Reposted from Dr. Judith Curry’s Climate Etc.
Posted on June 28, 2020 by niclewis |
By Nic Lewis
The course of the COVID-19 pandemic in Sweden is of great interest, as it is one of very few advanced nations where no lockdown order that heavily restricted people’s movements and other basic freedoms was imposed. As there has been much comment, some of it ill-informed, on how the COVID-19 epidemic has developed in Sweden, but relatively little detailed analysis published in English, it is worth exploring what their excellent publicly-available data reveal.
I present here plots of weekly new cases and deaths, with accompanying comments. I have been able to access detailed daily data from 2 April on.[1]
Overall development of the epidemic
Figure 1 shows the overall picture for confirmed weekly total new COVID-19 cases, intensive care admissions and deaths in Sweden. The dashed line normalises new cases by the dividing by the number of tests carried out each week, relative to those for the week to 10 April. Both actual and normalised weekly new cases have been divided by 10 in order to make their scale comparable to that for ICU admissions and deaths.

Fig. 1 Total weekly COVID-19 confirmed cases, intensive care admissions and deaths in Sweden
Several points are noteworthy:
- Recorded new cases continued rising until mid-April, and after gently declining from then until late May have doubled since then. All or most of that increase appears to have been be due to a decision on 5 June to expand testing. By the end of June testing was at about double the rate in May, which in turn averaged approximately 25% higher than in April.
- Allowing for the increase in testing over time, the incidence of COVID-19 appears to have declined by about 30% from mid-April until the late May and has since remained broadly stable.
- Deaths peaked in mid-April and have fallen by two-thirds since then.
- It follows that the infection fatality rate has fallen substantially since early in the epidemic.
- Deaths have been remarkably high in relation to confirmed cases. To a substantial extent this reflects Swedish policy of focussing testing in hospital, where the disease is severe, prior to June. It also reflects the spread of infections to care homes, where death rates are very high, relatively early in the epidemic.
- Far more people have died than have been put into an intensive care unit (ICU). This likely reflects a combination of deaths outside hospital and an apparent Swedish policy of not generally putting people aged 80+ into intensive care.[2] For admissions before late April, 49% of 70+ year old patients (who only comprised 15% of total ICU patients) died, and most of those were people in their seventies, for whom the prognosis is much better than for older patients.
Analysis by age group
The changing age composition of new cases over time is shown in Figure 2. The number of cases among people aged 70+ has been declining since mid-April. Until the end of May this more than countered gently rising infections in age groups younger than 60, with infections among 60-69 year olds broadly stable. But since then confirmed infections in people under 60 have rocketed, and there has also been a noticeable increase in infections among people aged 60-69.
It is likely that the bulk of these increases simply reflect the widening of testing in June. The total number of tests in the latest week was double that four weeks previously. The Swedish Public Health Agency estimates that the current reproduction number, Rt, in Sweden during mid- June was approximately 0.9, implying a decline of about 10% a week in the true number of new infections. However, comparing Figures 1 and 2 suggests that while infections in the oldest age groups are reducing steadily, this is being counterbalanced by an increase in infections among young people, resulting in little overall trend in the total number of infections.
Fig. 2 Weekly COVID-19 confirmed cases by age group in Sweden
{kind=link}
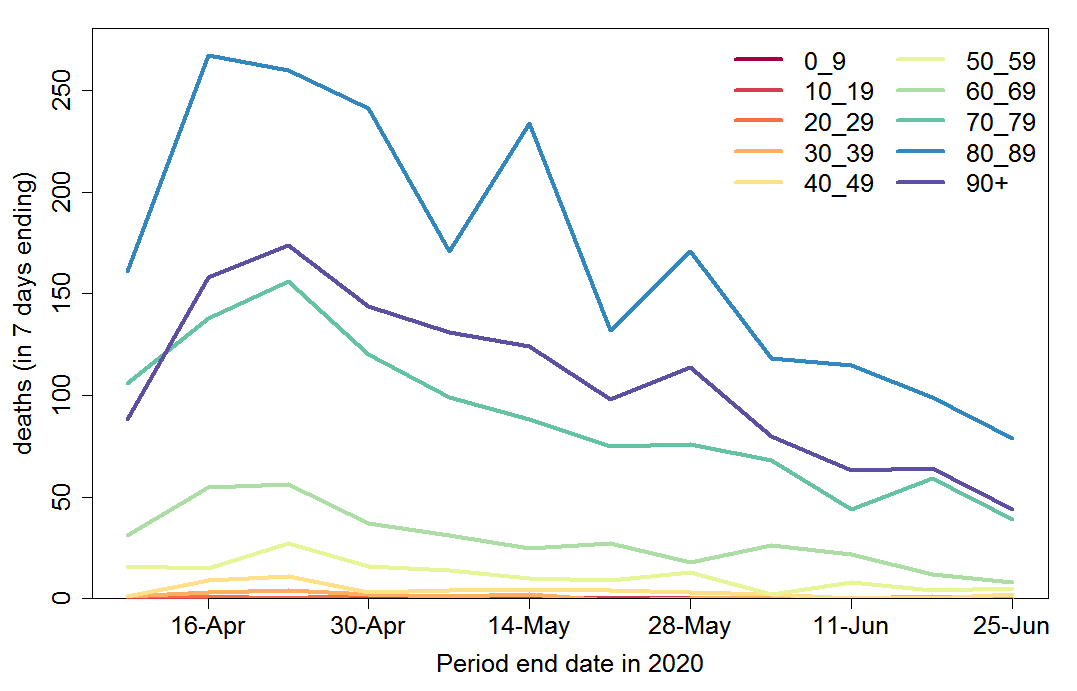
Weekly COVID-19 recorded deaths have declined very substantially since mid-April, across all age groups (Figure 3). The data show the number of people with confirmed COVID-19 who died, regardless of the cause of death.
Fig. 3 Weekly COVID-19 recorded deaths by age group in Sweden
{kind=link}
Figure 4 shows weekly deaths by age group as a proportion of new cases two weeks previously. Since most cases are only confirmed after hospitalisation, the average delay from a case being confirmed to death occurring is around two weeks.[3] This ratio therefore should provide a reasonable estimate of the hospital case fatality ratio (CFR). It has declined substantially for all age groups, albeit proportionately less for ages 80+, where it remains very high, although not unusually so.
The estimated hospital CFR for ages 50–69 has declined by an order of magnitude, while that for ages 70–79 has declined by a factor of three. The reasons for this extremely welcome trend are not entirely clear. Much of the reduction over the last few weeks is very likely due to a widening of the testing regime to include milder cases of disease, with more cases now being found outside hospitals.[4] Nevertheless, a good part of the decline is likely real: most countries have seen a decline in the hospital CFR over time.

Fig. 4 Weekly COVID-19 deaths by age group in Sweden as fraction of new cases 2 weeks before
Infection fatality rate over time
The decline in total deaths (Figure 1) is to a fair extent due to the changing age composition of new cases, as well as a moderate reduction in total infections, with an increasing proportion of cases among younger age groups and a substantial decrease at ages 80+, which account for most deaths. But within some of the key older age groups, which account for the vast bulk of deaths, the number of deaths (Figure 3) appears to have dropped in relation to the number of cases as adjusted for the widening of testing – certainly for ages 60-69.
The Swedish Public Health Agency estimated the infection fatality rate (IFR), based on a selection of confirmed cases that have been tested in Stockholm County and who fell ill on March 21-30, 2020, after adjusting by the estimated proportion of infections that resulted in confirmed cases.[5] Of all people who they estimated to be infected with COVID-19 around the second half of March, 0.58% died.[6] In the group At age 70 and over, mortality was 4.3% (1.9% for ages 70-79) , while it was 0.09% for persons younger than 70 years.[7] [8] The overall deaths were pushed up by the spread of infections to care homes, residents of which accounted at that point for 40%–50% of total deaths.
The order of magnitude decline in COVID-19 CFR at ages below 70 since mid-April implies that, even assuming that all the change in confirmed cases between early April and mid June is due to the three-fold expansion of testing, the IFR below age 70 is now much lower than the previously estimated 0.09%. The data indicate a current level of circa 0.015%. Even for ages 60-69, where the IFR for infection in mid-March was estimated at 0.45%, the implied IFR is now little over 0.1%.
It is not clear what has caused such a large reduction in IFRs for COVID-19 at ages below 70 years. Sweden is not the only country in which the IFR appears to have declined. There is little evidence of the SARS-CoV-2 virus having mutated and become less damaging. However, treatment of serious cases has no doubt improved; less use of invasive ventilation could be one factor here. Seasonal factors may also play a role. The body’s ability to fight infections and heal damage appears to be affected by sunlight exposure, with vitamin D and nitric oxide pathways perhaps both being involved.
Another important factor in the decline in the IFR over time could be population heterogeneity in susceptibility to COVID-19 infection, in particular variability arising from biological rather than social connectivity factors. More susceptible individuals may not only be more likely to succumb to COVID-19, but more likely to die of the disease once infected. Since more susceptible individuals will tend to become infected earlier in the epidemic than less susceptible individuals, a correlation between susceptibility to infection and risk of death if infected would automatically lead to the IFR declining over the course of the epidemic.[9]
Regional analysis
I turn now to regional analysis. Figure 5 shows weekly confirmed new cases for each of the 21 regions in Sweden. Although widening of testing varied between regions, it is evident that Västra Götaland dominates the overall increase in cases over time. However, the increase in testing during the first half of June appears to have been much larger in Västra Götaland than elsewhere, so the true increase in disease incidence is likely far smaller than the increase in confirmed cases suggests. Cases in Jönköping also rose sharply in June, albeit from a much lower level. Cases in the Stockholm region remain high.
Tracking serious cases only, so as to adjust for the widening of the test regime, comparison of the latest analysed week (24 – week ending19 June) with the average of the previous three weeks shows an increasing number of cases in Västernorrland, decreasing numbers in Jönköping, Stockholm, Sörmland, Uppsala, Västra Götaland and Östergötland, and an unchanged number for other regions.[10]

Fig. 5 Weekly COVID-19 confirmed cases by region in Sweden
Regions have varying populations, so confirmed cases per 100,000 head of population give a better picture of relative disease incidence (Figure 6).

