. There is a huge difference. All living cells (the viral hosts) have evolved DNA copy error machinery, but not RNA copy error machinery. That means RNA based viruses will accumulate enormous ‘transcription’ errors with each budding. As an actual virology estimate, a single rhinovirus infected mucosal cell might produce 100000 HRV virion copies before budding. But say 99% are defective unviable transcription errors. That math still says each mucosal cell infected by a single HRV virion will produce about 10 infective virions despite the severe RNA mutation problem. The practical clinical implication is that when you first ‘catch’ a HRV cold, the onset to clinical symptoms (runny nose) is very fast, usually less than 24 hours.
There is a related epidemiological consequence of great concern. It has been proven possible for a single mucosal cell to be infected ‘simultaneously’ by more than one viral seriotype. That is a simple math probability of virions and host cells Example: you have an easily transmissible ‘normal’ coronavirus cold already (defined below), go to Wuhan and also contract Wuhan. In your body those two different coronaviruses can now both be replicating in the same host cells, and because of RNA replication are indiscriminately exchanging genetic material. So you might end up with an attenuated virulence Wuhan, or a more virulent Wuhan—but most likely both.
The history of the 2009 Swine flu scare showed this. The novel new H1N1 seriotype started in Mexico, where my guy contracted his early fatal infection. For reasons explained below, flu is strongly seasonal. It was winter in South America, so the first hard hit country was Argentina. The mortality data were horrific (5.5%). But, this in hindsight meant the most virulent strains were already burning themselves out, since dead people cannot replicate virions. By the time swine flu reached the North American winter several months later, it was already significantly less virulent (1-2%, still very bad). What actually saved the situation was that based on Argentina, the world appropriately panicked, commandeered global conventional flu vaccine production, and crashed through a swine flu vaccine in just under 6 months at the expense of the normal next year stockpile.
Upper Respiratory Tract viral infections.
So-called URI’s have only two causes in humans: common colds, and influenza. Colds have three distinguishing symptoms–runny nose, sore throat, and cough—all caused not by the virus but by the immune system response to it. Influenza adds two more symptoms: fever and muscular ache. Physicians know this well, almost never test for the actual virus seriotype, and prescribe aspirin for flu but not colds. Much of what follows in this section is based on somewhat limited actual data, since there has been little clinical motivation to do extensive research. A climate analogy would be sea surface temperature and ocean heat content before ARGO. Are there estimates? Yes. Are there good estimates? No.
Common cold URI’s stem from three viral types: RNA rhinovirus (of which there are about 99 seriotypes but nobody knows for sure) causing about 75% of all common colds, RNA coronaviruses, for which (excluding SARS, MERS, and Wuhan) there are only 4 known human seriotypes causing about 20% of common colds, and DNA adenoviruses (about 60 human seriotypes, but including lots of non-cold symptom seriotypes like conjunctivitis (pink eye and pharyngoconjunctivitis) causing about 5% of common colds.
Another climate change related analogy. The internet (including Wikipedia) gets the previous paragraph’s facts mostly wrong. For example, Wiki distinguishes picornviruses from rhinoviruses without realizing the later is a subset of the former, so double counts.
Available data says rhinovirus seriotypes are ubiquitous but individually not terribly infective, coronavirus seriotypes are few but VERY infective, and adenoviruses are neither. This explains, given the previous RNA mutation problem, why China and US are undertaking strict Wuhan quarantine measures.
This also explains why there is no possibility of a common cold vaccine: too many viral targets. You catch a cold, you get temporary (RNA viruses are constantly mutating) immunity to that virus. You next cold is simply a different virus, which is why the average adult has 2-4 colds per year.
This also explains why adenovirus is not very infective. It is a DNA virus, so mutates slowly, so the immune memory is longer lasting. In fact, in 2011 the FDA approved (for military use only) a vaccine against adeno pharyngoconjuntivitis that was a big problem in basic training. (AKA PCF, or PC Fever, highly contagious, very debilitating, and unlike similar high fever strep throat untreatable with antibiotics.) In the first two years of mandatory PCF vaccine use, military PCF disease incidence reduced 100 fold.
These data expanded to influenza also explain why the annual flu shot is so hit or miss. The intent is to match the most common HxNy A or B types from end of this season for vaccination next season. That guess is never perfect. Plus, RNA based influenza mutates rapidly. So even IF the annual flu shot was a good initial match, the flu that spreads by the end of the vaccinated season will be the bits the guess missed—basic Darwinian evolution at work explaining the limited efficacy of the annual flu shot.
A clinical sidebar about URI’s. Both are worse in winter, because people are more indoors in closer infectious proximity. But colds have much less seasonality than flus. Summer colds are common. Summer flus aren’t.
There is a differential route of transmission explanation for this empirical observation. Colds are spread primarily by contact, while flus are spread primarily by inhalation. You have a cold, you politely (as taught) cover your sneeze or cough with a hand, then open a door using its doorknob, depositing your fresh virions on it. The person behind you opens the door, picking up your virions, then touches the mouth or nose (or eyes) before washing hands. That person is now probably infected. This is also why alcohol hand sanitizers have been clinically proven ineffective against colds. They will denature enveloped corona and adeno, but have basically no effect on the by far more prevalent naked rhinos.
There is an important corollary to this contact transmission fact. Infectivity via the contact route of transmission depends on how long a virion remains infective on an inanimate surface. This depends on the virion, the surface (hard doorknob or ‘soft’ cardboard packaging), and the environment (humidity, temperature). The general epidemiological rule of thumb for common colds and flus is at most 4 days viability. This corollary is crucial for Wuhan containment, discussed below.
The main flu infection route is inhalation of infected aspirate. This does not require a cough, merely an infected person breathing in your vicinity. In winter, when you breathe out outside below freezing ‘smoke’ it is just aspirate that ‘freezes’ and becomes visible. Football aficionados see this at Soldier and Lambeau Fields every winter watching Bears and Packers games. The very fine micro-droplet residence time in the air depends on humidity. With higher humidity, they don’t dry out as fast, so remain heavier and sink faster to where they don’t get inhaled, typically minutes. In typical winter indoor low humidity, they dry rapidly and remain circulating in the air for much longer, typically hours. This is also why alcohol hand sanitizers are ineffective against influenza; the main route of flu transmission has nothing to do with hands.
Wuhan Coronavirus
As of this writing, there are a reported 37500 confirmed infections and 811 deaths. Those numbers are about as reliable as GAST in climate change. Many people do not have access to definitive diagnostic kits; China has a habit of reporting an underlying comorbidity (emphysema, COPD, asthma) as cause of death, the now known disease progression means deaths lag diagnoses by 2-3 weeks. A climate analogy is the US surface temperature measurement problems uncovered by the WUWT Surface Stations project.
There are a number of important general facts we DO now know, which together provide directional guidance about whether anyone should be concerned or alarmed. The information is pulled from reasonably reliable sources like WHO, CDC, NIH, and JAMA or NEJM case reports. Plus, we have an inadvertent cruise ship laboratory experiment presently underway in Japan.
The incubation period is about 10-14 days until symptoms (fever, cough) evidence. That is VERY BAD news, because it has been demonstrated beyond question (Germany, Japan, US) that human to human transmission PRECEDES symptoms by about a week. So unlike SARS where all air travelers got a fever screening (mine was to and from a medical conference in Panama City). Since transmission did not precede symptoms, SARS fever screening sufficed; with Wuhan fever screening is futile. That is why all the 14-day quarantines imposed last week; the only way to quarantine Wuhan coronavirus with certainty is to wait for symptoms to appear or not. Quarantine is disruptive and expensive, but very effective.
Once symptoms appear, disease progression is now predictable from sufficient hundreds of case reports—usual corona cold progression for about 7-10 days. But then there is a bifurcation. 75-80% of patients start improving. In 20-25%, they begin a rapid decline into lower respiratory pneumonia. It is a subset of these where the deaths occur with or without ICU intervention. And as whistleblower Dr. Li’s death in Wuhan proves, ICU intervention is no panacea. He was an otherwise healthy 34 years old doctor.
There are two (really now three) key epidemiological numbers: R0 pronounced medically as ‘Rnaught’ (or, as we now know, R0 before and after symptoms). R naught is how many naïves will a single infected individual infect? We know from the Japanese cruise ship Diamond Princess quarantine that R0 is at least ~2. (As of now, 63 diagnosed out of 2667 passengers and ~1100 crew). Since Japan has moved the 63 symptomatic patients to hospital isolation, that same cruise ship may in the next 14 days also provide an experimental symptomless Wuhan R0 estimate. Late revision update, now 69, so asymptomatic R0 is unfortunately above 1.
The second important number is mortality, a virulence metric. We don’t know the mortality rate yet even given 811 deaths/37500 diagnosed. That is because of the multi-week disease progression, even if there were no other data issues. SARS was about 10% in the end (774 deaths from about 8000 diagnosed). The “Spanish flu’ of 1918-19 was also ~10% or perhaps a bit higher (CDC guesstimate is 40-60 million died out of about 500 million infected). BTW, for those wanting to deep dive that last lethal viral pandemic, I highly recommend the NYT best selling book THE GREAT INFLUENZA by John Barry. Wuhan is very unlikely to reach anywhere close to that mortality; otherwise we would already have seen many more deaths.
We also now know from a JAMA report Friday 2/7/2020 analyzing spread of Wuhan coronavirus inside a Wuhan hospital, that 41% of patients were infected within the hospital—meaning the ubiquitous surgical masks DO NOT work as prevention. The shortage of masks is symptomatic of panic, not efficacy.
Scientists last week also traced the source. There are two clues. Wuhan is now known to be 96% genetically similar to an endemic Asian bat corona. Like SARS and ‘Spanish flu’, it jumped to humans via an intermediate mammal species. No bats were sold in the Huanan wet market in Wuhan. But pangolins were, and as of Friday there is a 99% genetic match between pangolin corona and Wuhan human corona. Trade in wild pangolins is illegal, but the meat is considered a delicacy in China and Vietnam and pangolins WERE sold in the Wuhan wet market. This is is similar to SARS in 2003. A bat corona jumped to humans via live civets in another Chinese wet market. Xi’s ‘simple’ permanent SARS/Wuhan coronavirus solution is to ban Chinese wet markets.
This is similar to what is now known about the 1918-19 H1N1 ‘Spanish flu’. It started as a 1917 avian H1N1 (wild duck, Mississippi flyway, fall migration) influenza. It was hosted and incubated in an intermediary species, hogs, in Haskell County, Kansas for the rest of that year. A country doctor tending surprisingly many severe flu cases among hog farmer families as winter 1918 began raised an alarm, but his public health warnings were ignored. Then it jumped from Haskell County, Kansas hog farmers to Camp Funston, Kansas soldiers during winter 1918, where doughboys were training then deploying to Europe to finish the great war. The rest was history, with an R0 guesstimated between 2 and 3.
Conclusions
Should the world be concerned? Perhaps.
Will there be a terrible Wuhan pandemic? Probably not.
Again, the analogy to climate change alarm is striking. Alarm based on lack of underlying scientific knowledge plus unfounded worst case projections.
Proven human to human transmissibility and the likely (since proven) ineffectiveness of surgical masks were real early concerns. But the Wuhan virus will probably not become pandemic, or even endemic.
We know it can be isolated and transmission stopped with 14-day quarantine followed by symptomatic clinical isolation and ICU treatment if needed.
We know from infectivity duration on surfaces that it cannot be spread from China via ship cargo. And cargo ship crews can simply not be given shore leave until their symptomless ocean transit time plus port time passes 14 days.
Eliminating Chinese wet markets and the illegal trade in pangolins prevents another outbreak ever emerging from the wild, unfortunately unlike Ebola.
https://blog.nomorefakenews.com/2020/02/10/china-epidemic-cases-with-no-coronavirus-what/
“China “epidemic” cases with no coronavirus—what??”
2/10/20 Jon Rappoport
I get Jon’s point, but why would the Chinese themselves shut down their own economy based on a health scare they invented? Qui bono?
Go back and read the reports of Hong Kong and other dissent in various parts of China. Some of the unrest was due to the US-China trade conflict. A totalitarian regime, in times of unrest, needs enemies perceived to be bigger than itself and they were in a position to not claim the US was a bigger dog.
If anything this political season around the world has shown it’s all about power. Regardless. The Left, as a Chicagoan famously stated, “Never let a crisis go to waste”… the corollary is “Always find an enemy to blame, even if it’s a bug.”
And who knows? “…an otherwise healthy 34 years old …” who just happens to (horrors!) outs the government is treated and (shockingly) dies? well….
