SARS-CoV-2 antibody serology assays developed by MD Anderson researchers accurately detect neutralizing antibodies
UNIVERSITY OF TEXAS M. D. ANDERSON CANCER CENTER

HOUSTON — Two different types of detectable antibody responses in SARS-CoV-2 (COVID-19) tell very different stories and may indicate ways to enhance public health efforts against the disease, according to researchers at The University of Texas MD Anderson Cancer Center. Antibodies to the SARS-CoV-2 spike protein receptor binding domain (S-RBD) are speculated to neutralize virus infection, while the SARS-CoV-2 nucleocapsid protein (N-protein) antibody may often only indicate exposure to the virus, not protections against reinfection.
The results, published today in JCI Insight, highlight findings from a quantitative serological enzyme-linked immunosorbent assay (ELISA) using SARS-CoV-2 S-RBD and N-protein for the detection of circulating antibodies in 138 serial serum samples from confirmed COVID-19 hospitalized patients and 464 healthy and non-COVID-19 serum samples that were collected between June 2017 and June 2020.
Results showed that 3% of healthy and non-COVID-19 samples collected during the pandemic in Houston were positive for the N-protein antibody, but only 1.6% of those had the S-RBD antibody. Of samples with the S-RBD antibody, 86% had neutralizing capacity – meaning they could prevent reinfection of COVID-19, but only 74% of samples with N-protein had neutralizing capacity. When positive for both, 96.5% exhibited neutralizing capacity.
“These findings suggest that detection of N-protein binding antibodies does not always correlate with presence of S-RBD neutralizing antibodies, and that the presence of the S-RBD antibody is the best indicator of any potential protection against reinfection,” said senior author Raghu Kalluri, M.D., Ph.D., professor and chair of Cancer Biology. “We caution against the extensive use of N-protein based serology testing for determination of potential COVID-19 immunity, and we believe that accurate and reliable S-RBD serological testing is needed to carefully identify individuals with neutralizing antibodies in order to help advance recovery efforts around the globe.”
At present, some commercially available serological tests confirm only the presence antibodies to the N-protein, with over 200 commercial and hospital laboratory testing facilities currently using these tests. While these tests indicate exposure to the virus, they do not seem to suggest immunity to reinfection. These findings reiterate the need to educate on what an antibody test result mean for each patient, and that public health efforts should focus on ways to encourage patients to continue vigilant safety precautions even with the presence of N-protein antibodies.
“In addition to serological assessment of the general population, we are hopeful these results will aid in rapid assessment of the efficacy of vaccine candidates as they are translated into the broader population,” said lead author Kathleen McAndrews, Ph.D., postdoctoral fellow in Cancer Biology.
###
Luis L. Ostrosky-Zeichner, M.D., and Ramesh Papanna, M.D., of The University of Texas Health Science Center at Houston (UT Health) McGovern Medical School, contributed some samples to the study. A full list of co-authors can be found in the paper.
About MD Anderson
The University of Texas MD Anderson Cancer Center in Houston ranks as one of the world’s most respected centers focused on cancer patient care, research, education and prevention. The institution’s sole mission is to end cancer for patients and their families around the world. MD Anderson is one of only 50 comprehensive cancer centers designated by the National Cancer Institute (NCI). MD Anderson is ranked No.1 for cancer care in U.S. News & World Report’s “Best Hospitals” survey. It has ranked as one of the nation’s top two hospitals for cancer care since the survey began in 1990, and has ranked first 16 times in the last 19 years. MD Anderson receives a cancer center support grant from the NCI of the National Institutes of Health (P30 CA016672).
…..”we believe that accurate and reliable S-RBD serological testing is needed to carefully identify individuals with neutralizing antibodies in order to help advance recovery efforts around the globe.”
The only thing that anyone in the media or the politicians care about is that a positive test of any kind gets added to the “case count” to extend the draconian measures they’ve implemented. Anyone actually think that they are going to differentiate what the test is looking at? No one has any idea of the severity of these “cases” nor is anyone looking.
Yes. It’s basically all politics and, hence, control. The school unions are pretending that student lives are at great risk. They are not and neither is this the case for the majority of teachers.
I work in Boulder county CO and not one person under the age of 50 has died and not one under the age of 20 has been hospitalized, and this is a county with a relatively young population. Where I live, the population is older and there also have been no hospitalizations for anyone under the age of 20. All but 1 of the deaths were over the age of 40. That 1 death below 70 was someone between the age of 50 and 59.
Can agree. I live in northern Florida and to date, I know of no one personally that has even tested positive for the virus much less died with or from it. Oddly enough, the ones that I do know who have died had long term illnesses like cancer and other.
54246 has an aged and impoverished population quite isolated. The local medical authorities use health information privacy ignorance to hide the lack of identified Pt with symptoms, antigen or antibodies.
I know of no person sick with CoViD.
#Resist. Do Not Comply
Amen. And again, “never let a crisis go to waste”. A meme of the far left.
And the meme of every price-gouger after any natural disaster. Unfortunately, in politics there’s no law against it.
Rahm Emanuel Chief of Staff under Obama and subsequent mayor of Chicago aka the “Rahmboss,” Is Quoted as saying “you never want a serious crisis to go to waste.” Which is why the Propaganda Media keeps falling all over themselves to provide the Democrats with one faux crisis after another. Sad how their crisis actions always makes everyones life worse than before the “Cirsis” Its called the Law of Unintended Consequences. The left calls it Democratic Socialism.
The general population probably doesn’t need a vaccine. It would be good to protect those at high risk, however.
https://thefatemperor.com/ep91-emeritus-professor-of-immunology-reveals-crucial-viral-immunity-reality/
In the meantime, it seems that control is slipping away from darlings like S. Korea. Previous exposure to other corona viruses has more to do with their low death rates than anything their government did.
Scissor wrote, “[in] S. Korea. Previous exposure to other corona viruses has more to do with their low death rates than anything their government did.”
Utter nonsense! South Korea’s death rate is low because their case rate is low, and their case rate is low because they work very hard to quickly identify and quarantine everyone who has the disease, even before they develop symptoms.
South Korea: 15,318 known cases and 305 deaths from a population of 51.3 million
Italy: 253,915 known cases and 35,396 deaths from a population of 60.4 million
Sweden: 84,294 known cases and 5,783 deaths from a population of 10.1 million
USA: 5,564,938 known cases and 173,074 deaths from a population of 331 million
Fatality ratio, Italy / S. Korea:
(35,396 / 60.4) / (305 / 51.3) = 98.6 times higher for Italy
Fatality ratio, Sweden / S.Korea:
(5,783 / 10.1) / (305 / 51.3) = 96.3 times higher for Sweden
Fatality ratio, USA / S.Korea:
(173,074 / 331) / (305 / 51.3) = 87.9 times higher for USA
The United States is doing almost as badly as Italy and Sweden. Americans are 87.9 times as likely to die from coronavirus than are South Koreans, even though the epidemic got a head start in South Korea.