Fig. 6 Weekly COVID-19 confirmed cases per 100,000 head of population by region in Sweden
Deaths by region are shown in Figure 7. They are dominated by deaths in Stockholm region, which continue to be higher than elsewhere, although since mid-May deaths in Västra Götaland have become a much more substantial proportion of the total.
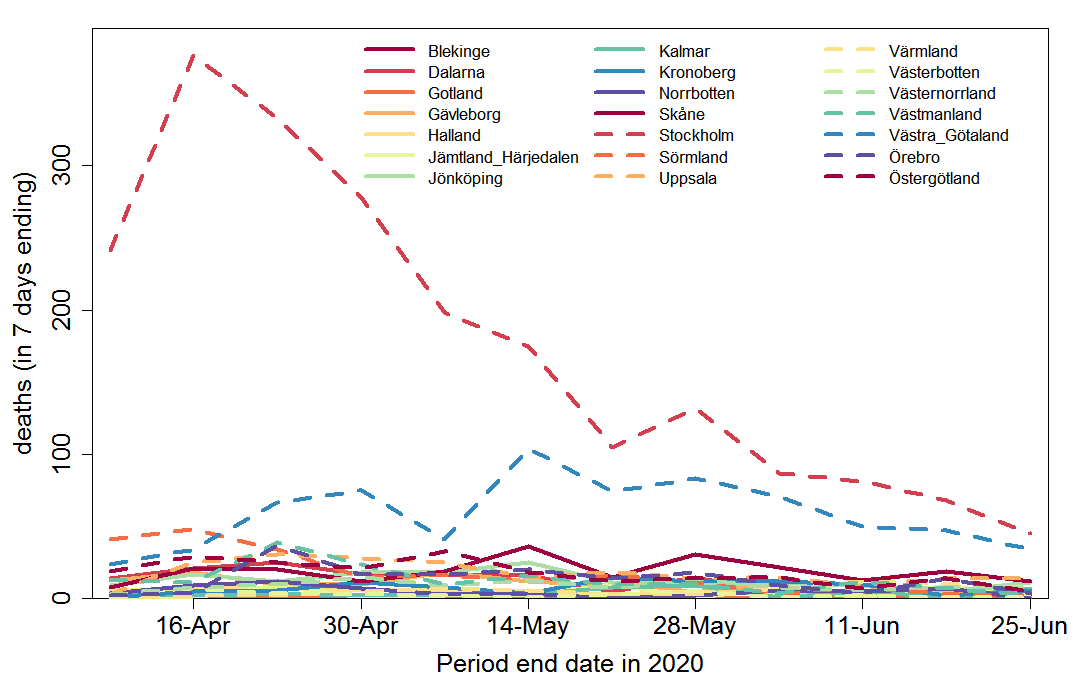
Fig. 7 Weekly COVID-19 recorded deaths by region in Sweden
The very large and almost monotonic decrease in deaths in Stockholm region, confirms that the less steep decline in cases from mid-April to the end of May (which occurred despite some increase in testing) is genuine. As already indicated, the sharp increase in confirmed cases in June is an artefact produced by the widening of testing; serious cases decline in Stockholm county.
Prevalence of COVID-19 infections
Analysis of samples collected at week 21 (late May) shows that antibodies were detected at 6.3% of the studied population. Seroprevalence remains lowest among adults 65-95 years (3.9%), compared to adults 20-64 years (7.6%) and children 0-19 years (7.5%). The Stockholm region had the highest proportion of antibody positive (10%) followed by Skåne (4.5%) and Västra Götaland (2.7%). The number of collected samples for other regions were less than 100 and therefore cannot provide reliable results.[11]
Cumulative confirmed cases as a proportion of population up to the end of week 19 (15 May), who would be expected to develop antibodies by early in week 21, were 0.32% for the whole of Sweden, 0.47% for Stockholm region, 0.11% for Skane and 0.29% for Västra Götaland. So, up to mid-May, if the foregoing prevalence estimates are correct then confirmed cases represented about 1 in 20 of people who had developed antibodies to the SARS-CoV-2 virus, but with an inter-region range of at least 1 in 40 to 1 in 10.
However, previous results showed higher prevalence, and prevalence cannot decrease over time. A fairly large sample study that sought response from a random sample of households in the Stockholm area obtained 446 valid results from tests on an average date of 11 April (week 16), reflecting infections up to late March. It found 10% prevalence.[12] And a study based on blood donors showed about 11% had developed antibodies in mid-April, although the sample size was only 100.
Moreover, the antibody tests used appear to have a sensitivity of only 70-80 percent, so 20-30% will test negative even though they have been infected. But the tests have 100% specificity – no one will test false positively.[13] There is no indication that any of these seroprevalence results have been adjusted for the relatively low sensitivity of the test used. So it seems likely that in all cases the true prevalence was 25-43% higher than that reported.
Many people with mild COVID-19 symptoms or asymptomatic infection probably do not develop antibodies in their blood, either developing antibodies only in their mucus or not at all. Antibodies are only one component of the adaptive immune system, and immunity conveyed by the development of SARS-CoV-2 specific T-cells may be more important; it is likely to be longer lasting.
Having regard to all these factors, it seems entirely possible that 20% rather than 10% would be a better estimate of the proportion of the population of Stockholm region that had been infected by late May.
Future outlook
It seems clear from the trend in cases since then that, as I intimated previously[14], by mid- April the herd immunity threshold had been reached in Stockholm county. Moreover, both there and in Västra Götaland, the two regions that have dominated deaths to date, deaths have been declining since mid-May. Regression of the logarithmic change in deaths over the last seven weekly data points gives similar results in both regions. The fits are good[15] and the slope estimates, averaging them, imply that each week’s death figure is only 81% to 86% ( at ± 1 standard error) of the previous week’s figure. Skåne, the next largest region by population, also has a downward trend in deaths, but the regression fit is less good and the slope estimate is not significant (p = 0.1). Those three regions make up 53% of Sweden’s population. For Sweden as a whole the fit is as good as for Stockholm country and Västra Götaland , with a slightly slower rate of decline: each week’s estimate deaths are 84% to 88% of the previous week’s. This range is slightly below the R value in mid-June estimated by the Swedish Public Health Agency, which has fluctuated around 0.9. The difference is likely to reflect the declining proportion of new cases made up by older age groups (Figure2) and the declining infection fatality rate for ages under 70.
If the estimated logarithmic rate of decline in weekly COVID-19 deaths in Sweden seen over the last six weeks continues, only about 1,100 further deaths would occur. That would bring total deaths up to approximately 6,400, or 0.06% of the total population. Of the first 4,500 deaths, some 40% involved people living in care homes,[16] a slightly lower proportion than earlier in the epidemic. To date, the average age at death was 82, and in only 6% of cases did a death not involve a co-morbidity (other health condition).
Conclusions
Notwithstanding that a month ago antibodies were only detected in 6.3% of the Swedish population, the declining death rate since mid-May strongly suggests that the herd immunity threshold had been surpassed in the three largest regions, and in Sweden as a whole, by the end of April.
In the absence of a change in trends, it seems likely that the epidemic will peter out after a thousand or so more deaths, implying an overall infection fatality rate of 0.06% of the population (0.04% excluding COVID-19 deaths of people in care homes). This is broadly comparable to excess deaths from influenza infections over two successive above-average seasons, such as 2016–17 plus 2017–18.[17]
The absence of a lockdown order, with the government largely trusting people to make their own individual decisions regarding their behaviour, informed by their particular circumstances, has enabled life to continue with less disruption and reduction of people’s autonomy in Sweden than in most other western European countries. While this has also meant that COVID-19 deaths to date have been higher than in some (but not all) other countries in which a lockdown was imposed, the wider spread of the epidemic in Sweden means that the future COVID-19 outlook there is better.
The herd immunity threshold is likely lower at present than it would be if people were behaving completely normally; it may also be seasonally lower. However, the continuing spread of infections since the peak of the epidemic, particularly among young people, should provide some margin of safety against its resurging when behaviour returns closer to normal and summer ends. That is, there is less risk of a second wave of the epidemic next winter. And if a second wave occurs, fewer measures should be needed to control it than in other countries.
Nicholas Lewis
Originally posted here, where a pdf copy is also available
[1]On 2 April 2020 the cumulative number of cases was only one-twelfth its current level, and only 5% of the deaths recorded to date had occurred. Updated data for 19, 20 and 21 June were not prepared. In order to avoid these days and plot as many weeks as possible, I use data for Thursday 2 April 2020 and each 7 days thereafter, ending 25 June. For consistency between the breakdowns by age and region, I use the data as originally reported on each date, not the final adjusted daily figures (which are not reported by age group). There is some lag in reporting, particularly for deaths.
[2] Such a policy would be understandable, as the prognosis for 80+ year-olds given invasive ventilation in ICUs is extremely poor, with many of those who do survive then having a poor quality of life.
[3] The average delay between a case being confirmed and death occurring is 12 days. (https://www.folkhalsomyndigheten.se/publicerat-material/publikationsarkiv/t/the-infection-fatality-rate-of-covid-19-in-stockholm-technical-report/) However, there is a significant delay between sickness arising and cases being confirmed. On average, it takes 11 days between sickness and the start of intensive care.
[4] The earlier increase in testing, from mid-April to mid-May, appears to have largely been targeted at, and detected more cases in, health and care staff. In week 20 (mid-May) the proportion of confirmed cases comprised of healthcare and care staff was as high as 74% in the Kronoberg region. https://www.folkhalsomyndigheten.se/globalassets/statistik-uppfoljning/smittsamma-sjukdomar/veckorapporter-covid-19/2020/covid-19-veckorapport-vecka-20-final.pdf
[5] They assumed that the estimated infections were spread evenly over the population of the Stockholm region, that is an age-independent atack rate.