You could think of lots of intricate conspiracies. For instance, China could get the world hooked on its cheap manufacture, then invent a health scare to remove that service while giving plausible deniability that it was intentionally precipitation the West into crisis…
One thing that I have learnt about humans – they form into little groups, each with their own interests, leaders and intentions. Rarely does an organisation or a country ‘come together’ in a conspiracy to drive a single policy through – more often things happen because lots of competing interests inside that grouping temporarily persuade themselves that some course is in their best interests, usually for widely differing reasons…
Skepticism is one thing, but there’s no need to be silly. Rappoport wrong about so much.
This article is incorrect about how the Spanish flu started the Spanish flu stared in China and not in Kansas USA
Read the article again.
It looks like China has had a very cold and snowy winter, not warmer. https://climate.rutgers.edu/snowcover/chart_daily.php?ui_year=2020&ui_day=40&ui_set=2
Going back several months, snow cover across China has been above average. Click on the single arrow to the left of ‘day’ to go back.
Everything bad is eventually blamed on climate change.
And don’t you forget it.
But, there’s no evidence (yet) that coronavirus is caused by climate change, because China is having a snowy winter.
— Unusual cold and snow is “weather”.
— Unusual heat would be “climate change”
Cold weather promotes “cold” viruses.
Just warm them up. Problem solved.
M.Simon, from your own post from Musings…
https://chiefio.wordpress.com/2020/02/06/6-feb-2019-ncov-corona-virus-outbreak/#comment-124672
The virus can survive for 9 days on many surfaces.
Try again
https://www.lincolnshirelive.co.uk/news/uk-world-news/scientists-discover-wuhan-coronavirus-spreading-3830100
Incubation period possibly up to 24 days as indicated today by Chinese officials.
That article was reporting an endpoint signifying most likely a single outlier case, possibly with unreported or unrecalled exposure in a shorter time frame. That same article reported a median incubation period of 3 days, which is the more relevant number for assessing risk and actually shorter than previously thought. Focusing on outlier cases where someone claims not to have exposure for 24 days before getting sick or someone who appears to have spread the virus to a lot more people than expected as if it represents a norm is alarmism. The truth is bad enough and getting hung up on dubious outliers is not a useful exercise.
Reports of overworked crematoriums is just fear mongering.
Reports of 5X the normal cremation rate are not official.
=====
The numbers released by the government do not match government behavior. They are the official truth. Allowed Speak.
Consistent 2.1% deathrate compared to cases. Virus good at math.
That presumes that each victim either dies or recovers the instant that they contract it. I wish people could think
Spot on ; the deathrate,caserate,condition recovered,mild or serious seems to be very consistent with a mathematical formula .
In 1 particular country .
Better to compare the death rate with the recovery rate. At present it is about 25%. Hopefully as they get better at identifying the illness early and treating it more effectively this will improve.
Looking at the out of mainland china deaths compared to confirmed cases two weeks ago show 2 deaths by the 11th of February with 87 cases on 1/28. This is comparable with the 2 – 3% death rate. However when we do the same with the mainland china numbers we get 1016 deaths for 6000 cases on 1/28/2019 which is about 17%. This higher number may be due to:
1) Under reporting of mild cases. They only have enough test sets for some people that need hospitalization so that the 80% who don’t need hospitalization are not being tested.
2) Health care system in china being overloaded to the point where they people die due to lack of equipment and people.
The other problem with China is that the way they do death certificates does not always show the root cause. For example they show in cases of the flu, pneumonia instead of flu has being the cause of death. Which is why official numbers of deaths from flu are far less in China than in the US.
In conclusion China is under reporting the deaths and way under reporting the number of people infected. So the percentage mortality could be anywhere from 1% to 6% and is probably around 2%’ In another month using non china numbers we should have a very good idea what the actual mortality is, as long as your health care system does not get overloaded.
Should add, with a lag the actual death rate is probably way higher. If the lag is two weeks, the rate is close to 30%. At one week lag it is 5.2%. Remember it is Official numbers. From the first 8 including the doctor, we now know at least 3 have died. that is 3/8 or 37.5%, but small group. What we know today is this is airborn, and the rate may be anything between 5 and worst case 37.5. Probably not lower than 5, but that will be found out in Japan.
Many possible calculations for the Corona virus death rate at this page: https://www.worldometers.info/coronavirus/coronavirus-death-rate/
This point came to me some days ago. With everyone geared toward a 14 day quarantine period what happens if it is double that, or if it can lie dormant for 3 months? The amount of possible cross infection does not bear thinking about.
however, as yet , much of this is speculation and with the draconian efforts by the Chinese to contain it lets hope that this is all just a memory in six months time.
let us also hope that the eating of exotic species is knocked on the head.
tonyb
Quarantine period is already extended to 4 weeks.
“Quarantine period is already extended to 4 weeks.”
This is false.
14 days is the quarantine period because it is at the extreme outside of the possible range of latency for an infected person.
If that was in any way typical, then it would be a dumb amount of time for a quarantine.
Forcing those people to stay on that ship may be the worst idea ever, depending on the virus particulars.
They have the same people serving everyone on the ship three meals a day every day for two weeks?
Very poorly thought out, IMO.
Already we are seeing the number of people getting sick on the boat going up by large numbers over a week after they were quarantined.
Some people are know to be showing symptoms in as few as 3 days.
If it is being spread by aerosols, they could be spreading it to each other by dint of them all breathing the same stale air for two weeks.
The immune system does not let viruses or anything else just hang around in our bodies.
14 days would be extraordinarily long for an incubation period.
The virions are getting mopped up by the innate immune system from the instant of infection, and incubation periods represent the amount of time it takes for the virus to multiply enough to overcome the immune system, infect cells, make news copies of itself, etc…prior to enough antigen being present to cause symptoms.
According to the CDC, the 14 day incubation period is being inferred, with that amount of time being thought to have occurred with MERS.
The CDC also states that there is no specific information confirming that the disease can be spread prior to a person showing symptoms, just that in general a person might be infectious from one day prior to seven days after the onset of symptoms with certain similar viruses.
The report from Germany of a patient spreading the disease prior to having symptoms has been retracted. It seems the woman in question had not been questioned carefully…at the time she spread the disease to four other people, she had muscle pain and was taking an anti-fever medication.
The reports from China of symptomless transmission had come from people who did not actually observe this occurring, but had been told by patients that it was the case. It is not confirmed.
Sources:
https://www.news-medical.net/news/20200205/Coronavirus-cane28099t-spread-if-the-patient-doesne28099t-have-symptoms-report-says.aspx
https://www.cdc.gov/coronavirus/2019-ncov/faq.html
There is no evidence that the novel virus spreads by aerosols. It is thought to be spreading by respiratory droplets.
This means you have to be very close to someone to have a high risk of getting infected if, for example, you sat next to or near someone on a plane that had it.
If it was spreading easily over distance of more than 6 feet, and was being spread readily by people prior to symptoms, there has been plenty enough time since the first person in the US, a man who had travelled to Wuhan, came back to the US, was found to be sick at some point shortly after, and was hospitalized.
That person has n gone home as of last week, and the last report I read indicated that the only person he infected was his wife through intimate contact. No one on his plan, no neighbors, etc, have come down sick.
It appears to me that the people who were spreading it were doing so prior to everyone being alerted to a new and serious disease, at which point people became more careful and would have been less likely to interact with others if they came down with symptoms.
As a side note, masks are generally not thought of as protecting a well person from getting a virus.
They are mostly used to keep a sick person from passing something to someone else., although they may be better than nothing if someone sneezes near you or in your face…or not. They may just be collecting up stuff and holding it against your face.
Bad information can arise for any one of several reasons, or a combination of reasons.
But keep in mind, at this point definite facts are sparse and much is uncertain.
Primary sources of info are best, IOW from medical authorities and not newspaper accounts and probably not any web sites that are not responsible medical authorities.
If we indiscriminately believe what we read, it would be easy to be sure that this is a bioweapon, but not to worry because vaccine is already being prepared.
I saw some guy on one website who purported to be a medical guy in China talking about 50,000 bodies being cremated in one city alone, and a video showed a woman climbing out a high rise window, apparently trying to get to the apartment right above hers to get some rice to eat.
She fell and the fall was graphically shown on the video with no warning…complete with loud splattering noise.
But there was no way to know where it was or when, or indeed why she did not have the rice passed down to her, instead of doing a very bad Spiderman impersonation.
Have you wrote for this site. You sound very learned and with good sources. This is a lot to read in a comment though. I appreciate you helping out but I for one do not want to read for hours in the comment section. Thank you for helping. I do appreciate your work.
I appreciate your kind words.
It is a lot of information.
Complex subject matter cannot be distilled to a sound bite.
I should try to have the most important parts at the beginning, like newspapers used to do.
Rud, thanks for a most readable, concise, and fascinating look at the virus and its spread.
From what I’ve read, the masks do little. The best protection advice seems to be:
a) Stay home
b) Wear gloves
c) Wash your hands. A lot. More than you’d think. More than you’d want to.
d) Avoid touching your face.
Would you agree?
Stay well,
w.
Willis, highest regards, and yes to all your points.
Frequent hand washing and NOT touching your face are the two biggest factors in avoiding cold transmission. They are especially important when out and about. Because that is where common cold contact transmission occurs. Most people don’t know this, but clinical observation studies have shown that the average person touches their mouth (lips), nose, or eyes (all enabling transmission) 15-20 times per hour! (There is a whole literature based on age (children, young adults, older adults), sex (turns out women fuss with their faces more), circumstances (office, shopping). That gives those virions picked up by touching stuff like shopping cart handles and door knobs LOTS of shots on goal.
BTW, I am always amused by the alcohol wipes grocery stores provide to wipe down their cart handles, especially in winter. At best effective in 25% of cold cases from enveloped virus. Useless against 75% caused by ~100 different rhinoviruses. Essentially useless against flu unless you can shop without breathing. Always get the annual flu shot, but then hope for the best and expect the worst.
Thank you, Rud!
This helped me considerably.
I am not close to panicking about this or most of the diseases that run about, but my antennae are always up and searching for the next threat.
It’s always great to have actual information.
Having a wipe kill a virus is not the only way they can provide some protective benefit.
There is also physical removal of the virions by wiping them up and having them adhere to the wipey.
One of the reason the people in doctors offices and hospitals do not get sick many times every year is because they are trained to not touch their faces and to wash hands a lot.
You do not have to keep every last virion out of your body.
For every disease, there is a minimum infective dose.
If you keep the number in your body below that, you will not get sick but may become immunized, at least slightly. And getting a high dose at the initial exposure will make the case of the disease you do get have an excellent chance of being far worse than if you get only the minimal infective dose.
Wiping surfaces is not useless…just be aware that they are not sterilizing the surface, and that doing it three times is a lot better than wiping it once. Use a fresh couple for each step.
It is like triple rinsing a container full of some nasty chemical. The water is only diluting it and using mechanical action to wash off the traces stuck to the container, but by the time you have rinsed it three times, the amount left is a tiny fraction of what was there to start with.
( The two things I use at home that most people do not seem to realize the value of, are povidone iodine, and something called Hibiclens. Both are available at CVS or any drugstore.
Both are used by doctors and hospitals to sanitize and sterilize surface and skin prior to or after surgery.
Hibiclens to wash hands, povidone for skin on the person being operated on and also for hands of the medical teams. Make sure you do not get even one speck of it in your eyes.
If you have a cut that takes more than a couple of days to heal…it has an infection…put a drop of povidone on a bandaid and put it on the cut overnight, and for longer if it is not much better over night.
The thing about iodine is…it kills bacteria, fungi, protozoans, and viruses.
It will also make contaminated water safe to drink in a emergency situation, and can be used in case of nuclear wars to stave off the effects of radiation sickness. At about ten bucks for enough to last for decades [unless there is a nuclear war…it will probably run out sooner if that happens and you use it to protect your thyroid] and it is a must have.0
yup I have the 10% stingy version of iodine,
betadines only 3%
and good old teatree oil is also close to as good for all of the above too,
they reckoned our soldiers were given eucy or TT oils in their med kits
and its supposedly why they survived bad wounds where other didnt.
The Betadine in my medicine cabinet is 10%.
My dad was a doctor and of the 5 kids, none of us missed a single day of school due to illness.
I always thought that this was because dad brought home micro-doses of whatever was going around on his clothes every day.
The concept if a minimum infective dose was a real eye opener for me personally.
Among other things, it got me to wondering what happens if the dose of an infectious organism is below this limit?