Anyone who doesn’t think the United States should be trying to emulate the success of South Korea, by emulating the strategy of South Korea, is an absolute idiot.
Until & unless an effective vaccine (or other preventive) is developed and widely deployed, there is one and only one way to stop the epidemic: identify everyone who has the disease, including those with no symptoms, and quarantine them until they are no longer contagious. That requires widespread testing, with rapid result reporting, and fast, efficient contact tracing.
Here’s one more statistic:
Known case rate ratio, USA / S.Korea:
(5,564,938 / 331) / (15,318 / 51.3) = 56.3 times higher for USA
In other words, although the per-capita fatality rate is 87.9 times higher in the USA, the per-capita known case rate is only 56.3 times higher in the USA. That means the number of deaths per thousand cases is much higher in the USA than in S. Korea, even though most of S. Korea’s cases occurred early in the pandemic, when treatment protocols were presumably less effective.
That strongly suggests that at least 36% of U.S. cases, so far, have gone undetected. And that is why the disease is out of control, in the United States: because we are not quickly and efficiently identifying and quarantining people who have the disease.
Near here we had a plumber who felt ill, and got tested. But due mostly to state bureaucratic delays, he wasn’t told that he was infected for a full week — and in that week he infected over a dozen households.
That could never have happened in South Korea. In South Korea that plumber would have had his test results in mere hours, and within a few more hours most of his likely contacts would have been notified to self-isolate, and get tested.
That plumber, and the people he infected, are what catastrophic, IPCC-level incompetence looks like, at a local level. In fact, NC state officials are actively making the epidemic worse, by restricting the medical personnel who may administer the tests, by unnecessarily delaying testing, and by restricting & delaying the reporting of test results.
It makes me sad to have to admit that the South Koreans certainly appear to be much smarter than my fellow Americans.
Or people get the Covid and get over it…much less intrusive
With survival rate better than 99 %. I be with you. Avoid the flu shot, take D3 with K.
Mere survival isn’t everything. Many COVID-19 patients apparently have lasting health issues, either pulmonary, or neurological, or both. It is better to avoid contracting the disease, altogether, if you can.
Apparently they have lasting 😉
It’s not nonsense. Cross reactivity immunity is becoming ever more obvious. Since many corona viruses originate in Asia, and China specifically, the incidence of immunity is higher in Asia. It is easier to control an outbreak when a higher fraction of the population are immune, however, there is no question that SARS-CoV-19 is highly infectious.
S. Korea has been effective in isolating outbreaks, but they are at risk of losing control as evidenced by new infections recorded in the past several days: Aug 10 – Aug 16 case numbers, 28, 34, 54, 56, 103, 166, 279, respectively.
Larger, more populated countries with greater numbers of international ports and transportation hubs are simply more difficult to isolate and protect. Once an outbreak gains foothold, it’s very difficult to regain control.
Here are links to articles regarding cross reactive immunity.
https://pubmed.ncbi.nlm.nih.gov/32668444/
https://www.nature.com/articles/s41577-020-0389-z
https://science.sciencemag.org/content/early/2020/08/04/science.abd3871
The only question is “why don’t we do this every time there’s an outbreak of flu”? There has been an attitude shift here – one of abject fear and panic. This is not good.
“known cases” are not measuring the same thing in each country. So your entire analysis is useless.
Go hide under your bed. Us grownups have work to get done and lives to lead.
The key is identifying and isolating patients who have the disease and treating them with whatever protocol they and their doctor agree on. Most people won’t get very sick. Older people may, but intensive treatment can allow many of them to recover. Dumping sick people into nursing homes to affect the residents and letting older people die due to a simple lack of care is a crime.
The USA “LOCKDOWN” policies have been pretty much a complete failure. Isolating people without the infection prevents most of them from getting any significant exposure and hence immunity. Lockdowns simply don’t work to prevent infection. eventually many will get sick. The lockdown policy was a short term idea to prevent hospitals from getting overloaded. That part worked so well that the lockdowns should have been gradually ended starting around the end of last April.
Do we have any vaccines for any Coronaviruses ?
Thanks
Just for a couple of canine and equine diseases.
Are we talking about 1.6% of the 3% or 1.6% of the samples. I’m presuming the latter but the way that it’s written leaves me uncertain.
Who cares what these tests are or how they perform, as there is no way that they are specific for C-19 because NO ONE has a pure culture of this virus. The spike proteins are common to other covis and thus it is patently nonspecific. The same is true for the PCR test. Not only is PCR not fit for purpose, it detects RNA that is not specific for C-19, again because no one has a pure culture and thus it cannot be specific. Both types of tests are probable 80 or more false positives, but the brains running this scam have told the public that all these false positives are virus carriers. A complete lie and the public is clueless.
Typhoid Mary is famous for being one of the few true asymptomatic carriers in history.
Here we go again 300,000 mainly old people die with co-morbities die every day in the world or 60,000,000 per anumm ITS NORMAL! Why don’t we have quarantine for Influenza or flu which kills much more and younger people? So far this coronavirus which is just a cold virus like all the others which has killed about 700,000 old people already dying over 7 months!!! Make your calculations Mosh and Jo anne nova, They are now killing millions with stupid lock downs. Look at Sweden NO MORE DEATHS while the rest of the world on lockdowns is just prolonging the virus because it cannot be allowed to immunize the young and middle aged and healthy older people. The pain from unemployment, depression suicide, economy! We take note that Mockton has dissapperaed from any site. Time that Jo nova STOP pushing the lockdowns. otherwise the Australian will blame her for countless deaths not due to coronavirus and want her scalp (joke) otherwise her climate stuff is fine cheers.
I used to rather admire Jo Nova, but she has fallen into the same series of fallacies that she condemns in Climate Alarmists.
– Predictions based on failed models and assumptions proven false by observation.
– Advocacy of simplistic solutions to complex problems.
– Disregard for cost-benefit analysis and sustainability of proposed solutions.
– Dependence on Authoritarian, One-Size-Fits-All solutions.
– Villification of dissenters
Show examples of “Villification of dissenters”, all I have seen disagreement with your views.
You can’t do a cost benefit analysis because you have to put a value on a life of what is left of an elderly persons life and no two people will agree.
At the end of the day Australia is a democracy and lockdowns have majority support (its running at about 83%). Personally I have little problem we are trampling all over what you believe in the same way I have little problem trampling all over what Loydo or some ecowarrior believes and wants.
I do not agree that democracy can be measured simply by how many people go along with something. Surely if it means anything at all, it means individual liberty, otherwise you slip into repression of minorities, which is exactly what is happening here. The majority are effectively calling for the repression of the minority – those who wish to go about there (formerly) lawful business. Not difficult to see where this leads.
Minority views are always repressed in a democratic process that is why to counter the effect US has a bill of rights. Many democracies like Australia have no bill of rights and yes the majority effectively represses minorities. There is a bit of humor on that front in Australia we have had referendums about having a bill of rights and last attempt it lost getting only 31% support. The majority don’t want to face endless lawsuits from the minorities about their rights being trampled. I can’t see Australia will ever have a bill of rights as there is nothing to gain in it by the majority.