[6] Measuring instead by the number of excess deaths in the relevant period over the estimated average number suggests a slightly higher overall mortality rate of 0.7%. However, mortality earlier in the 2019-20 winter period was lower than average, as it also was in the 2018-19 winter, so there were probably more than usual very old people likely to die from infection when COVID-19 struck. By week 23 (week ending 5 June 2020) the difference between the two measures was only about 10% (4,811 vs 5,353). (https://www.folkhalsomyndigheten.se/globalassets/statistik-uppfoljning/smittsamma-sjukdomar/veckorapporter-covid-19/2020/covid-19-veckorapport-vecka-25-final.pdf)
[7] https://www.folkhalsomyndigheten.se/globalassets/statistik-uppfoljning/smittsamma-sjukdomar/veckorapporter-covid-19/2020/covid-19-veckorapport-vecka-24_final.pdf
[8] https://www.folkhalsomyndigheten.se/contentassets/53c0dc391be54f5d959ead9131edb771/infection-fatality-rate-covid-19-stockholm-technical-report.pdf
[9] If much of the variability involved arose from whether and how many cross-reactive T-cells – such as arise from previous exposure to common cold coronaviruses – an individual possessed, the much smaller decline in IFR for 70+ age groups might perhaps be due to the T-cell senescence that occurs in old people.
[10] https://www.folkhalsomyndigheten.se/globalassets/statistik-uppfoljning/smittsamma-sjukdomar/veckorapporter-covid-19/2020/covid-19-veckorapport-vecka-25-final.pdf
[11] https://www.folkhalsomyndigheten.se/globalassets/statistik-uppfoljning/smittsamma-sjukdomar/veckorapporter-covid-19/2020/covid-19-veckorapport-vecka-24_final.pdf
[12] https://www.kth.se/aktuellt/nyheter/10-procent-av-stockholmarna-smittade-1.980727
[13] https://www.svt.se/nyheter/inrikes/11-procent-av-stockholmarna-har-antikroppar-mot-covid-19
[14] https://judithcurry.com/2020/05/10/why-herd-immunity-to-covid-19-is-reached-much-earlier-than-thought/
[15] The R-squared is close to 0.90 in both cases.
[16] https://www.folkhalsomyndigheten.se/globalassets/statistik-uppfoljning/smittsamma-sjukdomar/veckorapporter-covid-19/2020/covid-19-veckorapport-vecka-22-final.pdf
[17] https://www.folkhalsomyndigheten.se/contentassets/4b4dd8c7e15d48d2be744248794d1438/rapport-overdodlighet-vecka-23-2020.pdf
“Allowing for the increase in testing over time, the incidence of COVID-19 appears to have declined by about 30% from mid-April until the late May and has since remained broadly stable.”
It’s true that some allowance should be made for the effect of extra testing. But simply substituting the fraction of positive tests, which this seems to do, goes too far the other way. As testing expands, the population being tested has less prior suspicion of having Covid; the expansion often consists of going from testing people with symptoms or exposure, to testing randomly. So you would expect the fraction positive to go down, even without a change in true Covid prevalence.
Good to see you are keeping up your healthy balanced diet of meat, diary and word salad.
What are you actually attempting to say? “Less prior suspicion”? You seem to suggest this is a bad thing.
By testing randomly we are gaining an understanding of how many asymptomatic cases are actually out there. If I have been following other research correctly I believe a Spanish study suggested a 5 times amount of actual cases while a Swiss one was claiming a 12 time increase.
What we are however not seeing is a 5 time and 12 time increase in hospital cases and/or deaths.
The suggestion here is that anywhere from 80 to 92% of cases are actually asymptomatic. This by extension suggests a few more things.
Firstly that Wuhan Virus is not the massive killer everyone fears – thank Grud.
The second is that it may not actually be as contagious as everyone feared. Again using Sweden as our test subject we have a country which has been internationally accepted as the poster child for ‘Nah… It will be fine.’ Having done the absolute minimum to contain spread and having shown the amount of actual cases is much higher than expected due to all the asymptomatic types casually interacting with society, then basically every man and his dog in Sweden should have had or currently have the virus by now.
We can look at other examples to support these arguments. Here in Australia we have Chairman Dan’s Victoria which, being hard Left not only enforced harsher lockdowns than any other Australian State, but also happily allowed 10,000 protestors to gather. At least one of these protestors was then very soon after confirmed as being Wuhan positive.
So IF the virus was as proactive as everyone claims/fears, a significant amount of these protestors should been confirmed as cases by now. Australian media made a massive sound and dance these last few weeks because of a mere 20 something ‘new cases’ in Victoria. If say 1% of the protestors above became infected then we SHOULD have seen at least 100 new cases and… we haven’t.
Remember, we live and work in the real world and in legal terms As Far As Is Reasonably Practical is how you measure pro-active attempts at risk reduction. Yes, Your Country May Vary, but it is how the system works. Legally. Is it Reasonably Practical to ask or even force people with symptoms to isolate? Probably. Is it Reasonably Practical to ask everyone to isolate and to isolate for extended periods of time? Open to question and needs to be taken in context of many variables, BUT, the question does need to be asked.
Nothing is every 100% safe. All we can do is reduce the risks.
I appreciate your commentary on the Swedish statistics and what they may mean. I wonder about one other possibility. Not much has been said about a possible relationship between the quantity of virus received in the initial exposure and the subsequent severity of the illness. Since there is very little antibody testing going on I wonder if we are seeing acquired immunity from more common “light”exposure.
Earlier today I was reading an article about the G strain. In that article it says the G strain is better at infecting cells than the D strain leading to a higher overall virus loading but that in turn did not appear to increase how sick one got over the D strain. So if that article is correct then the answer to your question would be no.
Nick, in fact this part of the statement “has since remained broadly stable” says that Herd Immunity has NOT been reached.
New cases adjusted for more testing should be going down not staying stable.
Compared to the very badly handled UK situation where we have also drastically increased testing since April the Sweden new cases are not doing the same thing at all.
The values below are since the beginning of June and are as follows
Day UK New Cases UK 7 day cases/Million Sweden New Cases Sweden 7 day cases/Million UK New Deaths UK 7 day Death/Million Sweden New Death Sweden 7 day Death/Million.
1 1570 208 644 446 111 27 8 37
2 1653 202 889 459 325 30 65 34
3 1871 191 1070 485 359 29 74 32
4 1805 190 1042 512 176 26 20 30
5 1650 183 1143 549 357 25 77 29
6 1557 182 825 588 204 25 17 26
7 1326 173 462 608 77 24 3 26
8 1205 168 542 597 55 24 35 29
9 1741 169 936 602 286 23 23 25
10 1003 156 1427 638 245 21 78 25
11 1266 148 1326 666 151 21 19 25
12 1541 146 1251 677 202 18 40 22
13 1425 144 1113 706 181 18 20 22
14 1514 147 419 701 36 18 0 22
15 968 143 708 718 38 17 17 20
16 1279 136 1283 753 233 16 48 22
17 1115 138 1506 761 184 16 102 25
18 1218 137 1558 784 135 16 12 24
19 1346 134 1341 793 173 15 0 20
20 1295 132 774 759 128 15 0 18
21 1221 128 322 749 43 14 0 18
22 958 128 813 760 15 14 69 23
23 921 122 1344 766 280 14 39 22
24 652 115 1699 785 154 15 48 17
25 1118 114 1085 738 149 14 21 18
26 1380 114 303 634 184 14 50 23
Sorry about the formatting as it is straight from Excel.
But as can be seen the latest data has UK 7 day cases/million at 114 against Sweden’s 7 day cases/million at 634, the UK 7 day Deaths/million are 14 against Sweden’s 7 day Deaths/million of 23.
How can anyone comparing the UK with one of the worst lockdowns in the world with Sweden’s current position believe that Sweden’s performance shows that lock downs do not work
I cant really see any major difference between UK and sweden while looking at deaths per million using your data.
Population in Sweden 10.3M
If we remove our capital-region(2.4M citizen) which is about 50% of the cases but less than 25% of the population, Sweden has outperformed UK.
It’s all about how hard you got hit before restrictions where implemented. In southern Sweden, Skåne(1.4M citizens), there are about 10% of the cases compared to Stockholm.
If Skåne in sothern Sweden was an own country with 1.4M citizens, implementing the Swedish restrictions, and you looked isolated on the country “Skåne” then the voluntary restrictions work perfectly fine. In Skåne the death rate is not far behind Denmark which had much more severe lock down.
The infection was not nearly as much spread in Skåne as in Stockholm when the restrictions where implemented. Skåne where probably weeks behind Stockholm so if Skåne would have waited a few weeks more before implementing the restrictions then I think that area would have been hit just as hard as Stockholm.
You have to remember that London has the population of the whole of Sweden and the London Tube has twice the population of Stockholm stuffed in tube trains twice per day.
The UK at no time closed our borders, not Airports, Ferries or the Channel Tunnel. Our lockdown did not prevent 1.25 Million people coming in to the UK from all over the world, regardless of their infection rates and there was no quarantine or checking of the visitors.
Essentially the same is true for Sweden. There has never been any checking of visitors.
Except for the Stockholm area there is as yet virtually no testing of non-symptomatic people. In most aeas getting tested is quite difficult even if you are symptomatic.
no, because much of the new testing is driven by contact tracing, where you would expect to find more positives.
“It seems clear from the trend in cases since then that, as I intimated previously[14], by mid- April the herd immunity threshold had been reached in Stockholm county”
The evidence for this effectively is that infectivity Rₜ≤1. This would happen if herd immunity is reached, but can happen because of behaviour changes, or even weather. Denmark, Norway and Finland, among many other places, also had declining cases and deaths, without approaching herd immunity. I see nothing that specially relates Stockholm data to herd immunity.
Indeed the conclusion “herd immunity”, even if worded “appears”, is highly speculative and even unlikely. I guess we will all have to wait until the aftermath, at least a year or more.