Should also be noted that many sanitary wipes have more than alcohol on them.
A commonly used variety has alcohol and also 4% chlorhexidine gluconate…the stuff in Hibiclens.
Also note that alcohol will not do much, in fact nothing will, unless your hands are clean of dirt and grease, oil, etc.
And alcohol is listed as being slow acting against non enveloped viruses…not completely useless.
Wipes typically contain a surfactant and some water to dilute the alcohol to reduce evaporation time and increase contact time with pathogens.
Viruses do not tend to live long on surfaces, as you noted, so it stands to reason that anything that creates a more hostile environment for them is better than nothing.
Many cases of the flu are thought to be from touching a surface that has been sneezed on…and alcohol kills the flu virus very effectively.
I for one would not discourage anyone from using whatever types of cleaning products are handy.
Whatever they do, it is better than nothing.
Plus, as noted…they can wipe away lots of pathogens without killing them…just by having them adhere to the wipey.
“There a few ways that alcohol can kill bacteria and viruses, the most important one is that they will denature proteins. Other modes of action include having a direct effect on the RNA of the organism, killing the cell through breaking its plasma membrane, cell lysis and interfering with the metabolism of the cell.”
“All of the types of alcohol will kill most bacteria, including mycobacteria, but is really only effective in concentrations >60%. As stated previously, alcohols will not eliminate spores, which means it is not a good choice when considering disinfection of surfaces contaminated with Clostridium Difficile – a spore forming organism. However, Boyce reports that combining ethyl alcohol with alkali, mineral acids, hydrogen peroxide, or some surfactants can enhance its activity against spores. Alcohol also kills fungi and many viruses.
It has particularly good activity against viruses such as herpes, HIV, Influenza, Hepatitis B&C, but poor activity against Hepatitis A and polio. Ethyl alcohol is more virucidal than isopropyl alcohol when it comes to non-enveloped viruses such as Adenovirus, Rhinovirus, Enterovirus and Rotaviruses, but the activity is slow.
Alcohol has also been shown to be effective in disinfecting surfaces contaminated with pandemic viruses such as Ebola and SARS Coronavirus and has some activity against Norovirus.”
https://reynardhealth.com/using-alcohol-to-disinfect-healthcare-surfaces/
After I switched from dental floss to proxa brushes (and stopped putting fingers in mouth every day) my common cold incidence dropped from 1 or 2 per year to 1 every two or three years, for the past 20 years.
Masks are pretty effective at collecting sneeze goobers originating from the mask wearer which is actually why doctors want patients to wear them. And less hand-touch contamination for those who sneeze into their hand. If you are healthy and not sneezing, they do very little, quite unlike wearing one while leaf-blowing.
They prevent you from touching your mouth and nose, and goggles prevent you from touching your eyes (another route for infection). As such they are useful.
The principal reason for wearing the mask is/was supposed to be to prevent spreading your particles to others. That is why they are designed the way they are.
Sneeze and cough into your elbow. Make it a habit.
In view of the article cited and that of the “two versions” of the day before, this advice doesn’t appear to make sense:
a) “stay home” – easy to say, but only works if:
1) you live alone
2) have enough food, medicine, etc., to last out the epidemic
b) “wear gloves” – also easy to say, but:
3) will not prevent you from infecting yourself
4) will make access to your bare hands much more awkward
5) will create many more opportunities to infect yourself while taking them off
c)” wash your hands”:
6) presumably to wash off the virus you got on them from taking off your gloves?
d) “avoid touching your face”
7) why, will the virus crawl up your nose? Presumably, so long as you avoid poking your finger up your nose or into your mouth, the respiratory route of infection is not involved.
I propose a more sensible check list, based on the two articles and their logical interpretation:
1. wear a mask when there’s a possibility of close proximity to other faces
2. wear glasses, sunglasses or protective glasses under the above conditions, to prevent occular transmission
3. when taking off the mask and glasses, have soap and water or alcohol sanitizer and a hair dryer at hand.
4. wash hands thoroughly first.
5. take off the mask and blast it from the inside with the dryer, then again from the outside. This should take care of any viruses on the surface.
6. take off glasses and wash them and the hands thoroughly
7. wash face
8. if wearing gloves, wash them thoroughly at step 4, instead of washing hands, and again at step 6, while washing glasses, then remove them to wash hands and face.
PS. I mention glasses although I don’t understand how occular trasmission ranks in terms of severity of infection. Would welcome clarification
Just learn how to take off gloves. It is taught in hospitals and NBC military training with touching fingers. I’m sure it’s on YouTube somewhere
If taking off contaminated gloves is too difficult to describe succinctly here, I’m pretty sure most people won’t be capable of remembering to do it right.
And are you also going to carry a hazmat bag everywhere you go, as well as extra gloves?
The origin of the “Spanish Flu” remains controversial.
It may have appeared in France in 1916 or elsewhere earlier. Birds and pigs were kept behind the lines on the Western Front to feed the troops. Chinese and other East Asian laborers were also brought into to relieve British and French manpower crunch.
The flu also might have shown up in pigs earlier because they are more susceptible.
Its mortality rate was inflated by wartime conditions.
Some recent surprising leads could help clarify the picture.
https://www.statnews.com/2018/12/05/1918-spanish-flu-unraveling-mystery/
Anyone remember the riots and protests in Hong Kong?
Of course, nothing beats a national medical emergency from a highly infectious disease to stem the tide and discourage mass gatherings.
Bats; laboratory release….Mmmm!
True, but also calls into question the omnipotence and omnicompetence of the Party and its Mandate of Heaven.
Wait. Masks are outlawed? Masks are Not outlawed? Masks are de rigueur? Ah, masks mandated!
Any ideas on the origin of the Spanish Fly?
Yeah, right here:
https://youtu.be/AHfhK6fEFf0
Oh, my bad…I was thinking of Super Fly.
Messed that up and grabbed Shaft by mistake.
I have no expertise of any kind in any of related fields, however having an idea what Chinese dietary practices from animals of all kinds, I am surprised that this has not happened many years ago and times before.
Wikipedia states: “Wuhan consists of three national development zones, four scientific and technological development parks, over 350 research institutes, 1,656 hi-tech enterprises, numerous enterprise incubators, … Its major industries include optic-electronic, automobile manufacturing, iron and steel manufacturing, new pharmaceutical sector, biology engineering, new materials industry and environmental protection …..
The pharmaceutical sector and biology engineering obviously would be doing all kind of research; considering the rapid spread of the virus, it strikes me odd that if locals have been eating or using bats or snakes for traditional Chinese medicine for years, that this kind of epidemic has not occurred before, and if it did why no developed resistance or immunity in the local population.
Viral epidemics and pandemics have started many times before in Chinese wet markets.
I survived the 1957 Asian flu but with permanent nervous system damage.
John sorry to hear that. I grew up and was educated in a different political system. I had two relatives who succumbed in their 40s to the radiation exposure, despite ‘total safety’ assurances from the relevant authorities, hence my scepticism.
Thanks.
Skepticism is warranted regarding all regimes, even those presumably enjoying popular support.
I’m also a Downwinder, exposed through air and milk to radiation via intentional releases from Hanford reactors, where US Pu was made.
BBC:
Dr Li Wenliang …. was summoned to the Public Security Bureau where he was told to sign a letter. In the letter he was accused of “making false comments” that had “severely disturbed the social order”.
“We solemnly warn you: If you keep being stubborn, with such impertinence, and continue this illegal activity, you will be brought to justice – is that understood?” Underneath in Dr Li’s handwriting is written: “Yes, I do.”
He was one of eight people who police said were being investigated for “spreading rumours”.
This sounded terribly familiar.
Yup. Standard Commie Operating Procedure.
However, the ChiCom regime acted more promptly this time around than with SARS.
Bat-borne coronaviruses aren’t unique to China. MERS apparently came from the Egyptian tomb bat, with camels as a possible intermediary host.
I wonder if Dr. Li’s demise was in any way “assisted” by the State…
Could be. The first report of his death was dismissed as premature.
Would Time dare make him Man of the Year, risking the wrath of Xi? Long time until end of 2020.
Curse of the Mummy Bat.
JT,
Where were you living ‘downwind”? We moved to Connell in 52 so we missed most of it, but neighbors got thyroid cancer and other maladies that showed up in the 60s.
I was in rural Umatilla County, OR. Older brother born 1948, I in 1950 and younger 1952.
Rapid long distance travel becoming commonplace is the difference.
Many people that live in Wuhan are not native to Wuhan. Perhaps the locals have resistance but new comers don’t. Perhaps a bat seller decided to get into the pangolin business and voila.
There was information circulating on an Indian study that claimed to have identified 4 protein inclusions from HIV-1 in the nCOV. Any more information on that? It would seem to indicate that the virus was man-made.
Possibly this study:
https://www.biorxiv.org/content/10.1101/2020.01.30.927871v1.full
Uncanny similarity of unique inserts in the 2019-nCoV spike protein to HIV-1 gp120 and Gag
Abstract
We are currently witnessing a major epidemic caused by the 2019 novel coronavirus (2019-nCoV). The evolution of 2019-nCoV remains elusive. We found 4 insertions in the spike glycoprotein (S) which are unique to the 2019-nCoV and are not present in other coronaviruses. Importantly, amino acid residues in all the 4 inserts have identity or similarity to those in the HIV-1 gp120 or HIV-1 Gag. Interestingly, despite the inserts being discontinuous on the primary amino acid sequence, 3D-modelling of the 2019-nCoV suggests that they converge to constitute the receptor binding site. The finding of 4 unique inserts in the 2019-nCoV, all of which have identity /similarity to amino acid residues in key structural proteins of HIV-1 is unlikely to be fortuitous in nature. This work provides yet unknown insights on 2019-nCoV and sheds light on the evolution and pathogenicity of this virus with important implications for diagnosis of this virus.
Conclusions
Our analysis of the spike glycoprotein of 2019-nCoV revealed several interesting findings: First, we identified 4 unique inserts in the 2019-nCoV spike glycoprotein that are not present in any other coronavirus reported till date. To our surprise, all the 4 inserts in the 2019-nCoV mapped to short segments of amino acids in the HIV-1 gp120 and Gag among all annotated virus proteins in the NCBI database. This uncanny similarity of novel inserts in the 2019-nCoV spike protein to HIV-1 gp120 and Gag is unlikely to be fortuitous. Further, 3D modelling suggests that atleast 3 of the unique inserts which are non-contiguous in the primary protein sequence of the 2019-nCoV spike glycoprotein converge to constitute the key components of the receptor binding site. Of note, all the 4 inserts have pI values of around 10 that may facilitate virus-host interactions. Taken together, our findings suggest unconventional evolution of 2019-nCoV that warrants further investigation. Our work highlights novel evolutionary aspects of the 2019-nCoV and has implications on the pathogenesis and diagnosis of this virus.
(97 comments)
My first thought was, there is no reason to think the worst, unless there is a reason to think that.
It has long been feared that gene transfer from another virus in a co-infected individual could be how a virus can acquire new characteristics and capabilities.
A deadly virus like AIDS or Ebola acquiring a respiratory component via coinfection has been hypothesized as a worst case scenario, leading to one of those diseases being able to be spread like the flu.
My next though was…short inserts?
How short?
How similar?
How experienced are these researchers in India?
Do they know what they are talking about?
It turns out, perhaps no, they do not.
They are not talking about proteins, but amino acid sequences.
Are they wrong that these sequences are not present in other coronaviruses?
Are they wrong that they are a match for HIV, and wrong that these sequences are unusual?
Some seem to think so:
“Gag sequence:
MGARASVLSG GELDRWEKIR LRPGGKKKYK LKHIVWASRE LERFAVNPGL LETSEGCRQI LGQLQPSLQT GSEELRSLYN TVATLYCVHQ RIEIKDTKEA LDKIEEEQNK SKKKAQQAAA DTGHSNQVSQ NYPIVQNIQG QMVHQAISPR TLNAWVKVVE EKAFSPEVIP MFSALSEGAT PQDLNTMLNT VGGHQAAMQM LKETINEEAA EWDRVHPVHA GPIAPGQMRE PRGSDIAGTT STLQEQIGWM TNNPPIPVGE IYKRWIILGL NKIVRMYSPT SILDIRQGPK EPFRDYVDRF YKTLRAEQAS QEVKNWMTET LLVQNANPDC KTILKALGPA ATLEEMMTAC QGVGGPGHKA RVLAEAMSQV TNSATIMMQR GNFRNQRKIV KCFNCGKEGH TARNCRAPRK KGCWKCGKEG HQMKDCTERQ ANFLGKIWPS YKGRPGNFLQ SRPEPTAPPE ESFRSGVETT TPPQKQEPID KELYPLTSLR SLFGNDPSSQ
Alleged “gag” match: QTNS——–PRRA
Actual gag sequence: QTNSSILMQRSNFKGPRRA
To begin with this is such a tiny random part of gag. Like 1%. It’s also not a 100% match. They just ignore the middle part and call it a match anyway.