Eliza wrote, “Look at Sweden NO MORE DEATHS…”
Sweden has reported 21 deaths so far this month. Total to date: 84,294 known cases and 5,783 deaths from a population of only 10.1 million. That per-capita fatality rate is even worse than the United States.
South Korea has reported 4 deaths so far this month. Total to date: 15,318 known cases and 305 deaths from a population of 51.3 million.
Per-capita fatality ratio, Sweden / S.Korea:
(5,783 / 10.1) / (305 / 51.3) = 96.3 times worse for Sweden
Now, really, which country do you think the rest of the world should emulate?
Eliza wrote, “…this coronavirus which is just a cold virus like all the others…”
Has anyone ever heard of a cold virus with a ≥2% fatality rate?
Has anyone ever heard of a cold virus that killed 173,000 Americans?
Eliza wrote, “Why don’t we have quarantine for Influenza or flu which kills much more and younger people?
An average flu season kills fewer than 40,000 Americans. Here are the statistics:
https://sealevel.info/CDC_Influenza_stats_Table1_2010-11_thru_2018-19_as_of_2020-04-04.html
(Partly that is because, in an average year, nearly half of the U.S. population gets the flu vaccine, disproportionately those most at risk from it; unfortunately, we don’t have a vaccine for COVID-19.)
COVID-19 has killed over 173,000 Americans, so far, even though it has infected nowhere near as many Americans as the flu does in a typical year.
“Sweden has reported 21 deaths so far this month. Total to date: 84,294 known cases and 5,783 deaths from a population of only 10.1 million. That per-capita fatality rate is even worse than the United States.” The problem with this statement, Sweden death per million is not going to change much, he it will only grow, and how long God only knows. Presently Sweden deaths per million is a 572 the US is at 532, somehow the price we paid in extra death due to the lock-down will make Sweden look real good. Deaths per million due to COVID-19 and the lockdown here will make Sweden deaths per million far lower than the US. Delay health care, isolation and keeping kid out of school is a recipe for disaster. Wake up snowflakes.
You probably need to elaborate, Swedens economy is just as trashed as the US and as you say the rates are the same. So at best the Swedish had a few more personal freedoms with the same result.
And yet mainly old people or people with co-morbidities died. Sad, but we survived. Let’s move on.
Dave burton, the official covid death count in USA is overstated… it lumps “died from covid”, “died with covid but actually died from something else”, and “died with covid-like symptoms but were never tested for covid” all into the same group. Blame the CDC and orange-man-bad disease, among other reasons such as quest for power and greed $$$$.
goracle wrote, “the official covid death count in USA is overstated… it lumps “died from covid”, “died with covid but actually died from something else”, and “died with covid-like symptoms but were never tested for covid” all into the same group.”
That’s backward, goracle. The official death count in USA from COVID-19 is understated, because millions of COVID-19 cases in the USA are never diagnosed, and when COVID-19 kills someone before it is diagnosed, the cause is often mistaken for something else.
As you point out, the opposite can also happen: deaths due to other causes can be misattributed to COVID-19, but that is less common.
“Died with COVID from something else” is not very common, and when it happens it is rarely misdiagnosed as “died from COVID.” If you’re murdered, or die in an automobile accident, or drown, etc., nobody will check your body for COVID-19, and even if you were known to have had COVID-19 your death usually won’t be blamed on it. Deaths with no apparent cause are unusual, and deaths for which the cause is apparent are not usually autopsied.
For example, we know that George Floyd was recovering from COVID-19, and almost certainly suffering neurological problems because of it, when he was murdered. But, even though it is likely that the effects of COVID-19 contributed to the circumstances which ended in his death, his death is not blamed on COVID-19.
However, deaths due to COVID-19 have often been misdiagnosed as something else, because millions of COVID-19 cases in the United States have apparently gone undiagnosed. If someone with a known, life-threatening health problem dies at home, that known health problem is almost certain to be listed as the cause of death, even if the real cause was COVID-19, simply because there was no COVID-19 diagnosis before he died, and after he died there was no autopsy.
You probably won’t believe me unless we do the math. So let’s do the math.
On an average day, when there’s no epidemic, 7000-8000 Americans die of all causes. If 1.5% of the American population is infected with COVID-19 right now (a reasonable estimate), then you would expect that roughly 1.5% of the people who die today from other causes are coincidentally also infected with COVID-19 at time of death.
1.5% of 7500 is about 112.5. But that includes deaths by automobile accident, suicide, murder, fire, drowning, heart attack, stroke, cancer, etc., none of which would ever be attributed to COVID-19. In fact, in the great majority of deaths a likely cause of death is apparent, and few of those cases would be tested for COVID-19.
But let’s suppose, for the sake of argument, that 20% of those 112.5 deaths were mistakenly attributed to COVID-19. That’s probably way too high, but let’s see what it would imply.
20% of 112.5 would mean 23 misdiagnoses.
Now, compare that to the total COVID-19 death rate. In the first 14 days of August, the United States averaged 1047 deaths per day attributed to COVID-19. If 23 of them were misdiagnoses that would be a 23/1047 = 2.2% error.
So, even though a few of the approx. 1000 deaths/day in the United States attributed to COVID-19 might have erroneously attributed, it cannot have been enough to appreciably affect the statistics.
“The official death count in USA from COVID-19 is understated, because millions of COVID-19 cases in the USA are never diagnosed, and when COVID-19 kills someone before it is diagnosed, the cause is often mistaken for something else.”
Complete BS you cannot support with evidence.
Dave, I believe you’re wrong. There are very few people dieing at home from covid. They’re going to the hospital because they can’t breathe or have an out of control fever. With all the news and fear being spread about the seriousness of this virus, there will be very few who not seek help with these symptoms. On the other hand, with all the cancer treatments being skipped and people not going to the hospital because they feel a chest pain or are feel tired and lightheaded (maybe due to their blood sugar levels, for example), there are people dying at home that likely would not have because they’re afraid to go to the hospital to seek help because they don’t want to catch covid.
BTW, I know of 1 personal example where they tried to attribute covid as the cause of death for a 68 year old mom in an auto accident because the @45 year old son (who live a couple of cities over) had covid (he did not die) but there are a number of examples you can search for online that show this. The son complained. They never even tested her. I don’t know what the official cause of death on the certificate is but the point is they tried to attribute covid as the cause of death when it clearly wasn’t. There are a number of stories online you can search for along the same vein as this. On the other hand, I haven’t read a story yet of someone dieing of covid but it being attributed to something else (doesn’t mean it doesn’t happen, I just have not come upon such a story and I believe the media would love to post these stories everywhere).