There is clearly much that we do not understand about this epidemic. The simplistic SEIR type models seem to be totally inadequate which suggests there are other factors such as a partial immune response acquired from prior exposure to other corona virus strains.
Despite continued attempts by the press and others up maintain the fear, I see no reason to expect a “second wave” next winter.
There is no indication that sars-cov-2 has the same seasonal tendency of regular influenza viruses. Currently there is a resurgence of covid-19 in hottest states across the southern USA: Florida, Texas, N.M and California. Hardly consistent with the idea that has been naturally reduced by the arrival of summer and with will re-emerge in a second wave this winter.
The big surprise is that as confinement measures have been released there has not been a resurgence of the first wave of infections. According to the simplistic epidemiology being promoted so far, confinement was expected to simply spread the problem over a longer period, not lead to a sustained drop in infections once measures were removed.
There has been no resurgence in the main european countries which are largely circulating and working now with token mask wearing by proportion of the population.
My perception in south of France ( which like 3/4 of the country had very low infections through ) is that about 1/3 of folks in towns are wearing masks. Most that are, are of retirement age.
Summer still can have impact. It is about Vitamin D levels. People are usually adapted on their climate and receiving just right amount of Vitamin D. In hot countries people have darker skin, or using protection as cloth in Arabian countries, sunscreen as in California.
In Europe level of Vitamin D is strongly oscillating between winter and summer. So currently with maximum D levels in Europe and Sweden we can see positive impact.
An interesting paper re the temperature and (rel/abs) humidity: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3550308. Of course, it could also be that the countries that lie between 30 and 50 latitude are better at reporting…
Absolutely! It is interesting to notice that there is no official information recommending increased vitamin d, vitamin c and zink intake. Is this intentional?
“The simplistic SEIR type models seem to be totally inadequate which suggests there are other factors such as a partial immune response acquired from prior exposure to other corona virus strains.”
The elderly typically don’t go out as much as most people, reducing the likelihood of exposure to other such strains, and thus possibly immunity, as well. Greater indoor living might also reduce vitamin D levels in elderly at the same time.
Having lived in Austin Tx I can assure you that it will be hot and sunny. However, it is too hot to stay outdoors for too long and most people will see off most of the day in ice-cold malls, cinemas, bars and houses. The exposure to sunlight is minimised by most of the population, unlike the hordes of Brits who flock to the nearest stretch of beach to lap up the sun and mimic lobsters. It would be interesting to see some data on summer vitamin D deficiency in the southern US states (and Singapore etc).
I read somewhere that around 40% people in California have D deficiency, with darker skin people up to 60%.
So hot and sunny climate is not guarantee of sufficient D levels.
And from observing I see that Vitamin D is main driver in seriousness of this disease.
So the summer cold season for Austin due to the AC??
I have a dark complexion -thanks to my Cherokee side, so I have to take Vitamin D supplements. whe I get exposed to teh sun all I do is get darker and no burns.
Living at 45N doesn’t help even in the dry side of Oregon.
“There is no indication that sars-cov-2 has the same seasonal tendency of regular influenza viruses. ”
SARS did. Chinese Flu is a close relative of SARS. Therefore it’s highly likely that it will show similar behaviour in hot, humid weather.
“Currently there is a resurgence of covid-19 in hottest states across the southern USA: Florida, Texas, N.M and California.”
States where people will be spending most of their time in air-conditioned interiors, which is where SARS spread in hot, humid Singapore.
SARS disappeared because of its self-limiting diagnosic criteria. The virus didn’t go any where; they just stopped testing for it because the diagnostic criteria were no longer met to justify such.
http://theinfectiousmyth.com/book/SARS.pdf (links to pdf)
What a BS. SARS was contained by tracking and testing and never had the chance to get seasonal. It resurged a couple of times in limited outbreaks by idiots who were working on it in research labs and contracted it there.
How obviously careless SARS was handled in some Asian virus labs is the only reason I don’t disregard an outbreak from a lab where bat viruses are studied as source for SARS-CoV-2 as a valid possibility. Cause it happened before. And to see how different the interpretation of BSL1 and BSL2 about virus and bacteria work in the US are compared to Germany I don’t want to imagine China and BSL3 at all.
“What a BS. SARS was contained by tracking and testing and never had the chance to get seasonal.”
A study in Asia showed that SARS couldn’t spread easily in hot and humid conditions. If that’s your idea of ‘BS’, then I guess there’s no point responding to your BS in future.
@MarkG
The study you are probably referring to was testing the stability on surfaces. No real evidence from spreading events in the world outside the lab was evaluated. It was only speculated that the lab conditions with lower, NOT inactivating stability (T>38C and humidity>95%) could be a reason for lower incidence in Malaysia, Indonesia or Thailand. What is a very bold claim when the data in the paper show nearly no effect to the stability at T=33C and humidity 80-90%.
The epidemiological data does not at all support any of your claims.
But the BS was referring to the linked pdf anyway.
The whole article is highly speculative and not worth reading, in my opinion.
The pandemic is still in progress — accurate conclusions are not yet possible.
Sweden herd immunity = not even close.
Southern US states are getting hot so people spend a lot more time indoors with AC on.
The virus spreads indoors much faster than outdoors.
If bars and restaurants are open for them, that leads to faster spread.
The many outdoor protests with people sceaming, often without masks, leads to faster spread too.
It takes a few weeks to notice … and the mainstream media are trying to cover up the spread caused by protests and riots.
Also important:
How well did people social distance?
(Not the official rules – what people actually did).
How many people flew in from China, Spain, France, UK, etc., and how were they isolated from the local population, assuming they were isolated.
There are far too many unanswered questions for an article like this one — pure speculation about Sweden.
Sweden had good voluntary social distancing.
There may be other factors we don’t yet know about — by early 2021 it may be possible to come to a reliable conclusion about what actually happened in Sweden, and why.
“The whole article is highly speculative.”
An opinion I’m somewhat inclined to share. It seems to me a massive overanalysis of atrocious data collected against poorly defined baselines. The same is true of data from other countries. Probably more so in most cases.
About the best I can say is that Nick Lewis at least makes a probably testable assertion — 1100 additional fatalities — although we’ll have to wait a while to see how well he does.
I would like to see a similar analysis from Norway and Finland compared with Sweden. They are much more similar in latitude and population density. Comparing with countries like the UK is not useful imo.
Agreed. The herd immunity threshold speculation/claim is particularly under-evidenced.
“how were they isolated from the local population, assuming they were isolated.”
They were not, which is the main reason for the extensive epidemic in the Stockholm area. When Spring Holiday skiers returned from the Alps nothing whatsoever was done, despite knowledge about the epidemic in Italy. Within two weeks the epidemic was out of control.
I’ll be a lot happier if cases don’t pick up by late fall. Coronavirus is strongly seasonal.
The cold Aussie state of Victoria has experienced a big spike of cases along with the cold weather. My fear is this thing will just linger in people’s lungs, then strike them when the weather turns.
Everyone thought Spanish flu was defeated in August 1918, but it came roaring back in September.
2c nights 13c days everyone indoors, not a good look especially using rev cycle aircon nowdays.
the morons at protests for blm and ex reb didnt help matters
neither did the moslem families that just had to celebrate Eid against their own imams advice not to.
those able to are using cars not public transport at least.
rural areas clear so far but school hols and fools who must travel to country are a big risk for us out in the safer zones;-(
I manage to buy a decent supply of VitD and zinc before shtf and live alone so its all good;-)
Nick, you hint of genetics but nothing of ethnic origin. Maybe, the data is not complete. There have been indications that Sweden has one of the highest ratios of “refugees” in Europe. Also, there have not frequent mentions of no-go areas particularly in Gothenburg (which was such a nice city when I visited in the mid-1980). Gothenburg is in Vastra Gotaland which according to your figure 5 is having increased cases more than Stockholm. Recent upsurge in Victoria Aust has been attributed to celebrations of EID.
A ‘lockdown’ was never going work in Sweden because ‘refugees’ would simply ignore it. Also, if the theory about Vitamin D deficiency making people more vulnerable is true, then a large fraction of the ‘refugee’ population is likely to be deficient and highly vulnerable.
““We do see certain areas that are maybe more affluent with a bigger number of people working from home,” said Kristofer Agren, the head of data insights for Telia. Data shows a 12 percentage point difference between Danderyd, one of Stockholm’s most affluent suburbs, and Botkryka, one with the highest percentage of first- and second-generation immigrants.” https://abcnews.go.com/International/wireStory/coronavirus-takes-toll-swedens-immigrant-community-70593594
Nick Stokes. Never knowingly on the right end of any argument. Sweden proves lockdown was unneeded and ineffective, whether or not herd immunity was achieved.
If Joe Biden was President right now, he’d be singing a totally different tune. This was all political, China by design, with their globalist satellites following right along to “get back” at us. Sweden abhorred at thought of subjecting their population to that.
@ Chaswarnertoo. Sweden does not prove anything about what would have worked or not in other countries with very different demographics.
Even if you do not agree with Nick Stokes, even if he is just playing devil’s advocate, a contrarian position is ESSENTIAL in any debate. Thankfully he puts in the time to comment.
Plus he usually raises valid points which are worth discussion even if way above the heads of the many clapping seals wasting bandwidth here.
Here, here.
Proves nothing, northern Europe countries has strong tradition of getting Vitamin D not from sun but from fishes. I read article that 30 years ago it was mandatory to use fish oil as D source in Sweden and even now more than 40% of population are taking it.
Go little south and you get more D deficiency as in north during winter.
They just did what they could, but it does not mean that other countries including US could afford that.
Norther Europe countries all coped well with Coronavirus – Iceland, Finland, Norway, Sweden
Stokes provides both evidence and reasoning; you provide neither. Explaining how you disagree with one or both, as some other commenters here have done, is what intelligent people do. Doing neither provides evidence of your ___ (I’ll let you fill in the blanks).