Except this isn’t your standard HIV sequence for gag. It’s a unique isotype labs found in India. This sequence is NOT found in actual standard gag. Which is super confusing in general. Also the other matches are from 3 other strains of HIV. So it’s not even 4 of the same subtype which just makes this even more ridiculously terrible of a paper.”
“Trevor Bedford
@trvrb
· Jan 31, 2020
These short inserts do indeed exist in #nCoV2019 relative to its closest sequenced relative (BetaCoV/bat/Yunnan/RaTG13/2013, seen here
https://
nextstrain.org/groups/blab/sa
rs-like-cov
…). However, a simple BLAST of such short sequences shows match to a huge variety of organisms. No reason to conclude HIV.”
“To be clear, these observed insertions in spike protein are completely consistent with naturally occurring evolution in these viruses in bats. Spike has lots of evolutionary pressure and it mutates single bases as well as gains and loses sections across related bat viruses”
https://www.metabunk.org/threads/claims-of-hiv-protein-sequences-in-ncov-2019-coronavirus-report-withdrawn-by-authors.11103/
The paper was widely panned in short order, and was withdrawn by the author prior to Feb 1st.
Over two weeks ago.
Rud, thank you for pulling this together for us. I now see the Cruise Ship Lab Experiment is up to 136 cases, and I’m thinking tracing the contact routes of the infection might disclose additional data about this coronavirus. Imagine being trapped in this Hotel California arrangement?
Have a thought for the unfortunates on that cruise ship: most cabins are windowless, and the passengers are allowed only 90 minutes a day on deck.
Thanks for the summary, but I think the analogy to climate alarmism is mistaken, and the disease may ultimately be much worse than depicted here. The Chinese government does not want the alarm that may actually be appropriate. Even by official counts, deaths from the Wuhan virus already exceed those from SARS after a much shorter time. And there are indications that deaths are being greatly under-counted: many are attributed to other causes or not reported at all, and Wuhan crematoriums appear to be running at full tilt. Just today, China decided (against WHO guidance) that, even if someone tests positive for the virus, they will not be included in the count of new cases if their symptoms are not yet evident. So, there is the same lack of transparency as with climate alarmism, but this time the self-serving appeal is to complacency. I recommend Zero Hedge for a less filtered account of what might really be transpiring.
It is my experience that zerohedge is one step above Infowars so relying on them for accurate information is a dubious proposition.
The problem in determining how serious one of these novel viral infections are is that most people who contract will never see a doctor. That was most certainly true in 1919 epidemic. During the last killer flu panic virologists went back and examined tissues samples that exist from people who were alive during the epidemic. They were surprised to find that most had the antibodies for the Spanish flu. Basically, almost everybody got it. I can provide same anecdotal evidence from my family history. Everybody in father’s family had the flu and they all went to school and work because it was so mild. And here lies the explanation into why all thesr “killer” virus coming out of Asia seem to burn out when they hit the West. In Asia people only go the doctor when they are very sick so you only see the worst cases with the highest mortality rates. You don’t see the people who fight through the illness and get better without seeing the doctor. I would guess that in China that for every person who goes to the doctor there are 10 who the system never sees. They just get better on their own. It is easy to fall into the mirror image trap, that is, Americans go to the doctor at the drop of the hat so the Chinese must be doing the same thing.
Another factor in the low fatality rates for viral infections in the West is the use of the pneumonia vaccine in at risk populations. Corona and influenza virus seldom kill you. It is the secondary pneumococcal infections that do it. I doubt very much that many Chinese get the pneumonia vaccine as a standard vacvination
“I doubt very much that many Chinese get the pneumonia vaccine as a standard vacvination”
Speaking of which, is getting a pneumonia vaccine shot an effective means of defending against this Wuhan CoronaVirus? Pneumonia complications seem to be the way people are dying.
You should have every vaccination you can get.
I have gotten a polyvalent pneumococcal vaccine every five years since I was 21.
Get a meningococcal too while you are at it.
No charge if you have insurance, and Sam’s Club, Costco, CVS, Walgreens…they have them right there and the pharmacist can give them to you.
Actually there are now two kinds of pneumococcal vaccine available. Get both. And get a flu shot too.
Anything that activates your immune system is going to make your body more able to respond quickly.
Thanks, Nicholas. I think I’m up to date on my pneumonia vaccinations.
Have you got your rabies shots? A disease that is invariably fatal once symptoms appear, and that can be easily caught unwittingly by inhaling (spelunkers beware) or touching the saliva of an infected animal (if you have a break in your skin). I suspect my rather expensive series of vaccines has saved my life at least once . I can’t think of any other way my antibody titre could have tested at 10 times the minimum immunity threshold thirty years after initial vaccination with no boosters while my wife’s titre (innoculated from the same vials at the same time) tested one tenth of mine.
I hate caves, and if I ever get bit by a wild animal, there is plenty of time to get the shots.
The death rate in the US from Rabies is 0.0 per million people per year.
We have mandatory vaccination of all dogs and cats here, and since that went into effect, deaths from rabies has dropped to a case every now and then. Many years there are zero human cases, and rarely more than one or two in a year.
Domestic animal cases have gone from over 10,000 per year in the 1940s prior to the beginning or mandatory vaccines for dogs in 1947, to well under 100 a year in recent decades.
Rabies exists in wild animals all over the US, but hardly anyone ever gets the disease because people know to get medical attention in the case of a wild animal attack.
I bet even the guy who claims he does not believe in vaccines…would run not walk to get a rabies vaccination shot iffen he was bit by a raccoon.
BTW…there are at least 14 cases of people surviving rabies after beginning to show symptoms.
And this:
“Washing bites and scratches for 15 minutes with soap and water, povidone-iodine, or detergent may reduce the number of viral particles and may be somewhat effective at preventing transmission”
https://www.who.int/en/news-room/fact-sheets/detail/rabies
There is that minimum infective does thing again!
In the case of flu and flu like illnesses, it is most commonly the case that pneumonia as a complication is the result of a secondary infection.
I have not looked very closely at the particulars for SARS and MERS, so I am not sure if it is also the case with the corona virus illnesses, but I did take note of the observation that the disease progression seems like a normal cold or flu like one up until a certain period of time, and then there is a divergence where some people who had improving condition suddenly took a turn for the worse and became gravely ill rather than recovering.
This does suggest a secondary infection at a point in time that the patient is weakened and may be in a setting with resistant bacterial strains circulating.
Nosocomial infections are a whole thing apart from all else.
Best to stay out of hospitals unless you are gonna die without round the clock care, IMO.
It is a terrible irony that hospitals themselves have been the breeding ground for increased virulence and antibiotic resistance.
Go when you need to, leave when you can.
David I agree completely…
Never has China cranked up like this…..total lockdown on major cities…millions of people
…where did those spray trucks come from?
forced quarantine…
absolutely killing their economy
No one would do anything this severe if they didn’t know something….what do they know?
Yes, according to many internal leaks
past the communist firewall it is very bad.
Reasonable speculation is that those spray machines are military decontamination. AFAIK China has not even released what they are spraying.
“What do they know?” Answer, that mass quarantine have a good chance of stopping this. Furthermore, it makes them look decisive and caring even if overkill. Everyone is still getting paid and told they are helping society by staying home with pay. In these types of societies overkill is almost always the answer when the big bosses are paying attention.
whats weird is the amount of confirmed, but so few recovered? they mightnt have died but they must be pretty crook to still be hospitalised
the direct from hosp to crematorium makes sense
funerals and mourners would be a vector they sure dont need
just like with ebola
Very interesting, thank you.
I don’t suppose I could sucker you into answering why HIV is totally different than all other viruses, in that HIV supposedly makes the infected sick after the virus has passed on and only the marker cells of its past presence still remain?
Sure, I will bite. One of my board members was Andre Pernet, who as head of R&d at the Abbot Labs developed the first approved HIV antiviral.
Your description/supposition is just wrong on at least two counts. My comments are intended for you look stuff up before publicly demonstrating confusion.
1. It is not different. The virus ‘never’ passes on. The reason is that even with the best HIV antivirals, we cannot eliminate it in its quiescent ‘non-infective’ reservoirs in monocytes, non CD4 T cells, and such. Key word reservoirs.
2. HIV infects the CD4 ‘helper’ T cells, eventually eliminating them via viral replication and ‘burst cell budding’. You don’t die from HIV. You die from all the bad things that happen when the CD4 are insufficient to provide a functioning immune system. To cite two classics: Karposi’s Sarcoma and orophyrangeal thrush (a fungus of the oral mucosa). So in a sense the HIV ‘passed on because it killed the CD4s. But that profoundly misstates how the disease functions. Put differently, HIV was first called AIDS—Acquired Immune Deficiency Syndrome because that that was how it killed.
https://www.duesberg.com/
Duesberg argues that retroviruses like HIV must be harmless to survive: they do not kill cells and they do not cause cancer, he maintains. Duesberg writes, “retroviruses do not kill cells because they depend on viable cells for the replication of their RNA from viral DNA integrated into cellular DNA.”[1] Duesberg elsewhere states that “the typical virus reproduces by entering a living cell and commandeering the cell’s resources in order to make new virus particles, a process that ends with the disintegration of the dead cell.”[43]
Duesberg also rejects the involvement of retroviruses and other viruses in cancer. To him, virus-associated cancers are “freak accidents of nature” that do not warrant research programs such as the war on cancer. Duesberg rejects a role in cancer for numerous viruses, including leukemia viruses, Epstein–Barr virus, human papilloma virus, hepatitis B, feline leukemia virus, and human T-lymphotropic virus.[44]
I’d say the recent discoveries about cancer back up Duesburg, not his detractors. I don’t want to take away from your very informative post. I just don’t see much similarity between viral infections like the Wuhan virus and the virus we call HIV
call me a skeptic
Survival for any retrovirus such as aids is not dependent on the survival of the host cell any more than Malaria is dependent on the survival of an infected animal or human. It is only dependent on its ability to reproduce and move on before the death of the host cell. I don’t know Duesburg person’s work but the logic there is fatally flawed.
Duesberg was once respected as a pioneer of research in the role of retroviruses in human disease and cancer. Why he turned into a skeptic of his own research and that of many other virology researchers is unclear but the denial that HIV is the cause of AIDS or that retroviruses can trigger cancers goes against a huge body of reliable, well conducted research and all of what we have learned from the studies of HIV/AIDS. We should not let reputation persuade but rather the actual data and that all points in one direction. I have been involved in research at the epidemiological, clinical and basic science level in HIV/AIDS, which doesn’t guarantee anything about my statements being true, but does mean that I have a pretty good knowledge of the research literature.
I read Duesburg’s arguments 30 years ago and I couldn’t refute them. Back then everybody believed AIDS was going to kill everyone in Africa. It never slowed the population growth of any African country and its obvious that they don’t test for HIV to any scale in Africa, because it is very difficult to establish the presence. But when they do test in Africa the HIV is very, very common.
Anyway, HIV is behaving uniquely for a retro virus. Singularly unique. AIDS is the killer. How do we really know HIV causes AIDS? Every disease is to a great degree a failure of the immune system. If I die of tuberculosis and I am HIV positive, I die of HIV. If I die of TB and I am not HIV positive then I died of TB. The same with every HIV attributed death. There is no null hypothesis. There are lots and lots of HIV people living healthy lives, not just in Africa
Your arguments are not only dated and based on inaccurate info, but also several of your assertions are flat out wrong…contradicted by many layers of evidence.
And illogical.
When you say that “Back then everybody believed AIDS was going to kill everyone in Africa”, you are not stating a fact, but an opinion of the long ago opinions of “everybody” at a time unspecified.
Then you go on to make an argument based on this first idea not coming to pass.
Can you understand how ridiculous it is to dismiss the sum total of epidemiological, virological, and immunological evidence for not just HIV-AIDS, but by your own extension of logic several other ideas that are only connected by dint of having been originally made by the same person!
So let’s try to get a clear summation of the thread of logic: Back then, whenever then was, “everybody” thought AIDS was gonna kill everyone in Africa.