I have no idea what your 1.5% example means. You state 8,000 people die everyday in USA and that 1.5% of them currently have covid (112). If this is the case, how can you then say that covid kills 1,000 per day in august? That’s off by a factor of 10.
goracle wrote, “I have no idea what your 1.5% example means. You state 8,000 people die everyday in USA and that 1.5% of them currently have covid (112). If this is the case, how can you then say that covid kills 1,000 per day in august? That’s off by a factor of 10.”
It’s not “off by a factor of 10,” it’s two different numbers.
That’s the point: the number of possible misattributions, in which someone dies with COVID-19, but from a different cause, and the death is erroneously blamed on COVID-19, is tiny, compared to the total number of COVID-19 cases. That means the number of COVID-19 deaths cannot possibly be significantly exaggerated.
I wrote, “On an average day, when there’s no epidemic, 7000-8000 Americans die of all causes.”
If 1.5% of the entire American population is infected with COVID-19 right now (a reasonable estimate), then you would expect that roughly the same percentage of the 7000-8000 people who die today from other causes are also infected with COVID-19. Agreed?
That would be only about 112 people, most of whom would NOT be misattributed to COVID-19, because their actual cause of death was apparent.
But over the first two weeks of August, the U.S. averaged 1047 deaths per day attributed to COVID-19. Obviously the vast majority of those cannot have been misattributions.
Some people are claiming that the number of deaths attributed to COVID-19 is greatly exaggerated, by cases of people dying with COVID-19, whose death had a different cause. As you can see, they are wrong.
However, we have very good reason to believe that many people who have died at home from COVID-19 have had their cause of death listed as something else. Here’s an article:
https://gothamist.com/news/surge-number-new-yorkers-dying-home-officials-suspect-undercount-covid-19-related-deaths
dave, i believe you’re wrong. next to no one is dying at home from covid… if you can’t breathe or have an out of control fever, the first place you’re going is the hospital, especially with all the fear mongering – almost no one is staying home if they have these symptoms. on the other hand, if your chest hurts or you missed your cancer treatment or your feeling tired/light-headed (maybe due to low blood sugar, for example), you may opt to stay home and not go to the hospital because they’ve scared you from going to the hospital because you might get covid.
As for the 1.5% example, I’m totally confused. You state the @ 8K americans die daily and that 1.5% of those have covid (@112 people per day) but you then state that covid kills 1000 people per day. that’s off by a factor of 10.
Dave burton, how do you know that covid has not infected nowhere near as many people as the flu/pneumonia annually in USA? Has everyone been tested for covid to confirm your statement? Do we test everyone every year for the flu/pneumonia to see how many get infected?
goracle asked, “Dave burton, how do you know that covid has not infected nowhere near as many people as the flu/pneumonia annually in USA?”
The CDC estimates that in an average year, almost 29 million Americans have symptomatic illness from seasonal flu. Here are the statistics:
https://sealevel.info/CDC_Influenza_stats_Table1_2010-11_thru_2018-19_as_of_2020-04-04.html
Thus far we’ve had 5,566,632 known cases of COVID-19 in the United States. So, the question is, how many additional (undiagnosed) cases have there been?
We don’t know that precisely, but we estimate it, and calculate reasonable error bounds. By comparing U.S. statistics with countries like South Korea, which have identified nearly all their COVID-19 cases, we can deduce that at least 36% of America’s COVID-19 cases have gone undiagnosed.
That’s the low end. For the high end of our plausible range. We can also deduce that it cannot be that more than about 60% of cases have gone undiagnosed, because, otherwise, that would mean we’ve somehow achieved a dramatically lower fatality rate than South Korea, despite most of our patients never being diagnosed or treated. That’s obviously implausible.
So, it is fair to assume that somewhere between 36% and 60% of our cases have gone undiagnosed. That means the real number of cases is between (5,566,632 / (1-0.36)) = 8.7 million and (5,566,632 / (1-0.60)) = 13.9 million.
Even the high end of that range is only about half the typical number of symptomatic seasonal flu cases in the United States.
Death counts keep falling. If we take care of at risk people we will survive. Case counts….yawn.
Dave, S Korea has only tested @ 1.5million people of 50 million (3% of poplation) whereas the USA has tested @70 million (20% of population). Most of their population has not been tested so you cannot state that they’ve identified most covid cases.
The CDC stated nearly 2 months ago that there were @ 10 undiagnosed covid cases for every diagnosed case (that’s nearly 1000%, not 36-60%). At the time, that would translate to @ 25 million covid cases… since then, I’m fairly certain the infection has spread and there are @ 50 million infections as of now (most undiagnosed). The bottom line is Covid is not nearly as serious as we were initially and currently being told. The death rate is much closer to pneumonia (.1%) than 3% (deaths/confirmed cases).
Derg wrote, “Death counts keep falling… Case counts….yawn.”
Mere survival isn’t everything. Many COVID-19 patients apparently have lasting health issues, either pulmonary, or neurological, or both. It is better to avoid contracting the disease, altogether, if you can.
goracle wrote, “S Korea has only tested @ 1.5million people… Most of their population has not been tested so you cannot state that they’ve identified most covid cases.”
Sure we can. There’s no need to test people who’ve not been exposed to the disease. That’s why they do contact-tracing: so that they can find everyone with the disease, without bothering to test those who’ve not been exposed to it.
We know they’ve found the vast majority of their cases because they largely stopped the spread of the disease (though a few cases obviously escaped detection, because there’s been a modest disease resurgence lately).
goracle wrote, “The CDC stated nearly 2 months ago that there were @ 10 undiagnosed covid cases for every diagnosed case…”
That was Redfield’s June 25 press briefing. It was an estimate based on antibody testing, which might have been distorted by sample bias, or by false positives, perhaps due to patients having antibodies to other coronaviruses.
Here’s how we can know that it was not correct. If it was correct, then it would mean our true fatality rate is a small fraction of the fatality rate in South Korea, and their fatality rate is known quite precisely, because they’ve identified nearly everyone who contracted the disease, and because the great majority of their cases are resolved:
South Korea
Cases: 15,515
Deaths: 305
Recovered: 13,917
Active: 1,103
Resolved = Deaths + Recovered = 305 + 13,917 = 14,222
Deaths / Resolved = 305 / 14,222 = 2.14%
Deaths / Cases = 305 / 15,515 = 1.97%
So, the upper bound on their true fatality rate is 2.14%.
The lower bound is 1.97%.
(The uncertainty is because we don’t yet know the outcomes of the active cases.)
If we’d really had 25 million COVID-19 cases in the U.S. (almost as many as the number of flu cases in a typical season), that would make our fatality rate:
173,187 / 25,000,000 = 0.69%
That’s only 1/3 of South Korea’s fatality rate.
If we’d really had 50 million cases, that would make our fatality rate:
173,187 / 50,000,000 = 0.35%
That’s only 1/6 of South Korea’s fatality rate.