It should be noted that at least the numbers from sweden reported in norwegian newspapers are deaths of people with covid19 while norwegian authorities report deats from covid19. I dont know how others report fatalities, or if these ar the numbers used in this report.
I think the difficulty throughout has been trying to disentangle that knot of “with” and “from”.
The example quoted some months ago was of a man with a known heart condition who got into difficulties while swimming and died. The autopsy showed a heart attack which would have been almost immediately fatal but in reality he drowned. So what goes on the death certificate?
The only certain lesson that we can learn from this crisis – at this stage — is that in the event of a major infectious outbreak, “protecting” your health care system by offloading elderly patients into care homes without making sure they are not themselves carriers is not a clever move!
I’ve said elsewhere that until the official bodies, like the British Office of National Statistics, get round to crunching the numbers — which will probably need to be after next winter’s “excess deaths” season — we won’t have a clear picture of just how serious this virus is. At the moment the UK death rate is barely half that of the 1968 H2N3 ‘flu outbreak.
Nick,
You need to base your “Lockdowns are a waste of time” study on more than just the KDR (Kill/Death/Ratio)
https://www.bbc.com/future/article/20200622-the-long-term-effects-of-covid-19-infection
Nick,
You need to base your “Lockdowns are a waste of time” study on more than just the number of deaths
https://www.bbc.com/future/article/20200622-the-long-term-effects-of-covid-19-infection
Before when doctors would see symptoms like that they wouldn’t think covid and would look for the real reason; now all they can think is covid and treat for such, even if it ki!lls patients. Buried in this video is an example of a young person who was acting delirious because his blood sugar was too high, but the doctor ignored that and intubated the patient, which I think ki!lled him.
Nick,
You need to base your “Lockdowns are a waste of time” study on more than just the numbers of deaths
https://www.bbc.com/future/article/20200622-the-long-term-effects-of-covid-19-infection
I fear that the BBC should not be regarded as a reliable source for anything.
Pushing politically correct agit-prop has consequences.
Not just COVID patients, but anyone who goes into ICU and is sedated and intubated and survives will face a long and difficult recovery. Long been recognized by clinicians as a hazard of ICU admission. Sweden opting not to do that to many 80+ patients is probably the correct call. The cure can be worse than the disease frequently in the elderly. Attempting Cancer chemotherapy in the elderly frail tells us this.
Seriously!!!! The article is produced by the BBC therefore all comments by doctors/specialists held within can be ignored?
I am constantly amazed of the power of the mind to shield reality from itself in order to maintain its “i am right” mentality
There are a lot of other viruses that present primarily with one pathology but have many more sequelae in some patients.
Dengue Fever,
Zika,
Yellow Fever,
Measles,
Polio,
Western Equine Encephalitis,
Eastern Equine Encephalitis,
Japanese Encephalitis virus,
That most clinicians in western medicine have never seen these except in medical textbooks, its not surprising they are surprised.
Yes Seriously ! That’s the problem with “Editorial Narratives” – agenda based reporting.
Now crakar ask yourself when last you saw the BBC present two sides to an issue.
And by two sides I don’t mean a debate by two climate alarmists who disagree on how serious the situation is.
The BBC has in recent years become notorious for having a little group of “goto” experts (and “experts”!) mostly with leftist leanings. Any national news organisation that goes to the length of repeatedly lying about its justification only ever to tell one side of a story — as the BBC did and continues to do in the matter of climate change — deserves to be treated with extreme caution over anything it says.
“I am constantly amazed of the power of the mind to shield reality from itself in order to maintain its “i am right” mentality”
That sounds like what you’re doing: avoiding the harsh reality that intubation produces the very symptoms described in the article you linked to. My question is, how can doctors be so clueless to ignore that common knowledge and only think such damage is all caused by a virus?
Icisil, I picked up on that, too. Actually, I read the comment without noticing who wrote it and assumed someone else was making the remark TO crakar24, not the other way around!
The discussion on the “virus” has evolved, in my view, into a few camps who are each looking for confirmation of their bias at the expense of considering any non-confirming information. I think it’s too soon to draw definitive conclusions and it appears many here take the same approach.
Thanks to all for making this a lively forum!
badEnglish
craker24, best to not read ANY proven fake-news source, which is almost all of them. If something is important enough, it will appear in a credible source. What credible source you ask? That question would bolster my suggestion.
Same with Germany. That is likely a reason mortality is lower there. I suspect the pattern will hold across the globe: the more harmful the treatments (particularly intubation), the higher the mortalities.
https://www.translatetheweb.com/?from=de&to=en&dl=en&ref=trb&a=https%3A%2F%2Farchive.is%2FKX5IQ%23selection-4609.23-4621.63
Link doesn’t appear to be working. Here’s original link. Non-German speakers will have to use a translator
https://archive.is/KX5IQ#selection-4609.23-4621.63
People are not intubated until they are physically unable to breathe, mainly because they are exhausted. Not putting the over-80s’ into IC units is mainly because, no matter what treatment, they will die; they are being ‘sacrificed’ to allow others to occupy the beds. ECMO treatment is much better, but the units AND THE TRAINED STAFF are just not available in the numbers required (and many of those trained staff are/have-been themselves ill, or are exhausted by the need to perform hard physical work for long periods while wearing passive respiratory protective equipment. The UK health and safety executive specifies that a person wearing passive RPE and having to perform physically tiring work wearing it, should have a break every hour or so. yet doctors/nurses have to wear it and work for 12/14/16 hours each day.
That’s incorrect. Depending on the country/hospital, people are intubated early as a matter of protocol and policy, which changed during this outbreak due to fear of aerosolization of virus. Many patients have good compliance with no problem breathing, but can’t get enough oxygen, Doctors call it silent or happy hypoxemia. Gattanoni in Italy said about 70% of his patients fell into that category. Only about 20-30% were in respiratory distress with classic ARDS symptoms.
A great example of the BBC’s reliability on anything even remotely to do with science, is their current promotion of the idea that Yemen is a particularly tragic example of the effects of COVID-19.
This narrative avoids pointing out that Yemen has very many problems, not least a civil war that has been rumbling on for at least 50 years, a total lack of effective governance and a war which is now a proxy war between Shia Iran and Sunni Saudi Arabia.
BBC enthusiastically broadcasts heart rending pictures of tiny starving mites, (often in the arms of parents who appear surprisingly well fed) with a narrative of the scourge of Covid.
I wouldn’t want to think I had to rely on health care in Yemen if I had an ingrowing toe nail, although no doubt they have many dedicated and heroic doctors. But Covid? According to the official figures, 5 deaths per million, making Yemen 110th in the World. Tests? 4 per million, so 192nd in the World.
Obviously, I would trust Yemen’s statistics only a tad more than those from China.
But why does the BBC give us this agit-prop about Yemen? They hardly ever mention Belgium, with early and severe Lockdown, whose death per million figures are easily the worst in the world.
Brazil gets plenty of attention (but only ever quoting total deaths rather than deaths per million). But this is just a mechanism for knocking Bolsonaro, who had the cheek to win an election against an incompetent and corrupt Socialist previous government.
Just like BBC’s coverage of the USA, where absolutely everything is Trump’s fault.
You’ d be better quoting Mad Magazine than the BBC.
“incompetent and corrupt Socialist government” is a pleonasm.
oo, thanks for the new word. I will add it to my hoard.
Couldn’t have said that any better
They hardly ever mention Belgium, with early and severe Lockdown, whose death per million figures are easily the worst in the world.
Belgiums story is twofold:
1. They carried the virus very efficiently into their nursing homes.
2. They really did and admitted what other countries, foremost the US, are accused to do on this website: they counted every death that could be COVID-19-related as such without any testing in many cases.
The very different policy of how cases are reported and how much is tested makes it very difficult to compare countries directly. Euromomo excess mortality data suggests Belgium is comparable to France, Italy and the Netherlands and way lower than Spain and the UK.
There seems to be widespread agreement that this coronavirus is mutating. We’re just one mutation away from the virus becoming unrecognizable to our immune systems.
BS.
That statement is a Complete and utter lack of understanding how a healthy immune system functions.
Joel is our collective immune system getting better seeing that more people are testing positive with no symptoms?
No. Other factors are likely at play like Vitamin D levels in the populations of the Nhemisphere as we have gone from winter to spring to now summer. Also infecting doses exposures may be going down as more UV and higher humidity reduces the viability time for aerosolized virus attached to sub-micron particles.
A more likely possibility is that the tests are just crap. Data that don’t mean anything useful
COVID19 PCR Tests are Scientifically Meaningless
https://off-guardian.org/2020/06/27/covid19-pcr-tests-are-scientifically-meaningless/
What a load of crap from non-scientists. They don’t know what a PCR is used for and why. They don’t understand how Ct values can predict viral load, infectiousness and how it was experimentally proven. They don’t understand RNA hybridisation, proteomics and EM microscopy.
They don’t know where the term virus is originating from and how they were discovered.
But they have a strong opinion. Like everybody nowadays. Even if it is completely wrong.
They didn’t even get the very easy definition of sensitivity and specificity right. That is plainly embarrassing.
Oh, and about “hospitals have a financial gain of COVID-19 patients and therefore are misdiagnosing them and writing wrong death certificates”, maybe you believe a clinician first hand who is pro zinc, vitamin D and open to HCQ that the health insurance system does not support this:
https://youtu.be/NkTKA6toUcs?t=1889
Seheult doesn’t cover the increased incentive to diagnose covid in Medicare patients (possibly Medicaid too, don’t know), from the usual $5K per Medicare patient up to $13K if covid, and $39K if covid + intubated. Also, he doesn’t mention “covid rule-outs” who test negative, but are diagnosed covid. See video above.
As far as PCR goes, it sounds like they have a pretty good handle on it. The guy who invented the process disagreed that it could be used for what it’s being used for.
Also, none of the PCR test manufacturers claim that their tests are suitable for diagnostic purposes. Research purposes only.
Also, none of the PCR test manufacturers claim that their tests are suitable for diagnostic purposes. Research purposes only.