That has not happened, and in fact populations have increased.
Therefore HIV does not cause AIDS, viruses do not cause cancer, the war on cancer is a waste of money, there is no evidence that “Wuhan virus” and “the virus we call HIV” are in any way similar.
The fact is you demonstrate that you are highly misinformed, make sweeping assumptions, do not keep up with even the decades ago progress of the arguments you champion, let alone the now long and successful history of targeted antiviral therapy in fighting the progression of HIV-AIDS, or the dozens and dozens of different ways all of the assertions of the original band of HIV deniers have been disproven.
Try to follow the lead of former denialists in South Africa. People like Thabo Mbeki, and Barbara Hogan.
Have a look at the Durban Declaration, all the way back in 2000.
In fact even people like Duesburg and the Perth Group have shut their yaps, after the advent of one after another effective antiviral therapies, dozens and dozens of randomized double blind clinical trials, and many tens of thousands…hundreds of thousands by now…of people who have had their symptoms arrested and health restored by suppressing the HIV virus…which is all those drugs do…they do nothing else.
And if that was not enough…numerous people stopped taking them, and promptly got full blown AIDS.
Some went out of their way to help people avoid having to take life saving drugs, and some tragically let their own children die, before dying themselves, of the very thing they denied.
Others were tossed out of the denialist movement when they developed symptoms of AIDS, and promptly discovered God and started taking the worthless drugs. Those people are still alive. The people who scorned them are mostly dead.
https://www.latimes.com/archives/la-xpm-2005-sep-24-me-eliza24-story.html
https://web.archive.org/web/20080415232410/http://www.aegis.org/news/misc/2000/BG000201.html
How shocking to discover that many of these HIV deniers were in the business of selling people fake medicines, getting rich by charging huge amounts of money for such treatments as the miracle drugs sodium chloride, dihydrogen monoxide, or the dangerous colloidal silver.
I know what that reminds me of.
“…a process that ends with the disintegration of the dead cell.”
In virology the disintegration of the host cell is called lysing…the infected cell lyses and releases new virus particles.
But many viruses do not do this, and most of the ones that cause disease in humans do not do this.
Instead, virions bud out of the cell membrane.
At some point the cell may be engulfed by immune system cells, or initiate the preprogrammed cell death known as apoptosis.>
But it is simply not the case that the end point of the process is disintegration of the dead cell.
The longer a cell stays alive, the longer it is churning out new copies of the virus.
I do not generally like to use the term crank, as it is often used against people with whom someone merely disagrees.
But the amount of evidence one has to ignore is stupefyingly huge in order for someone to behave as Duesburg.
And how on Earth can anyone think that the weight of evidence is against cancers being caused by infectious organisms?
The argument that the war on cancer has anything to do with certain modes of carcinogenesis makes no sense. Who ever said the fight on cancer was only regarding viruses that cause cancer?
Almost everyone who gets hepatocellular carcinoma either has HBV or HCV. People that are coinfected with both have a greatly elevated risk.
As for seeing a similarity between two types of viruses, here are some pictures. One is of a corona virus, and the other is of HIV.
Are they more or less similar than fleas are to ticks?
Lions to sharks?
People with HIV virus get very sick and eventually get AIDS if not treated.
Direct acting antiviral drugs that are highly specific and targeted to various molecules in the HIV virus keep people who are infected from getting sick and dying, for a very long time. People who stop taking the drugs have a sudden and sharp rise in circulating virus, rapid diminishment in CD4 cells, and have a course of disease seen prior to when any such drugs were available.
No one who is not shown to have HIV viral RNA on blood serum PCR assay gets the disease called AIDS.
Everyone who has the disease gets sick and dies of AIDS without treatment.
In nearly every case, investigators have been able to trace the source of everyone who turns up having the disease, and the persons who passed it to that person have viral RNA that matches the new patient.
People that died many years prior to the disease being discovered and named, who had symptoms and a death that were at the time a medical mystery, have been exhumed and found to have viral RNA.
There is nothing very mysterious going on with how viruses cause and spread disease, or how it might be the case that a virus can cause mutations that accumulate to eventually cause a malignancy.
Not all details have been worked out, and viruses are not the only way that a cell can accumulate the various stages of genetic damage necessary for a cell to become cancerous.
Variations in the immune function of various individuals explains why all people do not have the same disease progression. Due to the incredible complexity of DNA…every cancer is unique. Every cancer starts out as a single cell that accumulated enough damage and acquired the ability to reproduce out of control, and then escaped the immune system.
The weight of the evidence against the ideas of someone like Duesburg is overwhelming.
But it is hardly unique that some people are able to be totally blind to mountains of information, and somehow focus on a few so-called “facts” that only they are in possession of.
We see it with antivaxxers, with warmistas, and with all manner of other people who just believe what they want to believe, all the while demonstrating that they are, in fact, spectacularly uninformed and ignorant.
Oops, forgot to attach the photos.
Here is HIV under a microscope by itself, and artist rendering of the virus, and a micrograph of virions budding from a live infected cell:
http://i.imgur.com/rCdvo2P.jpg
http://sexinfo.soc.ucsb.edu/sites/default/files/files/styles/large/public/field/image/hiv-virus_0.jpg
Now here is a corona virus, first a photo, then a rendering, then a picture of a live infected cell shedding human corona virus 229E:
And diagrams of some viruses.
Flu virus, corona virus, HIV, Hep B, Herpes Simplex
I for one have no problem seeing how they are similar. And distinct.
And a couple of more, of respiratory corona virus with a regular unenhanced photo and a rendering of the structure, and the same for HIV:

Mods, I posted a comment with numerous links to photos that is in moderation.
Thanks,
Nick
Have a child with cancer and watch all the quacks come out of the woodwork. I can remember when the conspiracy theory was cancers are caused by germs/viruses and not cell mutations. Of course there was probably literature on both ways.
What sucks is this sort of thinking will multiply when CAGW falls.
Scientists did us no favors however when they said stuff like there was no way to get HIV from dentist until there was.
Please post evidence of the usefulness of a vaccine.
Iron Argonaut,
It is evident that cancer is not one disease, it is a type of disease.
It does not have one or a few causes and/or pathways to the end stage illness, but many.
I am not sure who might have said something to the effect that it is impossible for a dentist to spread an infection such as HIV.
Obviously dentists are human beings.
They have no special immunity, or inability to pass along a virus.
So if anyone ever said that (and I am not doubting it, just unaware of the particulars you mention. I do know of the dentist who was infecting patients), they were being illogical.
What has become clear over time is that AIDS is not spread by casual contact, and the virus is not present in many bodily fluids such as saliva, or in excreta. To become infected takes some sort of blood to blood contact, such as two people with open sores or ulcers having unprotected sex, sharing needles or accidental needle sticks, etc. It is not a particularly easy virus to pass along. You need to get infected blood or blood product into your circulatory system. And the virus is fragile, more so than many viruses…it will not remain viable outside the body on surfaces for very long, etc.
So obviously an infected dentist, or some evil person who has infected blood in their possession, can infect other people, either inadvertently or purposefully, if unsafe practices occur.
It is important to keep in mind that individuals are not monolithic in thinking, in their manner of speaking, or in their level of knowledge, no matter who they are or what education they have.
A guy who is a scientist saying something is not the same thing as “scientists say”.
Not that it really matters…as every scientist in the world can be, and frequently has been, wrong about an infinity of separate issues.
The history of science is a compendium of people being shown to be wrong about one thing after another. It is more than that…but it is that.
As a last word…I am not a fan of the phrase or the habit of using the phrase “conspiracy theory, or associated phraseology.
The idea that there are no conspiracies is an outrageous lie, and the phrase itself has been crafted and deployed as a form of broad-spectrum gaslighting.
People collude.
They conspire.
They meet, discuss, make plans, exchange ideas, set goals, devise methods for achieving those goals.
In day to day life such activity is referred to as having a meeting, or a conference, or a gang, or a club, or a congress. And a conspiracy is by definition when two or more people discuss breaking some law or engaging in some illegal activity.
Who thinks that never happens?
And what is illegal is entirely subjective.
They still use the term AIDS, as in “full blown AIDS”, to identifying the end stage illness, but it is distinct from the virus, called HIV.
HIV/AIDS is considered a disease spectrum.
The virus was originally called HTLV III, for Human T Cell Lymphotropic Virus.
AIDS is still how it kills those who it kills.
Which is a small number here in the US these days.
But people do still die of it.
Some people just stop taking the medicine.
Many are addicts or mentally ill.
And nothing works for everyone, although the HAART regimen is ~95% effective within the first year.
Another issue is…many do not know they have it until they are well past the point they should have begun treatment.
Glad your feeling better Rud. Thanks for the write up. Interesting per usual.
I have viewed much discussion on ACE2 receptors being more prevalent (5x) in some Asian populations and place a higher risk of catching the virus.
I have often wondered if the Western vaccination regiments might play a role in resistance to such infections.
Initial data was pointing to more male (71% if memory serves) than female infections, but could be simply related to customs or environmental exposure levels. There does seem to be significant predisposition to many with existing health issues. I suppose we shall know more upon ultimate reanalysis.
Excellent summation of what is known and what is suspected.
https://www.cdc.gov/flu/weekly/index.htm
Best estimate for the 2019/2020 flu season is:
Total cases: 400 000 000 world wide, 19 000 000 US only
In Hospital 2 000 000 world wide , 100 000 US only
Total deaths (complications related to Flu or ILI (Influenza like Illness) 200 00 world wide, 10 000 US only.
Even if we assume that China is only reporting 1 in a 100 cases the numbers for nCOV would be 4 000 000 cases with 86 500 deaths.
I think Influenza is still the greater threat at this time.
P.S. During a “bad” flu season there are 80 000+ deaths just in the USA
John G
John
I was shocked and sceptical about your figures and checked those for the UK
“Public Health England told ITV News: “The number of flu cases and deaths due to flu-related complications varies each flu season.
“The average number of deaths in England for the last five seasons, 2014/15 to 2018/19, was 17,000 deaths annually.
“This ranged from 1,692 deaths last season, 2018/19, to 28,330 deaths in 2014/15.”
Since October, over 4,000 people with confirmed flu have been admitted to hospitals in England with 70 confirmed deaths.”
Some 25 million people most at risk receive a flu inoculation out of the UK population of around 65 million. Bearing in mind the relative sizes of our countries the number of deaths is very similar.
Puts the Wuhan virus into context but now it has set me worrying about flu!
tonyb
Hi TonyB, as the article above states we are talking about 2 different transmission pathways but using hand gels frequently when in public and avoiding people that are sick (encourage co workers that are sick to stay home) can provide some protection.
Flu vaccines work even when the powers that be guess the wrong combination of HxNy it will prime your immune system. In the US vaccine compliance is 40%-45% of the population I did not know that it was less than that in the UK since you have free healthcare.
John G
Flu shots are free in the US, with Medicare and most other insurances, or even without. Stores treat them as loss leaders to get people in.
I learned this year there are two different versions of the annual flu shot offered. The standard given to most people in “free” programs which costs about $40.00 and one that is claimed to be slightly more effective which costs $60.00. I was paying for mine and opted for the more expensive.
Did you find out what the difference is? Does the more expensive one cover more strains?
Rah and Mark W. I know the answer(s) to your question. There are two.
First and most common is dose. It can be ‘high’ or ‘low’. All medical personnel receive the ‘high’ dose automatically, for obvious reasons. Since the production process (incubation in fertilized chicken eggs, then virion extraction, purification, and inactivation) is identical, the high dose must cost more. A CVS ‘freebie’ is guaranteed low dose.
Second, and less common, is adjuvant vaccine enhancement. Adjuvants are additives that give a dose an immune boost. This was a BIG deal with 2009 swine flu since everybody knew it was a race against time and supply would be limited. A lower dose plus adjuvant produced more total doses. FLUAD is one such vaccine recommended by CDC for this year: a standard trivalent inactivated virus at ‘low dose’ plus adjuvant.
The better of the two standards is the Adjuvanted flu shot which is supposed to cause an enhanced immune response. Most often given to people 65 y/o or older. I’m 64 and opted for it.
Thanks Rus, I’m sure the one they offered me and I got was the Adjuvanted and not the high dose.
From what I’ve read pharmacies in the US get paid by insurance companies to administer flu shots. It’s something they are paid enough for that they can offer gift certificates to the people they administer the shots to.
https://www.seattletimes.com/nation-world/flu-shots-at-the-pharmacy-easy-for-the-patient-profitable-for-the-retailer/
I think there is also another version that is for kids that is not a shot but something they rub on your nasal membranes.