Because South Korea’s case spike occurred very early (4.5 months ago), when the medical community had little experience treating the disease, it is plausible that their fatality rate could be substantially higher than ours. But six times higher? That seems unlikely. Doctors have gotten better at treating this disease, but not that much better. Here are a couple of articles about it:
https://www.healthline.com/health-news/covid-19-mortality-is-going-down-in-icus-what-this-means-for-the-pandemic#The-mortality-rate-is-dropping,-but-its-still-high
https://www.bbc.com/news/health-53192532
Here’s a recent CDC article, about COVID-19 fatality rates:
https://www.who.int/news-room/commentaries/detail/estimating-mortality-from-covid-19
Excerpt:
“…with estimates of IFR converging at approximately 0.5 – 1%”
That’s lower than South Korea’s 2% fatality rate, but consistent with a trend toward lower fatality rates as the medical community gains experience with the disease.
However, there is good evidence that the disease began spreading in the United States well before it was recognized, initially masked by the larger number of flu cases. Here’s an article from a few days ago:
https://www.houstonchronicle.com/news/houston-texas/houston/article/UT-study-Thousands-of-early-COVID-19-cases-in-15479738.php
Mere survival rates;)
This thing is moving on. Covid is old news. Not scary anymore.
dave, your 1.5% example is overly confusing and the mental gymnastics required to try to make any sense from it is even worse. you make quite a bit of assumptions (we all do at some point because we all have different perspectives).
no one has an accurate idea of the actual covid deaths because they’ve muddied the waters by including “died with covid” and “died with covid-like symptoms but no test”. the fact you’re even trying to defend this hogwash non-science makes your nicely worded arguments less effective. we’ll need to wait till the excess death numbers are in to see how bad covid was because at this point we’re all just speaking past each other and only looking at numbers that prove our point.
How to explain the fact that Thailand reports .8 deaths per million population versus 6 per million for S. Korea?
There is a sharp rise in unexplained deaths … you can’t attribute what you don’t test for 🙂
They then went into hard lockdowns with extreme quarantine measures and contact tracing.
The likely rate is probably similar to South Korea as they have done many of the same things.
Dave burton, you stated “Many COVID-19 patients apparently have lasting health issues, either pulmonary, or neurological, or both.” What’s your definition of long lasting? This virus is new this year.
Additionally, you completely disregard that S Korea has only tested @ 1.5million people of their 50 million (3% of their population) whereas the USA has tested @70 million (20% of population). Most covid cases are asymptomatic and people never knew they had it. And contact tracing is fool-proof and 100% guaranteed to catch EVERYONE? Since most of S Korea population has not been tested, how would they know how many people were actually infected? It’s all an estimate based on you cannot state that they’ve identified most covid cases – your statement is totally inaccurate and so is your reasoning regarding the contact tracing.
Is reinfection an established possibility? I personally find it hard to believe over shorter time periods like a year or two. There evidently are a lot of “long haulers” that never seem to shake it in the first place. A lot of noise in all this.
I would like to know what pharmaceuticals the so-called long haulers were treated with. SARS patients had lingering abnormalities as well, which were most likely caused by treatments received, i.e., ribavirin (antiviral), high dose corticosteroids and mechanical ventilation.
New Zealand has decided to become a dictartorship for a nothing burger virus my god
I think the chinese communist party deserves to run the world they seem to be much more stable than the USA from what I am seeing to date https://www.youtube.com/watch?v=J0xxIlRbN90 AW you may want to not allow this posting unfortunately this is whats happening I am 100% pro USA but the chinese seem to be more sensible look at the BLM green deal ect? but I may prefer that you do not post this its for your eyes only
I suppose they could wait for a vaccine but at some point they will have to open their economy.
The approach should be protect the elderly and those who are at risk. Allow the healthy to pursue happiness. Forcing them into bankruptcy is wrong.
Sorry, no vaccine will be workable as you cannot make an effective vaccine against a rapidly mutating RNA virus. It is not for lack of trying. It is those seeking to make a fortune and gain power who are telling the public that they can whip up a vaccine in just a few months, while all others have failed for 30 years. Wow.
The only vaccine strategy that could “work” is unacceptable but it will undoubtedly be pushed by Gates and Fauci. They want to do gene therapy on everyone, introducing virus RNA or DNA hoping that we make the protein ourselves and then make antibodies against it.
However, our cell systems tag our extracellular proteins and there is a great probability that we will tag these as well and there will be no effect and who knows what the protein can or will do (is it even the right protein?).
Meanwhile, who knows what else is in the vaccine that Gates approves, him being the man who says we can decrease the world’s population by 15% if we do vaccines properly. How does that works? No vaccine for me!!!!!!
Quite.
Modern medicine is advancing in spite of ourselves. Certainly, mutations make the challenges more difficult, but besides strides being made in vaccines, other approaches like those highlighted by William Astley in these replies will be helpful.
I have not heard an explanation from Gates or anyone else on what he meant. It could be something related to reducing death rates from disease, like improved economic opportunity, reduces birth rates.
I take it from this report that neutralizing antibodies to viral N protein (at about 3/4 here) doesn’t ALWAYS correlate with potential immunity to reinfection and that neutralizing antibodies to viral S protein (at about 7/8 here) doesn’t ALWAYS either (as they didn’t bother to also conclude), but the combination of both may likely be pretty fully reliable for that purpose. And if a 1.6 % presence and double that were respectively positive in the “control” serums (from those deemed free of preceding Covid19 infection), this may be a measure of immunologic response to other coronaviruses such as those that cause about 1/3 of common colds.
Now the question is “in order to help advance recovery efforts around the globe”: Will the presence of either type of antibody really be a quite adequate enhancement to a community’s ‘herd immunity’ at this stage to sufficiently suppress their remaining susceptibility to ready contagion. And would administering ‘immune serum’ therapeutically provide valuable protection to the most vulnerable.
Herd immunity is appearing at low infection levels. The first 20 minutes of this video, run at 1.25 x is quite good at explaining this.
https://thefatemperor.com/ep91-emeritus-professor-of-immunology-reveals-crucial-viral-immunity-reality/
That’s wrong. That guy claims that 70% of the population is already immune, or at least partially immune, due to previous exposure to similar coronaviruses. That’s obviously untrue. If it were true, then older people would be least affected by the disease, because they’ve had the most exposure to other coronaviruses, and young children would be most affected, because few of them have had previous exposure to similar diseases.
Of course, everyone knows that that’s the exact opposite of what is happening with this disease. Most children recover nicely from it, but it runs through nursing homes like a scythe through wheat.
There’s no such thing as “herd immunity” when only 1.6% or 3% of the population have antibodies. Herd immunity only happens when a large majority of the population are immune, so that most people with the disease do not have the opportunity to pass it on to anyone else.