That has legal issues. Cause the FDA has to approve a test kit for clinical use. BUT the chemicals used for test kits are the same as in the PCR kits. You can make a relaible test with those. It just isn’t approved so you can’t sue the manufacturer if anything goes wrong.
The many worthless PCR and antibody test kits on the market after the FDA lowered their policy standards cause of COVID-19 tell you exactly why usually the practise is different.
As far as PCR goes, it sounds like they have a pretty good handle on it. The guy who invented the process disagreed that it could be used for what it’s being used for.
Which guy? Drosten? I can assure you the diagnostic at the Charité is using this test. After thousands of tests done and hundreds of virus samples grown in culture they have quite a good understanding which Ct values from nasopharyngeal swaps translate into still infectious virus load. This correlation is backed up from other diagnostic labs in Europe.
As far as PCR goes, it sounds like they have a pretty good handle on it.
No, they don’t. I really don’t know where to start to list all their misconceptions but maybe one of their biggest is a good one:
“all Asian viruses” means all Asian viruses that relate to SARS-subgroup of beta coronaviruses and not freaking all viruses in Asia. That are five, including SARS and SARS-CoV-2. The other three have only been extracted directly from bats and never been found in humans.
So the first test sufficient to give the diagnose “SARS-related virus”. And then you can do more to be more specific but you not necessarily need to bc the chance you have of the other four viruses is very low. Of three of them we don’t even know if they can infect humans at all.
Also, he doesn’t mention “covid rule-outs” who test negative, but are diagnosed covid.
He does address this. Everyone is tested. Without positive test, no COVID-19 diagnose.
Seheult doesn’t cover the increased incentive to diagnose covid in Medicare patients (possibly Medicaid too, don’t know), from the usual $5K per Medicare patient up to $13K if covid, and $39K if covid + intubated.
You know how much one day at the hospital costs? If the patients stay double, triple or even more long than usual that increase just covers the cost. Intubated patients need even more care and stay at least three weeks on average. Do you think $5k would cover this?
“Which guy? ”
Kary Mullis. Whe wn the Nobel prize for inventing PCR. He disapproved of what it is currently being used for.
“He does address this. Everyone is tested. Without positive test, no COVID-19 diagnose.”
You’re living in a fantasy land. That may be the policy in his hospital (which would be exceptional), but the video I posted earlier proves that is not the case everywhere, and doesn’t even touch on presumptive diagnoses.
“Intubated patients need even more care”
No they don’t. When they intubate they basically turn people into vegetables, only requiring ventilator settings to adjusted occasionally. The video I posted earlier mentions that a dentist was monitoring intubated patients. The less harmful oxygenation methods require much more attention and workload. Nasal cannula can fall off, and imagine how many people it takes to prone and readjust obese patients. No comparison.
Kary Mullis. Whe wn the Nobel prize for inventing PCR. He disapproved of what it is currently being used for.
Then maybe he didn’t follow the evolvement of his very own technique. It came a long way from using three different water baths and a timer. ddPCR, taqman-probes etc. The development of polymerases (speed, stability, accuracy) not to mention.
You’re living in a fantasy land. That may be the policy in his hospital (which would be exceptional), but the video I posted earlier proves that is not the case everywhere, and doesn’t even touch on presumptive diagnoses.
Am I? You think the hospitals have not changed anything since March and risk to be sued if any patient contracts the virus in their facility and dies? If you have enough testing capacity you don’t need “presumptive diagnoses”. Did you listen what he was saying? That theoretically there could be patients having the virus and being in the hospital for something else but it is just not what his daily life working with COVID-19 patients shows him.
He works in two hospitals btw.
No they don’t. When they intubate they basically turn people into vegetables, only requiring ventilator settings to adjusted occasionally.
Yes, they do. You have a fundamental misconception about work in an ICU. Patients on ventilators for ARDS are not to be confused with comatose patients with intact lungs. Different story.
Joel,
The virus has already mutated (see D614G) current research suggests those who had the previous version would not have immunity against this newer strain, ergo we are one mutation away from our imune systems not recognising the virus. Best you think before you play the BS card.
You do not know what you are talking about crakar24. Immunity to an acute illness causing virus is far more than a single mutation in an RNA virus. This virus makes that mutation and hundreds of others with every cellular infection cycle in a human host. Our immune system still beats it like a redheaded step child.
Mutations or errors?
As far as I know, this little beast has no error correction code segments.
It looks like a noisy lossy transmission (replication).
Could it be that us eukaryotes evolved something essential?
Joel you seem very keen to denounce every thought offered by other comments, its a shame people like exist because I for one am sick and tired of your self imposed gate keeper approach.
“This virus makes that mutation and hundreds of others with every cellular infection cycle in a human host.”
It doesn’t. No virus does. With a genome of only 20,000 base pairs it would be dead and dysfunctional in an instant if it had hundreds of mutations every replication cycle. In fact, coronaviruses have the most efficient replication enzyme of all viruses cause their genome is the largest.
Or the virus is one mutation away from becoming no more than a minor inconvenience like the other coronaviruses that cause the common cold. And there is at least some anecdotal evidence that some immune systems are recognising it as simply a coronavirus and treating it accordingly.
You’re not related to Dad’s Army’s Private Frazer, are you? You must be great company at parties!
Vis a vis the nature of any mutations, you’ve got to ask yourself one question, “Do I feel lucky?” link
Why don’t we have herd immunity against the common cold and influenza?
The above results further validate what was obvious from the diamond princess experiment.
COVID disproportionately impacts the elderly.
This was obvious 4 months ago.
That the elderly are more susceptible to die from what would be a banal infection to a younger person is not covid specific and was know long before sars-cov-19 was fabricated by irresponsible “gain of function” research and leaked through slack security at WIV.
Oo. No need for conspiracy when stupidity suffices.
You are right on this one. Joel is wrong. Even worse, latest research show individuals with mild to asymptomatic covid-19 will have a short ‘immunity’. For those antibodies start to diminish within three months. That will cause any ‘herd’ immunity dysfunctional. Also questioning vaccines. (This month).
Further, it also seem like a mild or asymptomatic course still may inflict severe harm. (This month).
And it is mutating. So far seem like more contageous. Next we don’t know ! (Published last week).
However there is hope, we have vitamin-D3, NAC and Theanine. (Study released June 26).
T-cell immunity has been largely ignored by the clinical-medical community. Too much stock is placed in simply an antibody titer. Research immunologists who study T cell responses to many different viruses understand the T cell issues and how they are coordinating what B cells do in the big scheme of the immune systems response. T cells are a more important indicator of what is happening. It is just that T cell specificity is much more difficult to measure (and costly) unlike simple antibody tests of serum from a small blood draw. It does not surprise me that we see fewer seroconversions in elderly demographics, as seroconversion requires T cell “licensing” to B cell germinal center reactions in lymph nodes to then generate IgG antibodies.
One huge factor for heterogeneity in Susceptibility is also going to be pre-existing cross-reactive T cell memory for closely related beta-corona viruses. The prevalence of a protective T cell immunity may be as high as 40% of many adults populations in Western countries.
It is from the T cell immunologists that a louder voice of concern should come for two of the vaccine candidates to SARS-CoV-2. The mRNA vaccine and the DNA vaccines that generate mostly antibody responses to this respiratory virus should alarm anyone who understands the details of how the RSV vaccine debacle occurred in the 1960’s. The only vaccine candidate I’ve seen so far that I would put some trust in not killing people is the AstraZeneca vaccine that uses a live, but replication incompetent, adenovirus vector to express the CoV-2 spike protein with a boost regime that appears to generate both antibody and robust T cell responses for host protection.
T cells matter.
I appreciate your comments, as you do know what you are talking about.
Do you think that Asian countries in general are benefiting from T cell memory from other corona viruses? I’ve been to many Asian countries and I find the low fatality rates being observed amazing given their high population densities and general lack of hygiene in normal situations.
Yes, T cells in the end are more important than antibodies to clear the virus. But you are probably wrong about the AstraZeneca vaccine. If their results in apes are predictive than it’s no good at all. In all 6 vaccinated apes that received the virus 4 weeks later, the viral load within the nose was the same as in controls. Even worse, in 3 apes the virus also reached the lungs and caused breathing problems. In addition, immunity induced by the vaccination was marginal at best, with low antibody titers and low numbers of activated T-cells. Briefly: it does not act as a proper vaccin (viral load in the nose), does not induce proper immunity, and does not prevent the virus from damaging the lungs.
In normal times, after such results in a nonhuman primate model, this stuff would have been discarded.
Nick Lewis
Thanks for the excellent work
The level of testing and effectiveness of tracing are also a factor…
S Korea had a high level of effective tracing after a high level of testing: result lower spread of infection.
what are the figures for Sweden? /How was their test/trace/quarantine?
Bear in mind there are social distancing measures in place, a very high level of home working in Stockholm, low population, highest percentage of single households in the EU and 40% of the population lives in sparsely populated rural areas. Sweden also has a population which follows the rules.
I don’t see how Sweden compares at all to the USA.
“what are the figures for Sweden? /How was their test/trace/quarantine?”
Swedish Authorities completely gave up test/trace/quarantine in mid-March (which was illegal by the way). It is only now being re-started in some areas.
Can’t stay away can you? How many times have you said you will leave and never return to WUWT? And yet, here you are.
Showing again that lockdown was unnecessary. In 1968 we didot lockdown in the UK, 80,000 died in total, in three waves. Basic hygiene practises were implemented, hand washing, face masks, that was it.
The Socialists didn’t need a Donald Trump to get thrown out as US president in 1968.
A couple of notes:
– In my copy of this post figures 2 and 3 are missing. Is this intentional, unintentional and applicable to everyone, or am I just unlucky?
– What I would dearly like to see is a figure showing Excess Deaths Week By Week, compared to the average Deaths Per Week for (say) the last five years. That would remove any problems inherent in trying to count the number of deaths of people who died of COVID-19, rather than who just happened to have it when they died. Are such figures available for Sweden ?