Oh, I see …it is a nasal spray.
It is made from a live virus but weakened.
As for those huge numbers of deaths…almost all of them are people who are very old, although it also includes some newborns and infants.
And some other people who are very sick with something.
And many are killed by secondary pneumonia or other infections.
When someone gets very frail, as in end of life stage, flu is often the straw that breaks the camels back.
Pandemic flu, in particular Spanish Flu, killed a high proportion of young healthy people.
There have been several reasons put forth for this odd fact, with one more recent one (recent as in the past few decades) is that they died because they had a very sudden and strong, overwhelmingly strong, immune response. In this scenario, these people died of something called cytokine storm. Also known as cytokine release syndrome, or infusion reaction (this from people who had it for a different reason-monoclonal antibody drug therapy).
Basically a runaway immune reaction feedback loop.
Eric
The company I work for provides the cheaper shot free but only for those that attend the quarterly safety meeting at which it is given. Thus covering the flu shot is not included in my company health insurance when given by a doctor or at a pharmacy. I did not attend that meeting and so went to the pharmacy we use for my flue shot and paid for it out of my own pocket.
“Free” dental work is why 10% have done self dental work. So, is getting the flu shot easier or harder in UK. Price is same since all insurance in US covers it and everyone has insurance now that it is mandatory.
John
What percentage of those that died were vaccinated. Do they ever bother to find out.
Regards
The vaccine effectiveness data is scheduled for release next week.
Vaccines are never tested almost by definition, so how can you measure their effectiveness (whatever that is)?
If what you said was true, there would be no such thing as vaccines that are not approved because they are shown not to work.
Here are 9017 clinical trials, either proposed, under way, or completed, in which vaccines are being tested.
Each one has all of the information about the trials…what the goal is, what the protocol is, the endpoint of the study, what stage trial it is.
Completed studies have links to the data.
All show which sites are conducting trials, which the specific contact people are, who can be contacted if one wants to enroll, the names of the research institutions and the researchers at each site, the manufacturer of the intervention, etc.
That is 9017 of something you claim does not exist.
You can click on any number of filters, such as studies which have been suspended, those that are recruiting, those that are completed, withdrawn, terminated, active…etc.
They can be sorted by eligibility criteria.
By type (interventional, observational, etc).
By phase of the trials.
By how they are being funded.
And by results, either with or without.
If you would like to see a few tens of thousands of more once you read through these…let me know.
You have no clue what the hell you are talking about…and just make stuff up.
Really dumb stuff, too.
https://clinicaltrials.gov/ct2/results?cond=&term=vaccine&cntry=&state=&city=&dist=
niceguy, you asked above: “How do you know a vaccine works?”
Take a disease like Polio (Poliomyelitis), which afflicted my Mom and who lived out the remainder of her life, after contracting Polio, unable to walk unassisted. She contracted Polio about the time the vaccine was being developed by Dr. Salk, and a few years after I was born (so I remember a time, early on, when my Mom COULD walk unassisted).
Polio vaccines were distributed, as I recall, via little square sugar cubes when I was a kid. I could not tell you the year, but I remember distinctly ‘the drill’ involving the sugar cubes.
Now I will ask you: When was the last time YOU saw a Polio victim, or heard about the use of what was called an IRON LUNG (in the day) that kept a full-blown Polio victim alive, as those patients were unable to breath unassisted due to having contracted Polio?
“Polio (Poliomyelitis), which afflicted my Mom”
Prove it.
There is no evidence polio vaccines did more good than harm.
“When was the last time YOU saw a Polio victim,”
Please explain what you mean. You make no sense.
What the hell is “polio”?
re: ” What the hell is “polio”? ”
Look it up.
You seem to profess to know everything; Do some leg work …
niceguy (a moron) re: “There is no evidence polio vaccines did more good than harm.”
You’re a full-blown idiot. That’s NOW been established.
Mods, ban this MFer. One cannot “fix stupid” of this magnitude.
“Completed studies have links to the data.”
And the data doesn’t prove that the vaccine protects against anything, and multiple female died during the testing of one your magical drugs. And nobody cares in your “science” demented cult.
Hah!
As I said…you were lying when you said you were done making a complete fool of yourself.
I can tell you still have plenty of witless remarks in you.
And do not go moving the goalposts…you assured everyone that:
“Vaccines are never tested almost by definition, so how can you measure their effectiveness (whatever that is)?”
But now you have conceded that you started out with a pure lie when you said
“during the testing of one your magical drugs.”
Moving the goal posts, is that what you want to do?
So you are abandoning your original lie?
Now you want to go off on a fresh thread of jackassery?
Just want to be clear…we are moving on from your first set of lies then?
That’s from October. You are comparing some thing that was barely noticeable in January to something that’s been around 3 months longer. On a virus spread which has quadratic to exponential growth. If a virus is doubling incidence every week there’s an ~2^10 difference in the comparison. 400 000 000 / 1024 = 400 000. Not a huge difference to the suspected 100 000 Corona cases we have now.
You should be comparing November’s Flu numbers if you want to compare against nCov2019
Also note hospitalization rate of Flu is 0.5%. Corona virus is an order of magnitude higher than that, which puts tremendous stress on the healthcare system. This stress is likely one of the reasons most of the deaths are in Wuhan – they simply don’t have enough equipment or beds to handle complicated issues like lung failure. Other places haven’t reached that stress level, yet. I hope they don’t.
Peter
Numbers are the current flu outbreak which for the US started on 9/29/2019 so we are in week 17 for reporting purposes. Last numbers are:
Total cases 22 000 000
In Hospital 210 000
Deaths 12000 including 78 children
https://www.cdc.gov/flu/weekly/index.htm
Current nCOV numbers are I believe based on first case 12/1/2019 so now in week 10 or 11.
The number of cases in the media are total cases since that date not current infected if you have a different source please let me know.
John G
The flu outbreak didn’t start on 9/29. that’s just the first day of the flu season by convention.
This year’s flu season started with 136 tested cases. See:
https://www.cdc.gov/flu/weekly/weeklyarchives2019-2020/data/whoAllregt_cl05.html
There was zero tested cases for nCov on 12/1/2019. nCov probably didn’t hit 136 tested cases till early mid-January. On Jan 26 there were ~2400 confirmed cases and it was doubling every 2 days back then. 2400/136 = 17, or about 8-10 days worth of growth.
Exponential scales are funny that way.
So it’s likely a delta of 12 weeks, not 6-7 as you calculate.
Correct started with 260 cases. (type A + type B)
So that’s 10x the starting count of nCov2019 on Dec 1.
I have never been “tested” I have had flu with vaccines and without. Dr says you have flu and slight pneumonia if still sick in a few days come back. I don’t bother going unless on deathbed not worth the drive when sick. So, I think all are just estimates except maybe deaths.
your flu is what we had downunder pretty much
the Vic B strain nd a(then) un named A strain did the damageas well as some H1N1
the vax was pretty close to useless
elder vaccines on their own info label even the ramped up doses are around 29 to 32% effective.
and the flu and pnumonia vaccines should NOT be given together
bu in Aus they over rode the maker advice and did double shots
they counteract
explains why many of the vaccinated got crook
the pnumonia is the BIG risk stuff the flu shot and go for the Pnumonia one.
I copped in last march( got in early lucky me) knocked me rotten for 10+days= 2 courses abiotics for the pnumonia
Peter Sable
Thanks for the accurate comment.
Pretty good overview…but not enough flaming hair, people jumping from out of windows, and cats&dogs…well, you know.
A few additional remarks since I love reading about viruses.
Viruses tend to spread further and faster in dry air. Scientists do not necessarily know why, but the conjectures are: 1) People tend to spend more time close to each other in winter, 2) humid air causes the tiny mucus droplets that people sneeze to settle to the ground faster thus reducing chance of breathing them in, and 3) humid air in itself might help to break down viral coatings faster. Another finding seems to be that warmer air breaks down viral envelopes faster, so warm air and humid air are just be correlated. In any case, if the Coronavirus continues to spread, it should slow down as summer approaches.
Virus genetic materials are a but more complex than indicated and its important to understand how if you want to understand risk. As mentioned, viral genetic information can be stored as either DNA or RNA. It can be positive-sense or negative (you might have to make more translations to get working code). It can also be kept in one or more loops or strands – and this is extremely important.
In general, DNA code is more stable then RNA code and so will be preserved with more fidelity. If you have a negative-sense type of material, it has to be copied at least once to make a working copy (a positive transcript). Each time a copy occurs, you have a chance to mutate… RNA loves to mutate so you get a much faster mutation rate with RNA than DNA, (Genetic drift is faster) There are also “Retro” viruses – these are really bad in that once you are infected, it’s for life (think Chicken Pox which later in your life is called Shingles). The Coronavirus is not a retro-virus (yeah!)
The Flu type viruses have either 7 or 8 strands of RNA virus. (Yeah, they can’t even agree on how many strands they want). Typical Flu viruses that infect people have 8 strands. If a single person (or pig, or whatever host) manages to be infected with more than a single Flu virus, they can swap strands. Now think carefully about this – not only are the genetic materials mutating quickly, but the viruses are essentially swapping parts to build brand new never seen before viruses. This is why the FLU is so dangerous and is so hard to stop – it just mutates past any barriers you build. The coronavirus is single stranded (yeah!)
One other notable behavior thanks to evolution – a specific virus strain will “tend” to evolve into less dangerous forms given time. This has to do with breeding success – the virus becomes more successful if it doesn’t harm the host while making copies of itself and spreading the infection. This is often referred to (mainly in the past) as a disease “burning out”. If a population gets the virus and doesn’t have symptoms then they likely will never even know it – the virus has essentially become invisible.
So the current coronavirus – is a positive sense single stranded non-retro RNA. Positive is good (fewer mutations). Single Strand is really good (fewer mutations and harder to swap genes). Non-Retro is good (not infected for life) RNA is bad (faster mutation rate). This all means its mutation rate is likely slow for an RNA based virus, it will likely remain a killer for a while (maybe years, maybe forever), it will likely seem to almost vanish in the summer (northern hemisphere) and reappear in winter. We have no vaccines, but do have medicines that can slow replication. Scientists have been working on vaccines for coronaviruses for many years, so the quick development of a vaccine is unlikely.
One other troubling report – but not sure it is correct so take with a grain of salt- is the onset of catching the new coronavirus might be followed by diarrhea, and then 7 to 10 days later by respiratory symptoms. If true, this would be very bad as that would mean the virus has more than one mode of transmission and a person is likely infectious for a longer period of time. The only protection? Don’t touch anything in public you don’t have to and lots and lots of hand washing.
R of T
All excellent points. I skipped them because the post was already long and complicated. Stuck with only the most basic RNA/DNA genetic distinction, brought home by the PCF military vaccine example.
Regards.
Thanks. I thought you did an excellent overview.
It will be interesting to plot the course of this disease based on its behavior and genetic makeup. I just do not imagine it becoming much worse (that is more deadly per people identified with the disease) given how it spreads, but viruses can mutate without warning into something more troublesome. It would be interesting to study if this is the first time the disease has actually spread, as opposed to the first time it was detected.
Thought of something else to bring up for those taking precautions: Hand sanitizers do not necessarily work well on viruses (they advertise as antibacterial, not antiviral). The best option is soap and running (obviously clean) water along with a good scrubbing. Try not to handle door handles on the way out of a bathroom – use a paper towel.
Ethanol (or any alcohol) based cleansers (that you use in absence of running water) *may(?)* help on a coronavirus because it has an envelope, but will not work on many other common viruses. There are other types of hand sanitizers that should be more effective (but soap and water is still best).
Hypochlorous based sanitizers will likely work better, and work much better on non-enveloped viruses.
I am putting in a link for those interested:
https://bitesizebio.com/3933/does-hand-sanitizer-and-liquid-hand-soap-remove-viruses/
No matter what you use you need to wash your hands first.
Alcohol based products will not be effective in the presence of organic matter.
And dirt is like microbe village.
Your hands have to be clean to have any chance of disinfecting them.
Soap and water work by rinsing them away, not by disinfection.
Again…it is a numbers game.
Ten virions will not make you sick.
But ten thousand might.
How similar is that really?
When folks make comparisons of DNA percentages, I get seriously confused. I have no clue whether 96% should be considered close or not.
The issue is confused by citing comparisons of “genes”, ie protein coating sequences, and of whole genomes, without clearly distinguishing.