For a highly contagious disease like COVID-19, herd immunity would require at least 90% of the population to be immune. Here are herd immunity thresholds for several other infectious diseases:
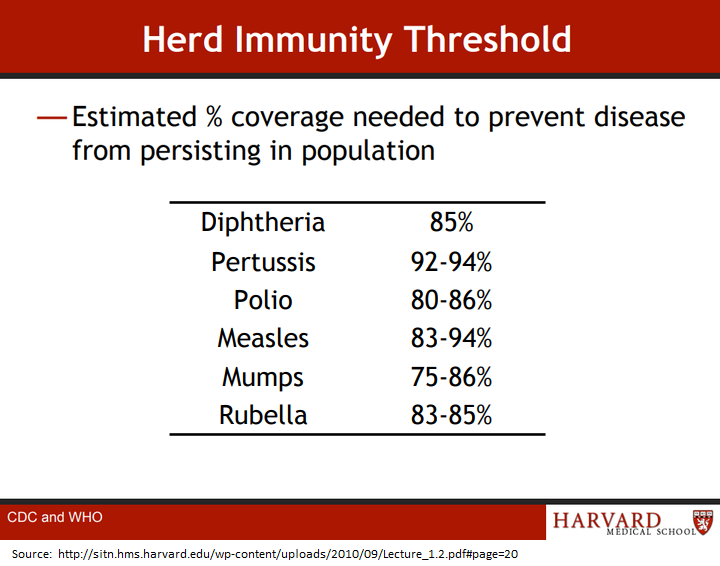
Source:
http://sitn.hms.harvard.edu/wp-content/uploads/2010/09/Lecture_1.2.pdf#page=20
Dave.
If you had bothered to listen to that interview and the many others posted on that site, you would not so easily reveal your ignorance.
1. The problem with aged people is not lack of exposure to corona-type virus’ but compromised immune systems. Age itself is a factor in declining immune-system effectiveness, but so are the comorbidities that come with increasing age.
2. The immune system functions on several levels, only one of which is addressed by current antibody tests. Those exposed to the virus and whose immune systems defeat it at those alternate levels are immune, yet do not show up on current tests.
3. Even under ideal conditions, the majority of the population exposed have not become sick. This IS pre-existing immunity, regardless of whether they test positive for antibodies or not.
Try paying attention next time. No wonder the learned gentleman called you an “Immunity Denier”
PeterW wrote, “The immune system functions on several levels, only one of which is addressed by current antibody tests. Those exposed to the virus and whose immune systems defeat it at those alternate levels are immune, yet do not show up on current tests.”
You’re just making stuff up. This is a heavily studied topic. There is no basis for a belief in “alternate levels” of immune system, which can defeat a COVID infection and leave a person immune, without triggering a conventional immune response.
Here’s a review of the antibody tests:
https://www.cochrane.org/CD013652/INFECTN_what-diagnostic-accuracy-antibody-tests-detection-infection-covid-19-virus
Dave, what then provides children a much lower incidence of contracting covid-19 as compared to adults?
As the children of today become adults; and assuming the covid-19 virus is still not completely eradicated, will such people become just as susceptible to the virus as the adults of today? — or not? — and what is the underlying physiological explanation?
noaaprogrammer,
https://youtu.be/8eDYVtPwWiM?t=43
Dave Burton at birth a baby is protected by its mother’s antibodies. Once this has worn off the infants innate immune system is the only immune system in play. As the child grows the adaptive immune system slowly becoming predominant during the school age years. This is from a paediatrician here in the U.K.
It is thought that up to 95% of our immune response is from the primitive innate immune system, the one we share with insects and other invertebrates.
Mr. Burton your argument lacks understanding of the immune system and how it changes with aging. From attack by new antigens, it’s supposedly strongest at puberty. Previous exposure and exposure to related antigens is helpful to one’s ability to fight off infections.
Your arguments on herd immunity follow Neil Ferguson’s thinking. Such as he are terribly incorrect. Read a few of the new studies regarding how CV-19 herd immunity is reached at lower levels than classical theory would suggest. There are a couple of hypotheses of merit and these each may contribute, but cross reactive immunity appears to be the correct answer.
Reach Joel O’Bryan’s very good explanation below, which covers a lot of relevant material.
People need to understand viral immunity to a specific pathogen is not a binary, True- False. Like everything in nature, levels of immunity are much more complicated than that, both in individuals and in populations. Neutralizing antibodies are but just one part of the protective immune response to a viral pathogen.
Speaking in broadly general terms, the highest level of viral immunity would be “sterilizing immunity.” Many pathogens though, like HIV, Hepatitis B and C, and the Herpes viruses (and a few viruses that most of us have for a life-time that most people in the general public have never heard of), have evolved immune evasion strategies that prevents the host, even with a healthy immune system, from developing “sterilizing immunity.”
SARS-Cov-2 virus though is not one of these persistent (or chronic) viruses. It is an acute infecting virus. The vast majority of people with a healthy immune system who are infected clear the virus with sterilizing immunity. Those who don’t die usually within 3-4 weeks. If the person’s immune system fails to clear this SARS-2 virus, i.e. sterilize the body of it, the ongoing cycles of viremia leads to severe lung pathology, then more aggressive immune system responses in a vicious cycle that then also adds to collateral damage of the airway epithelium, and they die. Period.
Sterilizing immunity is what one has immediately after the pathogen is cleared. This is “By definition” as evidenced by your body “sterilized” itself of the pathogen. The PCR tests for viral nucleic acids sequences comes back negative. You immune system could “sterilize” again if immediately re-exposed or continually exposed, say as a recovered health care worker in an influenza ward working with the sick. They can then work freely around sick patients knowing their “sterilizing immunity” is protecting them. It can last for a month it can last for years, but most assuredly it wanes. But immunity can be boosted again the next flu season with another live or attenuated virus inoculation. This is also the reason for booster shots to most vaccinations.
An example of a very long-lived IgG antibody response is the tetanus shot. The tetanus-toxoid (TT) vaccine induced IgG antibodies are very well studied by immunology. The tetanus toxoid is a protein molecule that is highly immunogenic for B-cell recognition in humans and creation of plasma cells that crank out TT-binding antibodies at protective level for 10-20 years in most people. But even that still wanes. But B-cells can only undergo variable region hypermutation and class-switch recombination in lymph nodes with CD4 T cell help. CD4 Tcells are thus vital components of the immune response to make IgG, because CD4 Tcells can then also directly help kill infected cells with cytotoxic response upon recognition using their own T cell receptor (TCR).
Because T cells are definitively and directly involved in B-cell/IgG antibody production, the host then also will develop some levels of T -cell immunity, regardless of what the B-cells do and and how fast the plasma cells die and protective levels of IgG then wanes with time.
With the CD4 T cells, they also divide and expand in numbers, but not all have the same levels of differentiation and development of “effector” tools. T cells, especially T cells, have avery diverse array of differentiation and development paths they can take. In most infections, especially acute infections, CD4 T cells produce a small population of long-lived CD4 T cell memory cells that persist for years to decades, ready to more quickly respond if the pathogen infects the host once again.