Go to https://www.scb.se/om-scb/nyheter-och-pressmeddelanden/scb-publicerar-preliminar-statistik-over-doda-i-sverige/
About halfway down the page is a link, with text “Statistik hämtas som excelfil på scb.se”, to an Excel file that contains the data you seek (and is regularly updated, the last 10 to 14 days worth of data will be too low as it takes time for death certificates to arrive in Stockholm and be officially “registered”).
That Excel spreadsheet is BI-LINGUAL (!) Swedish-English :
– The “Tabell 1” tab gives daily numbers for 2015 to 2020, and even includes a pre-calculated “2015-2019 average” column
– The “Tabell 5” tab does a similar thing with weekly numbers
– The “Tabell 7” tab breaks down the weekly numbers by age group, but only provides “2015-2019 averages” and “2020” numbers
I generated my own “Excess deaths by week” graph from that data easily enough. It peaked in early- / mid-April, and is now almost back down to 0 (even after removing a couple of “preliminary data” lines at the end).
And before march 15 average 2020 was 7.08% below average. So still 7% above ?
Further, there were a lot of dead people at least in the beginning not tested in Sweden.
Limited testing was due to lack of testkits and lack of preparation. (PPE and personal).
And before march 15 average 2020 was 7.08% below average. So still 7% above ?
Further, there were a lot of dead people at least in the beginning not tested in Sweden.
NB : If an “unseen” COVID-19 “death wave” had hit Sweden before March / April wouldn’t the mortality rate have been higher than “normal” ???
The OP only asked for “Excess Deaths Week By Week, compared to the average Deaths Per Week for (say) the last five years”, compensating for “mild flu seasons” versus “bad flu seasons” is both complicated and subjective.
Counting from the crossover point [ Week 11 : “Excess Deaths” = -170 ], the SCB data gives 5220 “Cumulative Excess Deaths” for weeks 12 to 24 (the numbers for weeks 25 and 26 of 2020 are clearly too low / incomplete).
The Worldometers “./country/sweden/” page has 5280 deaths (attributed to COVID-19, up to today, 29/6/2020).
It’s all reasonably coherent (to me, at least).
You must remove the last three weeks. It takes that long before excess deaths is reasonably complete.
Mark – Thank you very much. I’ll go and look at them.
Compare the Covid-19 death rate in Sweden with that in its close neighbour Norway. As well as a >1,000 mile long land border, the two nations share many social and cultural similarities. As of June 29 in deaths per million polulation (Worldometer):
Sweden: 523
Norway: 46
Norway went into national lockdown on March 12.
The virus isn’t finished with Norway by a long ways. Sweden is nearer the end if you didn’t understand what Nic was conveying in his prediction of only about a 1,100 more excess deaths in Sweden.
According to My World Data, daily new confirmed Covid-19 cases in Norway have fallen at a rate of -13 per week since the start of April. In Sweden they have risen by +56 per week over the same period. https://ourworldindata.org/coronavirus-source-data
TheFinalNail got it exactly. Also compare the swedish Covid-19 death rate to its other neighbors Denmark and Finnland. Compared to Germany it would mean about 45thousand dead people instead of 9thousand. Mostly elder people, who built this country, who have a right to be sheltered. A massacre. I am glad, that our politicians listened to the scientists and acted promptly. To be fair, the swedish authorities always said, that they are in a marathon, not in a sprint.
They want to be jugded for their measures after the pandemic. It will however be a very long and hard Marathon for the people of Sweden, when the restrictions of going to other countries will be removed for the residents of the other countries of the EU, but not for them.
To some extent you are just reporting the simple fact that some countries happen to have been hit much less hard by this than others. How about comparing Sweden to the UK, France, Spain, Italy, Belgium, the Netherlands, all those places with comparably high death rates? Actually though, I don’t want to be too blase about any comparisons that might be truly insightful or aimed at analyzing the medical outcomes involved. For instance, I understand that Denmark in particular, besides being close neighbors to Sweden, was for a while quite similar in the new cases per tests aspect of things. Despite this, Sweden has been persistently higher in the death rate. Is hospital care better in Denmark, so fewer deaths there, relative to the incidence overall?
What mustn’t be missed here is that, given the ‘hard to explain’ differences between countries and regions, there is every indication that Sweden is following the same *pattern* over time as most Western countries, with deaths peaking sometime in April and declining steadily ever since. This in direct contradiction to the alarm narrative that says both the incidence rate and deaths ought to be *exploding* in Sweden (as the only country to avoid draconian business shutdowns or related lock down measures). If it’s not actually climbing in Sweden, that’s a sure indication that other countries could have used more moderate distancing measures too — they would still have followed the same ‘topping out’ pattern, with quite likely better health results from a better economy in the long run.
Sweden is overtaking those countries one by one.
The reason death rates are so high in Sweden is that the quality of care for old people is low, and that the medical system was severely overstrained due to uncontrolled immigration even before the panemic. Essentially we have hospitals for 8 million people trying to handle 10+ million.
In many cases old people infected by COVID-19 were simply given massive doses of morphia and left to die, often without even being examined by a MD. The doctors prescribed “palliative care” by telephone.
Not necessarily true. With measures like face masks, distancing you are also lowering average viral load. And it is obvious with this disease that its severity depends on viral loads. Just check Italian doctors…
So it is really possible that Norway will get through epidemic with less pain, because most of people got into contact with virus by smaller loads. So they will have more asymptomatic and more lighter cases. And they will still build herd immunity.
The major control measure found to work is religious devotion to hand washing.
Face masks are a distraction with no evidence of usefulness in preventing viral transmission.
https://www.sott.net/article/434796-The-Science-is-Conclusive-Masks-and-Respirators-do-NOT-Prevent-Transmission-of-Viruses
Only because of early adoption of face masks, one week after first case, Slovakia became one of best Covid-19 handling countries in the world. With 5 deaths per million and 305
cases per million. Masks are decreasing spread of virus around 4 times, from R0 at 3 to R0 at around 0.8.
I was observing this from first row and saw countries around me, like Czech Republic, Austria, Poland, France etc. adopting face masks and two weeks later see drastic drop in new cases. Every country which stubbornly refused face masks learned hard way. And finally accepted.
As last week ago California mandated usage of face masks. So just keep watching in one week how number will slow down.
Thanks for that link, Nessimmersion . Here is one quotation from that article:
” if there were any benefit to wearing a mask, because of the blocking power against droplets and aerosol particles, then there should be more benefit from wearing a respirator (N95) compared to a surgical mask, yet several large meta-analyses, and all the RCT, prove that there is no such relative benefit. Masks and respirators do not work. ”
Now this article certainly *would* seem to confirm my own ideas as to what is ‘common sense’ on this matter, based on things I’ve read before, that regular surgical masks, especially (and/or homemade masks as well), are certainly *not* effective in stopping or controlling viruses.
So why do we get all the current stories as how various places have been helped by adopting masks? The infection rates fluctuate up and down, right, so do we have misattributed cause and effect, again, with ‘correlation mistaken for causation’, same mistake as ever, for ever and ever?
One question that I’ve not seen answered yet, and is key to the long term planning is : was this a natural transmission from animal to human or was it accidentally released from a lab (possibly having been modified).
If the former then we will have future events, if the latter then it can die out, okay it may take a few years, but that should be it.
The answer to your questions is probably a single “yes.” Animal to human via accidental (lax controls) release by allowing an infected lab worker to then go home. The Chinese were playing with fire and got burned. And then the govt tried to cover it up until they no longer could.
Increasingly there seems to be evidence that this thing has been out “in the wild” for the best part of a year. Which probably lets the Wuhan lab off the hook.
On the other hand the “sigh of relief” from one of that lab’s senior staff when she found it “wasn’t one of mine” is quite. It more than suggests that it could well have been “one of mine” or why the sigh of relief? And of course it could in any case be a mutation of one of hers that only reached its murderous level around Christmas time.
Epidemiologists might like to tell us whether that suggests its next “incarnation” will be wimpish or even more deadly!
We swedes are a strange people.
First we don’t have lockdown in sweden of that simple reason that the swedish government don’t have any legal autority to impose any. I’m horrified when I read what other governements around the world does.
We do have “special” laws but the governement can only use them if we are at war and no, this is not a war.
Second, it dies around 250 persons in sweden every day, it’s the “normal”. In april and may, we did have a peak of around 300, but now it’s back to normal around 250/day.
I don’t think you can protect a population from covid 19, you can only delay it but as soon as you open up the cases will rise. We will never get rid of it.
Covid 19 will be with us forever.
Quarantaine for anyone passing our border in late January had done the trick !
Lars, we in Slovakia still prefer to have close to zero cases, go shopping or in bar without fear to contract Covid-19.
And really I’m sleeping better when I know that my parents closing to their 70 are safe from virus.
If there is storm on the sea, it is never wise to steer boat directly to it. It is always best option avoid it.
Thank you Lars for adding your comment about the daily number of people dying in Sweden that has decreased to the normal number. Many people are unaware of this, or prefer to ignore it because they are prejudiced that the Swedisch approch will not work. The world may never get rid of this virus, but Sweden will be one of the first countries that achieves herd immunity (maybe they already have). It will be much easier then to control an occasional outbreak (for instance from people that enter the country from abroad.
Here in New Zealand we have achieved that situation.
Unfortunately, we now cower behind our borders, afraid to go anywhere. There are serious discussions as to if we should stop our own citizens from returning home.
The situation is not sustainable, and when we reopen borders, as inevitably we must, will it have all have been in vain?
We in Slovakia are already past that. Few weeks of zero cases, then opened borders. But it is working somehow. Pressure is here, import is coming, but testing and searching contacts of sick helps.
Normal this time of year is about 225. There is still excess mortality, but statistics for the most recent three weeks is essentially meaningless due to lag in reporting.
And the peak was actually over 350.
“First we don’t have lockdown in sweden of that simple reason that the swedish government don’t have any legal autority to impose any.”
That is a myth. Read “Smittskyddslagen”. The government can do anything they want to stop contagion. After enumerating what the government can do, it adds that it can also impose whatever other measures are needed.