With viruses, the complication is multiplied by the high mutation rate of RNA viruses. The Wuhan and SARS coronaviruses are close enough to bat coronaviruses to make the connection highly probable.
It’s actually even more complicated than that. You can also compare how similar are the genes that organisms do share. That’s how the oft-cited comically high similarity between humans and bananas was generated.
https://science.howstuffworks.com/life/genetic/people-bananas-share-dna.htm
Thanks for the link. It’s enlightening. I am now slightly less clueless. 🙂
For whatever help I was, you’re welcome. It’s often hard to tell what’s being compared, ie genes or the whole genome. Or in the banana case, similarity in sequence among those genes which are shared.
“The Wuhan and SARS coronaviruses are close enough to bat coronaviruses to make the connection highly probable”
Interesting comments. Would love a rational discussion on the Wuhan lab and that possibility. Yes, not disagreeing that nature is messy. However bat Coronaviruses with SARS similarities and transmission to humans is exactly what the lab was studying and fearful of. ( They warned about this very senario) The lab had mistakes happen in the past. Their are credible sounding reports of other evidence of human insertion. I will find them and post them, and would be happy to see them debunked.
I don’t know enough to rule out an escape from a bioweapon lab, as with the 1979 (then) Sverdlovsk anthrax incident, but wet markets or other natural source in my ill-informed opinion remains more likely.
Yet keep on mind, I am not saying a bio – weapon. The reports I read indicated they expected this scenario most exactly, they even indicated they created it in the lab in an effort to develope an antidote.
Yes, nature is messy, yet human hubris is not to be underestimated.
Ah, here I think is the link to one report, speculation ( especially the title) mixed with good research.
https://web.archive.org/web/20200203110836/https://medium.com/@realAdrianBond/coronavirus-exposed-part-1-communist-coverup-or-pandemic-bioweapon-of-mass-destruction-229ad482c0d3
They said it was a bat virus. But they had the idea it was a snake virus first.
And now it’s a pangolin…
They don’t know anything for sure!
4% is, quite a bit…Lets put it this way…humans and eastern gorillas are virtually identical. There is a 1.6% difference in genetics between us humans and gorillas.
But yet we are not alike at all.
The percentages aren’t comparing the same thing.
In terms of proteins, such as blood groups, humans and other great apes are indeed very similar. The differences are in control sequences, ie for instance whether jaws, arms, legs or body hair grow long or short, teeth large or small, etc.
CB, there is a math answer. Chimps and humans code for on the order of 30000 genes (I skip the quibbles about introns/exons, and so proteins per gene. The quibble is that on average >1 so even a gene to gene comparison is only approximate from what we know now.)
Those genes comprise about 100million base pairs out of about 2 billion total DNA base pairs (the rest is two things, true Junk dna, and supplemental epigenetic gene expression coding, anything but Junk).
The Wuhan Corona has slightly less than 30000 total base pairs, all likely coding for a single protein. Much simpler, so a 96% overlap is VERY tight, where in chimp/human the same metric is very loose. One metric, but apples to oranges use comparison. Excellent point.
The close to 30,000 base pairs in the Wuhan coronavirus code for about ten genes, ie proteins, not just one.
https://eurekalert.org/pub_releases/2020-02/uoc–ugb020720.php
It was once thought that the human genome included 30,000 genes, but that’s now down to 19,000 and possibly still falling. Our genome consists of around three billion bp, ie ~100,000 times as many as the virus, with only 1900 as many times genes. We have to conduct metabolism and reproduce ourselves, but the big difference is in non-protein-coding genome. Sequences formerly known as junk.
John, you thankfully caught my mispeak. I meant to say that each of the genes in those 30000 base pairs likely codes one protein. Impossible that the whole does only one, since ciral replication requires several. I chalk the goof up to day 10 recovery medicine—Jim Beam neat.
Virologists use the term polyprotein to describe the initial translation product. The poly protein product then gets cleaved by a chymotrypsin-like protease produced from the first vRNA open reading frame. Ultimately during the trascription of the (-) strand, viral mRNAs that are translated are produced in the infected cell. So the 30Kb RNA viral genome codes for many proteins. SARS-CoV was noted for it use of many non-structural proteins near the 3′ end of its genome that have no role in cell culture replication, but their functions are unknown in humans. The problem is that only cynomolgus macques are the only animal host that develops a SARS-CoV pulmonary disease like humans, so experimentation is quite difficult.
Yeah, they used to think the glial cells, which are the majority of the cells in the brain, do not do much except for to provide support for the neurons.
(Actually a quick check before sending this comment reveals that, while it was not long ago “accepted wisdom”, AKA it was known, that glial cells were the vast majority of the cells in the brain, now it seems at least one study indicates it may be closer to 1:1 or less.)
In truth there may be zero junk DNA.
Imagine not knowing anything about written language, and finding a library full of books, and the books all had only one interesting page…the cover with those nice drawings! And a bunch of useless junk clogging up the rest of the pages.
Rud,
Terminology matters.
CoV has a single strand RNA nucleotide sequence.
CoV does not have base-pairs like the double stranded helix of genomic chromosomal DNA.
The RNA strand is a string of nucleotides that can form hair pin loops, and foldings to make complex 3D structural signals like a string of peptides does to fold into protein structural motifs.
As far a human-chimpanzee genome comparisons, the real difference is not in the genes themselves, but expression patterns locked in by positional effects of the gene located into long strings of “junk,” which is certainly not junk. Your junk are things like non-coding silencer sequences, and enhancer sequences that interact with transcription factors to control gene expression patterns particularly during embryonic development the vast majority of which are epigenetically shut down soon after patterns are set in the developing embryo.
Joel,
Good point. Not base pairs but just nucleobases in coronaviruses.
Yesterday’s junk is today’s control sequences. Species can and do have nearly identical protein sequences in the few percent of genomes that are technically “genes”, but still be as different phenotypically as teosinte and corn (maize) or chimps and humans.
Rud,
I figured. A Brit in Wuhan claimed that he cured himself with whisky and honey, shunning Chinese medicaments until the whisky ran out.
At the very least, three nucleobases code for one amino acid in a protein, plus start and stop codons. An average protein might be a polymer hundreds of amino acids long. Shorter oligomers can have functions however.
Some of the confusion is in the details of how many genetic “parts” there are and whether sex is used to perform segment swapping. No sex exchange of materials in viruses (unless you count the accidental swapping of entire strands).
If you have one strand of genetic material the changes are all due to mutation (Coronavirus). DNA mutates fairly slowly, and RNA relatively fast. If two same-species virus are 95% similar and use DNA, they could be separated by thousands of years. If they use RNA, they might only be separated by tens (or less) of years. So knowing the kind of genetic material is important to understanding how “time dependent related” they likely are.
If you are dealing with multiple strands like in a FLU virus, it gets harder. Two viruses can swap one (or more) of several strands in a single infection (one host) and come out looking like very different viruses from a genetic comparison. Only by looking at entire strands and looking for their origin can we determine that the virus is a hybrid (sort of…I am using hybrid in lack of a better term).
This is why having animals and humans in close proximity can be so dangerous. If you have viruses that rarely cross over species, but can, it eventually can lead to one host that has caught a virus that it is already adapted to exchanging genetics with a virus it has no immunity to. They can (but often don’t) produce a really dangerous virus that spreads among the host’s species, until an immunity level is reached or the virus mutates into something kinder and gentler.
So, in a corona virus you would expect the genetic similarity to be pretty high (say 90% to 99%) if recently evolved from a similar virus (say last 30 years). Being 75% or so genetically related indicates it must be older (likely a lot older), or they haven’t found the brother/sister virus it evolved from yet. It is only about 80% or so similar to the SARS-CoV – again this is not very closely related and makes this new virus novel.
CommieB
If you look closely at that oft-cited connection between chimps and humans, you will find that the genes are the same but not even on the same chromosome a lot of the time. It is a bit of a stretch to draw conclusions about descent between two creatures that have to live in the same climate, eat the same food and generally have the same shape. There are some very complex differences between humans and chimps, one being speech and the development of the physical components needed to do it. Did you know that human babies can drink and breathe at the same time? The hardware needed later turns into the ability to speak.
Being genetically similar doesn’t say much. One gets the impression that the whole genome is put together “in the same order” but if you look at where the genes are and how they are expressed, there are many, many differences between chimp and human DNA. As the Darwinists are still fighting the Lamarkians we ordinary have have to put up with the fallout.
Remember when they used to say that gorillas are so close to humans in terms of evolution, all the proofs of this and that? Now it turns out they are quite remote having separated from others apes a really long time ago. So much for the “similarity of appearance and behaviour means descent” argument. Coincidence is not cause. I think we learned a few lessons about that in Climate Science School.
Human and chimp genes are on the same chromosomes. That applies as well to the two smaller great ape chromosomes which fused to form human #2.
There no valid arguments against the inference of shared ancestry and all the evidence in the world for it. Humans adapted to a different environment from chimps and bonobos.
Yep. My favorite example is that there are fish, mammals, and dinosaurs which are quite similar in appearance. link Form follows function.
Yup. Convergent evolution in not closely related groups is common, since we’re all subject to the laws of physics. Compare and contrast vertebrate and cephalopod eyes. But the differences are as important as the similarities.
The anatomical, embryological, proteomic and genetic differences between dolphins, ichthyosaurs and tuna show their separate descent from a common vertebrate ancestor.
Humans and gorillas share blood groups. Our last common ancestor lived around ten million years ago. For chimps, about seven million and orangutans, 12 to 15.
However, there has been rapid evolution during those ~6 million years between the two ape species’ Y chromosomes:
https://www.nature.com/articles/nature08700
Darwin was a Lamarckist. He accepted the inheritance of acquired traits, in addition to those acquired via selection and as a source of new variation upon which selection could work.
Regrettably, neither Darwin nor any other British naturalist seems to have read Mendel. The nature of inheritance thus remained obscure to them until early in the 20th century.
Noe-Lamackian inheritance, based upon epigenetic sequences rather than genes in the genome, in no way invalidates the reality of evolution via other processes.
Neo.
Good, but a couple of small corrections. 1 In modern classification, there are three domains of life: Bacteria, Archaea and Eukarya. Bacteria and Archaea together constitute Prokaryotes. 2 Cyanobacteria are almost certainly not at the root of the Eukarya tree: there are various theories on this, but as far as I know all see the rise of algae and plants as a secondary symbiosis of cyanobacteria with early eukaryotes.
That’s right, but the addition of Cyanobacteria in one eukaryote line happened soon after the endosymbiosis of an archaean and alphaproteobacterium to create the first eukaryote with a mitochondrion. Origin of the nucleus might owe to a megavirus.
There likely have been numerous symbiotic transformations in the Eukaryotes line – 1) Nucleus 2) Mitochondria, 3) Chloroplast – just to name the most likely.
I have always wondered if the virus developed from the development of a defense mechanism (it’s a great way to kill a competing cell) or from the gradual loss of genetic material from a parasite cell. It could be the virus developed many times from different beginnings.
The key endosymbiosis to form the mitochondrion apparently happened just once. Same for chloroplast, although algae were subsequently also engulfed.
Good information thanks to Rud.
My two children have severely compromised immune systems because of total kidney failure. They are on dialysis awaiting transplants and are very anxious about their catching this rather nasty virus. I have forwarded this to them both, they live on different continents, and I am sure this article will help them with their efforts to stay safe.
Thanks.
Excellent analysis Rud.
One major difference between epidemics and “Climate Change” is that epidemics are historically shown to be, well, viral in nature, meaning a positive feedback loop (Rho being greater than one), often quadratic but sometimes exponential.
The Climate, however, is self regulating with negative feedback loops, as Willis has clearly shown.
So the underlying math comparing the two is different (or rather opposite). So the risk mitigation should be different between the two.
If the US government is not busy building out inventories of N95 masks and respiratory assistance (O2, ventilators, etc), as well as figuring out how to quarantine 10s of thousands of people, then I’m very disappointed. It’s quite okay to spend a few billion now just in case. Because you can’t spend it later. And some of the stuff like emergency housing will last long enough for the next epidemic.
I’m reasonably confident that our government is doing so. I’ve been rather impressed by the administration’s response. Adult, no panicking, just doing the right stuff
I visit a local hospital regularly for check-ups and an exercise class.
They seem to be doing a tolerably good job.
If you have flu symptoms – visiting the hospital is not allowed. Lots of signs about that. And last Wed the intake nurses started asking about visits to China.
The intake nurses are not wearing masks. Yet.