Because the molecular recognition of the pathogen is accomplished by snippets of amino acids (aa) string up to 15 aa long, these form unique recognition keys within closely related virus families for T cell’s TCR to recognize by this pool of T cell immunity that persists long after the plasma cell -derived IgG levels are gone. That is point the host would have “protective immunity” but not sterilizing immunity. The host could become infected, even experience mild symptoms, but the anamnestic response is there to more rapidly respond upon re-infection. So while the infected person my shed some virus and (importantly for control) still pass it on to new hosts, they are protected from severe disease by their long-lived T cell memory and its ability to quickly response. This is likely what is happening in 20%- 50% of the population, because T-cell memory is cross reactive to other common cold corona viruses and it is providing protective (but not sterilizing) immunity. With this protective immunity, it may be asymptomatic, but the person may still be shedding infectious virus for a short period of time able to pass it on to other people.
Bottom-line, there is a broad spectrum of immunity that will be present in the population as the epidemic progresses. Sterilizing immunity, protective immunity, minimally protective immunity, to completely naive and every gradation in-between can be found. And because viruses are intracellular parasites that hijack a cell’s molecular machinery to replicate itself, B and T cells must work together to clear virus infections.
Simply measuring antibodies to specific viral protein gives an incomplete picture of the immune status on an individual.
The posts which you have put up on this and other threads explaining the immunology are brilliant. Thank you for taking the time and for putting things in terms which non specialists can understand.
Thank you Joel. That was very informative.
Thanks for the post, Joel. People clearly must develop “Levels of immunity” over time, according to their exposure. Interesting that tests of homeless shelters, prison systems and meatpackers suggests that between 80 and 90% of individuals who are positive for COVID are asymptomatic. Doesn’t this mean herd immunity is happening?
WRT
I’m not clear what this means.
All of the dense populations above were diagnosed by (~ $100-a-pop) RT-PCR tests which are reading positives for asymptomatic and recovered cases weeks and months after the virus has been “cleared”. According to the MedCram video below, this is because “fragments” of the virus remain in the blood.
https://www.youtube.com/watch?v=h7Sv_pS8MgQ
I wondered if you would comment on what this means for our current testing in the U.S. The video, especially segment starting at around 3 minutes, suggests that “gold standard” PCR tests might be misleading both public and health officials as a predictive or screening tool because they give these positive results for people who are no longer infectious (Infectiousness stops after about 2 weeks with the disease) AND because they take days and now weeks to get results. A different kind of test, says the blog guest, is needed – a self-administered spit test which can be manufactured in large numbers cheaply. It delivers results within 15 minutes and it costs about $1.
Such test gained CDC approval over the weekend to smooth the path for the NBA season.
A better option for those who have weaken immune systems may be the new technology, artificially manufactured antibodies.
Artificially produced optimize antibodies, is the same technology that was used to defeat the deadly Ebola virus.
Those infected with covid will get a single injection of an artificial antibody, as soon as possible in the virus’s progression and they will be almost virus free in 48 hours. If the treatment is done early, as soon as covid is detected damage will be limited.
Regeneron, the leading company in the new field has received $500 million dollars from the US and have moved onto Phase 3 trials of their new artificial antibody.
This is an artificial antibody, not a vaccine.
The injection would provide the person injected, with roughly 4 weeks of immunity to covid.
There are two other antibody designing companies that are working the with the US Military to develop a covid antibody.
https://investor.regeneron.com/news-releases/news-release-details/regeneron-announces-start-regn-cov2-phase-3-covid-19-prevention
https://www.cnn.com/2020/07/06/health/regeneron-coronavirus-antibody-drug-bn/index.html
Regeneron starts Phase 3 trial of Covid antibody drug
Regeneron received $450 million to manufacture their covid artificial antibody therapy.
Interesting that the Indian death rate is less than 2%. Odd that the calculation in the covid virus tracker incorrectly states the Indian death rate to be 3%.
Comment:
And obviously the simplest solution, to stopping the spread of covid, is to correct the population’s vitamin D, deficiency. Regardless of sex or age, those who have a blood serum level of 25(OH)D that is less than 20 ng/ml have a 19 times greater chance of death or serious organ damage than those who have a blood serum level that is greater than 30 ng/ml. 82% of the US black population, 68% of the US Hispanic population, and 42% of the US general population are Vitamin D deficient, same definition for deficient and Vit D normal.
Neat. The Regeneron approach should be especially useful for immune compromised individuals, and we really should have public service announcements regarding the importance of vitamin D. This would produce all kinds of health benefits.
Once India reaches its peak in death/cases, then global numbers will begin to improve. I think that Indian cases will eventually rival or exceed those of the U.S. but India has the Asian advantage of exposure to other corona viruses and its median age is on the young side, so these contribute to lower death rates.
Eli Lilly is leading another effort with Canadian biotech AbCellera to develop an artificially produced optimized covid antibody.
https://investor.lilly.com/news-releases/news-release-details/lilly-begins-worlds-first-study-potential-covid-19-antibody
INDIANAPOLIS, June 1, 2020 /PRNewswire/ — Eli Lilly and Company (NYSE: LLY) today announced patients have been dosed in the world’s first study of a potential antibody treatment designed to fight COVID-19.
This investigational medicine, referred to as LY-CoV555, is the first to emerge from the collaboration between Lilly and AbCellera to create antibody therapies for the prevention and treatment of COVID-19. Lilly scientists rapidly developed the antibody in just three months after …
The Vit. D issue, population def. our def,… It is more interesting than I would have thought possible. It is interesting on so many levels.
The general population has an average 25(OH)D blood serum level of 26 ng/ml.
Optimum blood serum level of 25(OH)D based on stopping cancer from developing is greater than 60 ng/ml.
With a blood serum level of 25(OH)D that is greater than 60 ng/ml, the majority of our body cells…
will use the 25(OH)D to get the blueprints that….enable the cells in question.. to build special modules that sit on the cells in question.
These new modules, will on stimulus….
… as directed by the cell in question, produce bioactive chemicals which are evolution’s solution to protect and maintain the cells in question, the organ in question.
The bioactive chemicals which these new modules produce has been shown to stop the grow of cancer by stopping inflammation.
Inflammation is linked to a host of autoimmune diseases. Peer reviewed studies show that a group of diseases are prevented by the bioactive chemicals that are released when the 25(OH)D blood serum level is raised above 60 ng/ml.
This is a medical miracle, that we do not think is possible.
Our bodies have the capacity to prevent all common diseases. People are stronger. Old people do not get weak and do not lose mental capacity when their blood serum level is greater than 60 ng/ml.
It does not make sense evolutionary that there is a cohort of old people that lose their mental capacity, strength, and suffer organ failure.
The new chemical modules which the 25(OH)D provides the blueprints for…
produce evolutionary developed special bioactive chemicals at the organ, body part in question, ….
….to protect that group of cells from virus attacks, to rebuild that organ such as heart cells, to protect against cancer, to stop auto immune diseases from happening, such as type 1 and 2 diabetes, and so on.
We are different, better, stronger, smarter, less frighten, more confident, more thoughtful and patient, because we are different at a cellular level when our blood serum level of 25(OH)D is above 60 ng/ml. Our bodies build new muscle, fix problems in our body. Which explains why people lose weight and gain muscle mass when they raise their free 25(OH)D above 60 ng/ml.
It logically makes sense that are bodies do not need man made chemicals to stop common diseases and protect against all viruses.
Our bodies have the biological solution to solve the biological puzzles. 25(OH)D is required to enable the cells to do what they biologically want to do.
It is really quite amazing as there is some else.
Magnesium is essential for Vitamin D synthesis. Vitamin C and zinc are also necessary to support the immune system.
There is a general population mineral deficiency which the general public are clueless about.
Do to the fact that plants take zinc, magnesium, copper, and so on, out of the soil and we do not replace the minerals that the plants take out of the soil.
We eat the plants and the minerals go out to sea.
So because the minerals are not replaced in the soil, over time the plants that we grow to eat have less and less of the key minerals that our bodies require.
The general population is deficient in magnesium, zinc,….. and that has biological effects on those who are deficient.
Dietary magnesium has decline in the last 100 years from 500 mg/day to 175 -225 mg/day, changing depending on how much of your diet is plant based and where those plants are grown.
There is a good explanation of what magnesium does in body in this paper from the scientific journal Nutrients.
https://pubmed.ncbi.nlm.nih.gov/26404370/
Magnesium in Prevention and Therapy
Dietary surveys of people in Europe and in the United States still reveal that intakes of magnesium are lower than the recommended amounts [20–22]. Epidemiological studies in Europe and North America have shown that people consuming Western-type diets are low in magnesium content, i.e. <30%–50% of the RDA for magnesium. It is suggested that the dietary intakes of magnesium in the United States Nutrients 2015, …
….have been declining over the last 100 years from about 500 mg/day to 175–225 mg/day.
This is likely a result of the increasing use of fertilizers and processed foods [5,9,22–24]. In 1997, the Food and Nutrition Board (FNB) of the Institute of Medicine had increased the dietary references intakes (RDA) for magnesium, based on the results of controlled balance studies. The new RDA ranges from 80 mg/day for children 1–3 year of age to 130 mg/day for children 4–8 year of age. For older males, the RDA for magnesium ranges from as low as 240 mg/day (range, 9–13 year of age) and increases to 420 mg/day for males 31–70 year of age and older. For females, the RDA for magnesium ranges from 240 mg/day (9–13 year of age) to 360 mg/day for females 14–18 year of age. The RDA for females 31–70 year of age and older is 320 mg/day [6].
One word: Junk.
Nothing but 19th Century-style Snake Oil with 21st Century packaging.
The hysteria about ‘cases’ apparently has a parallel in the Swine flu epidemic. A reverse transcriptase test to identify victims came on line after the main bulk of the epidemic was past. This produced an alarming rise in ‘cases’. Since there were no more deaths at that time, it can be assumed the test was picking up the recovered who went for a test when they got some respiratory symptoms.
https://www.youtube.com/watch?v=FU3OibcindQ
Seems to be shadow banned on youtube.
Public health bodies have an interest in playing up these so-called pandemics. How about we let our immune systems and local medical facilities deal with common cold viruses like corona, adeno, and rhino. Of course a flu virus can also cause cold-like symptoms. This Covid hysteria is unprecedented. It seems to crossinfect with Trump Derangement Syndrome; further research is needed as to whether both of these are treatable or whether they are chronic conditions.:).
+1000
I don’t understand why there is still any debate over this! The data out of Switzerland shows that use of HCQ leads to a 75-80% decrease in case fatality rate! The same figure comes out of the international study comparing countries that used HCQ early in the scamdemic against those that did not! Here in the US that would be 130,000-140,000 of our exaggerated 173,000 deaths! That is the number of deaths that may be attributable to the politicians who politicized this medical emergency and then got in the way of doctors treating their patients for a power grab like none we have ever seen before.
I have seen one commenter liken this to psychological torture of the American public; we must isolate ourselves from all human contact and sacrifice our freedoms and prosperity while they pretend to be dealing with an existential crisis. But it is ALL A LIE! The solution was there all along; Fauxi even wrote about in an earlier paper on viral suppression! Now he stands to make a lot of money and wield substantial power by ignoring a simple and cheap remedy for MOST of the infected, while he touts a vaccine that seems unhelpful at best and possibly worse than the disease itself!
This has been a disinformation campaign of the first order and if the American people start to wake up to the extent to which they have been abused and lied to, these mass murderers will be facing some difficult times. Sadly, President Trump appears to have fallen for these charlatans and it may be his downfall; but without him to lead us over the next four years there soon won’t be a country that any of us recognize!
People are convinced not only that HCQ doesn’t work, but that it is so dangerous that people shouldn’t be taking it, and that it should be restricted so that only specialists are allowed to prescribe it. I’ve had these discussions – they don’t want to know what the studies say, they don’t care about the facts. They’ve been convinced it’s such a horrible drug that doctors prescribing it are killing their patients.
Medical treatment by hysteria, that’s where we are now.
Ok, I really gotta know: what did I say there that triggered moderation?
The “K” word, Tony.
Really?
I’ve been gone awhile, guess things have changed a bit. I don’t remember that being a trigger before.
Should be HCQ + Zn + Zpac. Add Vit.C &D.
In effect, roughly, I translate that a little over 1/2 of covid19 ex-patients have 96.5% immunity,
and a little less than 1/2 of covid19 ex-patients have about 74% immunity.
Plenty enough, it seems, to establish herd immunity.
Plus the vaccine should fairly abolish it.
Almost every media report I read that reports the number of deaths scrupulously omits the median age of the dead. In Canada, it is 84. Do you know anyone who is 84 or older? People that old are weak and sick most of the time, and all people that age know that they are close to death.
Two mistakes were made at the outset, when policies were enacted to contain the pandemic. The first was a gross overestimation (probably by a factor of 10) of the mortality rate of COVID-19 in people younger than 65. The second was that COVID-19 would cause death with equal frequency in people of all ages. We have known for at least three months now that these first assumptions were incorrect but the people in power would rather eat shingle nails for breakfast than admit that they got it wrong, especially since the measures to contain the spread of the virus must cause so much misery to so many people.
I live in Edmonton, Canada, which has a population of 918,000. As I write this, there are 23 people (ages unreported) in Edmonton hospitals with a diagnosis of COVID-19. No one I know knows anyone who has had COVID-19, and I’m 68. Only the stupidest and most supinely obedient young people actually believe that this is a serious health crisis.
It’s not the public who need educating!!
It is the arrogant idiots who can’t believe we have herd immunity because not enough people tests positive (in their view) from their silly tests. The reality is even if every country opened up and ended the epidemic at the Sweden/UK levels and then cases categorically crashed, these morons will continue believing that herd immunity has not been achieved despite the virus obviously dying – just because their test isn’t showing enough people with antibodies.
New Zealand vs Sweden:
“Reaching For The Precious”