Thanks so much, Rud, this is very helpful as our family has been pondering a long planned vacation tour of China later this year. We’re not sure what to do, however, you’ve given us a wealth of knowledge in a concise and comprehensible form to assist our decision making.
China has a history of rapid responses to virus, Sars, bird flu and swine flu all met with organised press conferences often along side WHO when only a few cases were known.
Active culling/detergent spraying and quarantine/treatment were swift.
On this occasion, almost nothing has been done, it was still an ‘unidentified mystery pneumonia’ in January and then suddenly they quarantined cities containing millions of people.
My guess is several factors come into play which lulled authorities there into a false sense of security, all the while a ticking time bomb progressed.
The lull is the incubation period together with symptoms which appear mild initially, perhaps with a recovery followed by descent into ICU required treatment of pneumonia.
The time bomb is asymptomatic viral shedding, effective transmission rate and capacity of hospitals.
So, by the time they’d not concerned themselves with the disease, many people were infected, suddenly a whole host of intensive care patients landed on their laps and the maths is obvious, if you cant care for the rapidly increasing volumes, the death rate will involve many of the 25% or so that require ICU.
Therefore, shut the cities, prevent spread….it had already unwittingly got too far.
Add general lung issues in the cities due to bad pollution issues….and you may have a reason this hasn’t yet impacted the west with severe symptoms??
Surely you jest. The ChiCom regime has an abysmal record in responding in a timely fashion to viral outbreaks:
https://www.nature.com/articles/s41591-020-0771-1
An interesting development possibly related………. or not.
https://www.justice.gov/opa/pr/harvard-university-professor-and-two-chinese-nationals-charged-three-separate-china-related
Dr. Charles Leiber is chair of Harvard University’s Department of Chemical and Chemical Biological and helped set up a chemical/biological research facility at Wuhan University of Technology.
This morning in the UK: Police ‘wearing hazmat suits’ will be able to HANDCUFF suspected coronavirus infected people and force them into quarantine !
People forcibly removed from homes and sent to quarantine. This is pretty crazy footage from China…the flu might kill 10000s a year, but they arent doing this if you have it.
The last part of the video is shortened, the original shows 2 people being forced into the box in the bed of the pickup…
China is way more worried about this than they are admitting in the press…
https://www.nbcnews.com/news/amp/ncna1133096?__twitter_impression=true
I would like to know what that guy kept repeating.
Lots of Western academics and business people have been suborned by the massive ChiCom military and industrial espionage program. The USSR’s programs were also successful, but faced greater financial and counterespionage obstacles.
Both regimes saved hundreds of billions in R&D by stealing and buying secrets. Or were given them in return for camoaign cash, as in the Clinton’s case with China.
Sec State Pompeo just shot a 16″ round across the bows of US Governors. This video is very much worth a watch.
https://twitter.com/TeaBoots/status/1226526914275368961
Strange how to study the SARS virus one must have a BSL Level 3 or four to study the live virus as it only exists in a lab.
Coincidently there is a BSL level four in Wuhan, China. And it is the only one in China. The Wuhan Institute of Virology (WIV) and it has played a central role in the outbreak.
To continue the virology department is run by Shi Zhengli. Shi and Cui Jie found the SARS virus originated in bats. And holds the largest database of bat virus.
Could Wuhan city because of their strange eating habits be the center of research on new and improved virology? Inquiring minds wish to know…is there another place besides cruise ships, to study viruses…hmm maybe fish and exotic food markets.
Shi Zhengli was quoted in a couple of articles as stating…
“I swear with my life, [the virus] has nothing to do with the lab [ The BSL Lab in Wuhan Institute of Virology]”, and when asked by the SCMP to comment on the attacks, Shi responded: “My time must be spent on more important matters”.
She has further stated…
“The novel 2019 coronavirus is nature punishing the human race for keeping uncivilized living habits. I, Shi Zhengli, swear on my life that it has nothing to do with our laboratory”
‘Punished’ for ‘uncivilized living habits’. Well Shi isn’t an elitist, is she?
Those markets with many kinds of live animals, some wild, and butcher shops and prepared food all in close quarters with terrible sanitation and terrible attention to such things as cross contamination…this has been known to be extremely dangerous for centuries.
I have been reading about epidemiologists worried about those markets being the emergence point for new pandemic strains for decades.
Ebola and AIDS are both thought to have jumped species due to people eating wild caught animals.
Here in the US, most people know you do not even let anything that touched raw meat come anywhere near cooked meat, or any raw foods. At least people who know how to keep from getting sick do.
Without specific information, speculating about COVID19 being an escaped bioweapon is just storytelling. It is not necessary to explain a new illness.
And what ever the truth is, trying to glean the truth by cobbling in together internet rumors with guesswork is worth that pointless. If you do a good enough job of spinning it in your head, you will become immune to actual info if and when it becomes available.
Typo:
…worse than pointless.
Rud, I think your conclusions may be erroneous if they are based on the earlier data coming out of China.
I get the distinct impression that the number of cases and especially the number of deaths have been deliberately played down.
Some people like the latest guy from here in the UK has infected a lot of people with close contact without him feeling ill until after he got back to the UK.
https://www.dailymail.co.uk/health/article-7986517/Number-coronavirus-cases-UK-doubles-EIGHT.html
It is of course prudent to be skeptical about the Chinese reports and data. However it’s what Rud has to work with!
Actually we are getting a sense of the viral R-Naught (how contagious it is) from cases outside of China now. It is very likely that the number of people infected far exceeds the cases identified which is why I do not think this virus can be “contained”. I just don’t think it will turn out to be much worse than a bad modern Flu virus season at worst. (Not including the Spanish Flu in this, that one was plain nasty).
We pretty much know the Chinese government, as our own, will lie through their teeth.
So what if this inadvertent release is really the true data, and its 80,000 cases and 25,000 dead, and that is from Feb 2.
Taiwan News Releases Corona Virus Deaths That Are 80 Times Higher Than Communist News Narrative
https://www.nukepro.net/2020/02/taiwan-news-releases-corona-virus.html
> “We know from the Japanese cruise ship Diamond Princess quarantine that R0 is at least ~2. (As of now, 63 diagnosed out of 2667 passengers and ~1100 crew). Since Japan has moved the 63 symptomatic patients to hospital isolation, that same cruise ship may in the next 14 days also provide an experimental symptomless Wuhan R0 estimate. Late revision update, now 69, so asymptomatic R0 is unfortunately above 1.”
With 135 now confirmed aboard the cruise ship, the Rnaught is now likely closer to 3. as you say, very concerning.
They only tested something like 300 people on that ship so far……
Exactly. The Cruise ship environment is bad, yet what China is doing may be down right murder, if reports are correct? It is shown that they are seperating anyone that MAY have been exposed to a positive case into buildings with no real medical supplies, very limited restrooms, rows of beds right next to each other, hundreds – thousands of beds. ( A 1.5 million sq foot convention center as an example)
It is certain that some of these people will be contagious although currently symptom free. These conditions make contagion almost certain.
I tend to think the worst aspects of contagion about this are likely true.
Why? Because there is no chance that China would put 70 million plus on lock down and 350 million plus in severe travel restrictions for the numbers they are reporting. Because they arrest Doctors that show anything outside the party line. Because the videos look real and not staged. Because of numerous reports from wealthy well connected Chinese business men who say it is far worse then the official numbers.
On the other hand, how typical are cruise ships?
There have been quite a few cases where other diseases have become wide spread due to the conditions on such ships.
Recently my wife and I spent 3 days at Disney World in Florida. I concluded that place is one of the germiest places on earth. I suspect a cruise ship would not be much better. I returned from that trip with a bad case of the flu that was not only a URI but also involved abdominal cramping and severe diarrhea. It’s been three weeks and I’ve still not completely recovered.
Yup. They’re like airplanes, only for days instead of hours, and with thousands rather than at most hundreds of passengers.
Cruise ships = Petri dishes for the elderly.
That said, You couldn’t get me to bet on any aspect of the spread. We know very little and have no epidemiological models upon which to rely. New Coronavirus seems to be more deadly and more transmissible and more persistent but it will take months or years to see if that is the case. We don’t even know if the virus itself is the cause of death rather than the vector weakening the system to other illnesses.
The cruise ship does not have kits to test everyone on board so are just testing symptomatic persons and their family. The quarantine is on day 4 and there are already 135 confirmed cases.
Wuhan infections and deaths are grossly underreported for the same reason, not enough test kits and not enough lab processing facilities.
Two other cruise ships are currently suspecting an outbreak but haven’t been granted docking space.
Please don’t forget cross infection is a two way street. Face masks may not be ideal for your own protection but they can help others by reducing the load of droplets exhaled by yourself. I have a small stock of soap, gloves, masks, glasses “just in case”. The health system needs a longer flatter bell curve of infection should the worst happen–bruce
Well, what doesn’t kill you makes you evolve in to a better species. I bet RNA viruses are a major driver of evolution. Maybe we should be jealous of Wuhan? 😉
I hope they finally say no to the wet markets and trading of illegal and endangered species.
“[…]there are only 4 known human [serotypes] (sic) causing about 20% of common colds, and DNA adenoviruses (about 60 human [serotypes], but including lots of non-cold symptom {serotypes} like conjunctivitis (pink eye and pharyngoconjunctivitis) causing about 5% of common colds.”
But yet there some 90 distinct Pneumococcal serotypes, and this specific coronavirus is known for its pneumonia. Fever, dry cough and shortness of breath seem to be the common symptoms followed by acute pneumonia and finally organ failure and death.
Wuhan is known for its terrible air pollution, might we have two agents working here as about 40,171 of the confirmed cases of a greater total of 40,632 are on the Chinese mainland, mainly around Wuhan. Of the 910 deaths, 908 of them are in China.The 3,323 recoveries, 3,281 in Mainland China. Meaning that 42 of the 461 cases outside of China have recovered.
So there are a full percentage point more recoveries outside China. Incidentally many cases are showing up as clusters of asymptomatic; in Germany and the Philippines.
The case for the PCR to be the finite evidence of a coronavirus infection is prone to easy contamination and prone to false-negative and positives. Contamination is at a premium as this process is both quick and cheap in its use as a decider. Using blood, sputum and swabs are inconclusive as they vary from site to site, and conclusion can only truly be attained by using Cerebral Spinal Fluid (CSF), which is rather an expensive process.
Since this virus is closely related to the SARS coronavirus — it is almost identical in its symptoms as 2019-nCoV. Now not a single case of SARS has been seen outside the laboratory since the initial outbreak which killed some 800 people in 2005.
“[…](As of now, 63 diagnosed out of 2667 passengers and ~1100 crew).”
And cruise ships are known for their old people…
“But pangolins were […]”
Strange I was looking at that line of contamination myself, what don’t Chinese people eat?
Very little. I recall a Chinese expression that is “the dog’s heart and the wolf’s lungs” (it may be the other way around). This means something which is unpalatable to say, but must be said, as there is no way to disguise it. Its meaning is based on the fact that these are the only two items whose taste cannot be disguised, and are thus never eaten. Everything else is on the menu.
The Huanan Market is known as a seafood market but, media reports say these items are for sale:
Badgers, Bats, Beavers, Camel, Chickens Civets, Crab, Crocodiles, Dogs, Donkeys, Emmental cheese, Fish, Foxes, Giant salamanders, Hedgehog, Herbs, Koalas, Marmots, Ostrich, Otters, Peacocks, Pheasants, Pig, Porcupines, Rabbit organs, Rats, Sheep, Shrimp, Spices, Spotted deer, Striped bass, Turtles, Vegetables, Venomous snakes (including Bungarus multicinctus), Wolf puppies.
And yet a report was published on January 20th, 2020 that no virus was found at that market.
“what don’t Chinese people eat?”
The North Koreans and some Chinese eat dog meat. Here’s a link to a description of prankster Joey Skaggs request by mail in 1994 to 1500 American dog shelters by a prank Korean for dogs to use in his dog meat soup. He really got a rise out of dog-lovers.
https://joeyskaggs.com/works/dog-meat-soup/
Transcript:
“Dog shelter kill million of dog, cost money…Dog shelter need money to operate. Where it get money? Hard to get money. Many people like to eat dog…Where do they get dog?…We buy all dog, regardless of size or color. We prefer big, young strong dog, but we take all dog from your dog shelter.” [Ten cents a pound]
Kim Yung Soo, President, Kea So Joo, Inc.
Ten cent?
You pay 18 cent or take a hike buddy!
And you must take cat and dog, take both.
Cat is 23 cent a pound…cat food more expensive, cat so finicky, they cost more.
Kitten and puppy you pay double for extra tender.