So much focus on numbers, although illuminating at times, might still miss the larger points:
– Swedish policies might have not worked in most countries since people do not behave exactly the same, in statistical, relevant sense, all our Europe. This is a sociological fact completely discarded by number junkies.
– Swedish policies took into account the knowledge at that moment in time and a projection into the future of most likely outcome. Part of this was the estimation that finding a vaccine will take multiple years.
– Swedish authorities already indicated they would have done things somewhat differently in hindsight. This in itself would tell you they are not in need of defense.
– Latest news from Sweden will tell you the death count will be re-calibrated soon and will show quite a new picture. In general, no country counts the dead in the same way. This can lead to major differences when comparing numbers.
There are no plans to “re-calibrate”, because it could only be re-calibated upwards.
Excess mortality has been significantly higher than recorded COVID-19 deaths. And it is well known that local authorities have covered up deaths in nursing homes by deliberately not testing patients.
In other words, the difference between lockdown and sensible behaviour of an informed population is not significant. Hence, at the face of it, the UK lockdown was a futile exercise.
Thanks to the ‘best scientific advice’ the economy was run into the ground for no good reason.
Who will hold the ‘experts’ to account?
No it doesn’t. The people pushing Lockdown doesn’t work never compare them to those countries that did a proper hard & fast lockdown who have very low or zero new cases and very low or zero deaths.
Even in the UK with a very poor lockdown our current 7 day New Cases/Million rate and our current 7 day Deaths/million are below Swedens.
114 cases/million v 634 case/million and 14 Deaths/million v 23 Deaths/million.
Countries like South Korea, Taiwan and closer to home Slovakia or Greece went into lockdown hard the moment the first fatalities happened. That was long before the peak of the first wave would have been reached. Therefore it was successful and they could more or less come out of it relatively quick. The UK went into lockdown after or at the peak at which time it clearly had no useful effect anymore. The Sweden data you give are affected by more testing recently and also because of a time delay compared to the UK. The total death toll since the start of the outbreak is 641/million UK and 523/million Sweden according to the WHO.
Yes but the overall doesn’t show the changes in the last month. The UK has also increased it’s testing as well.
UK – 136,854 Tests/Million Sweden – 444,607 Tests/Million.
It should be strikingly obvious that:
1. All the lock downs, masking dictates, social distancing, etc., has had no effect on people contracting the virus.
2. The “flattening” will not reduce the number of total cases – at best, just the distribution – this is exactly what the experts told us in the beginning. This is what all the “spikes” show with “re-opening” confirming their efforts to avoid overwhelming medical resources.
What should the Trump admin do based on all this data and experience gained? It’s really extremely simple:
A. Create a Daily Coronavirus Treatment Task Force (DCTTF) composed to leading medical clinicians and treatment specialists. There is no need to even have the Pence Coronavirus Task Force since all they can do is perform a bean counting exercise and are useless as to clinical treatment.
B. Have the DCTTF present facts like those presented here. I.E., if you’re under 60, you chance of going to hospital is pretty much zero.
C. DCTTF presents their “best treatment” protocols which they submit to governing medical bodies to study – however, the DCTTF protocols will be used for the remainder of the crisis. Treatment todsy — NOT awaiting some jury of experts — using most current clinical outcomes.
D. DCTTF directs resources for directing rapid-response treatment resources to any and all hot spots.
E. Promote the fact that the original crisis of being overwhelmed, regardless of final analysis, is over and will never occur.
F. Rinse, repeat.
It would be truly great if they also stated that all the masking and distancing and the rest is useless. Life must return to normal in that you contract some disease, you go to your medical professional who treats you and you recover if you don’t already have cancers, metabolic illness, or at the end of life in a nursing home. Even for the severe cases, use the best clinical treatment proven in clinical practice, for even the end of life patients.
Tell that to South Korea, Taiwan, Czechia, Malaysia, Thailand, Hong Kong, Vietnam, New Zealand, Australia, Israel, Norway, Finland etc.
Have you tried ordering the Countries by Cases/Million population or Deaths/Million population?
Go watch Ivor Cummings videos on Youtube. He’s a bio-engineer and has all the charts and comparisons. His conclusions include nothing actually “stopped” or effected the typical viral response curves. The short version:
Thanks to Nic Lewis.
Here is a small graph of the deaths in Sweden on a weekly bases for first 26 weeks of 2020 and the average for 2015 to 2019:
http://carl-fh.com/images/offsite/sweden-death-week-20200629.pdf
The data after w. 22 are unreliable because of lags in reporting deaths. Excess mortality is actually higher.
@tty and whom may be in doubt.
I had already discarded the last two weeks 26 and 27, so what you see on the graph is correct.
No, it is not.
w. 23, 24 and 25 are also shonky. Here is how much mortality changed for w. 22-25 between the latest two editions of the SCB statistics:
w. 22 +8
w. 23 +22
w. 24 +134
w. 25 +1166
No data for excess mortality after w. 22 can be considered reliable at this time.
What do Sweden, Norway, and Finland have in common? These nations have the highest vitamin D levels in Europe, whether by diet or genetics. The nations with the highest COVID-19 deaths, Spain and Italy, have the lowest D levels. In the United States, the worst hit demographics are the elderly and African Americans, both cohorts having low levels of vitamin D. One study found 93% of African Americans are deficient in vitamin D. There is a strong correlation between vitamin D deficiency and COVID-19. The data is out there, but medical researchers are ignoring it. I’ve urged my online friends to take vitamin D and spread the word.
The data is out there, but medical researchers are ignoring it.
There are a couple of trials on COVID-19 and vitamin D3. I would hardly call that “ignoring”.
Great analysis. Though I question how much of the difference in death rates in different countries can be put down to lockdowns when some countries that had early and strict lockdowns had such high death rates while others with light or no lockdowns had low death rates. Some countries saw infections begin to slow before lockdown while others saw them climb fast after lockdown.
why the obsession with Sweden?
whatever, Sweden shows no exponential curve which should have their death toll up by multiples of where they are.
much more interesting is Japan which belatedly had a very soft lockdown:
Statista: Coronavirus (COVID-19) deaths worldwide per one million population as of June 29, 2020, by country
#90 Japan 7.68 deaths per million
https://www.statista.com/statistics/1104709/coronavirus-deaths-worldwide-per-million-inhabitants/
3 Apr: Nikkei Asian Review: Tokyo governor says lockdown in Japan is ‘impossible’
Japanese law makes it “impossible” to impose a forced shutdown in Tokyo as seen in other global cities such as New York or Paris, Tokyo Gov. Yuriko Koike told the Nikkei Asian Review.
“Because Japan’s law puts emphasis on protecting personal rights, a lockdown is impossible,” Koike said in an interview on Friday, adding that she can ask for “no more than voluntary restraint.”…
An official of Japan’s ruling Liberal Democratic Party said Friday that he expects Japan to declare a state of emergency soon, but that the country’s constitution does not permit the government to demand individuals to stay home due to civil liberty concerns. “It will not be compulsory or mandatory,” he said. “It would be a request.”…
https://asia.nikkei.com/Editor-s-Picks/Interview/Tokyo-governor-says-lockdown-in-Japan-is-impossible
Interestingly, what Japan & S Korea have and the rest of the world does not is bidet toilets.
Bidet toilets have around 70 % of installations in Japan & 60 % in S Korea.
We already know the social distancing on Japanese trains can be down to 0.5 mm, similar on Korean buses.However both countries have very high standards of public hygeine, handwashing, not shaking hands at introductions etc.
As there appears to be strong evidence of fecal transmission (like Polio) the control measures put in place are a red herring.
We know old folks homes struggle with contamination issues, very hard to maintain hygeine with so many being either demented, incontinent or liable to have toilet accidents.
We also know that despite everyone & their dog wearing dustmasks in Wuhan it didn’t do any good.
However some S Korean hospitals have reported no transmission between rooms by enforcing religious handwashing between rooms / beds in hospitals.
No messing about with gels, just traditional soap & water.
So it appears that fecal transmission is much more common than we like to admit and the 2 countries with the best control of Covid have the best general public hygeine, I.e. bidet toilets in more general usage.
Nils Tegnell, physician specializing in infectious disease and current state epidemiologist of Sweden spoke clearly months ago that we will only be able to properly assess the statistics when we can look back over a year since the start of the virus spreading. I believe this will vindicated him but in all likelihood the media will not correct all their virus falsehoods. When looking at the stats of many countries, most do not allow for an apples with apples comparison.
We can add the following about the real costs to the above:
The Doctor Is In: Scott Atlas and the Efficacy of Lockdowns, Social Distancing, and Closings
https://www.youtube.com/watch?v=kZqGSnVt8c8
For every life year lost to COVID-19 two life years have already been lost due to lockdowns.
YES – all this blathering about lockdowns ignores the effects of the lockdowns. Everyone should watch this video. I can see the effects in my own family. My grandfather committed suicide 2 years after the 1929 crash. Now one son in law who was laid off is being treated for major depressive disorder (despite Trudeau’s 2k/month). Vallient’s analysis of the 1923 Harvard class shows 10-15 QUALY years lost from men who have MDD prior to the age of 50 – look it up. My other son in law is working reduced hours from home. His blood sugar and gout are completely out of control, and it looks as if he will be insulin dependent in the near future.
The supporters of the lockdown are largely people whose income is not affected by the lockdown. It is the young and middle aged who are bearing the costs. This is immoral.
The only number that matters about COVID-19 is the Case Fatality Rate. If COVID-19 has a low CFR, it simply doesn’t matter how many people get it. Everything that has been done is predicated on the notion of a high CFR. If the CFR turns out to be low, absolutely none of the lockdowns were justified. At first, I thought the CFR might be as high as 30%. Since I’ve been tracking the numbers the CFR (in the US, at least) has dropped to about 5%, and is steadily declining in spite of an increasing number of cases. In fact, the more non-fatal cases they find, the lower the CFR becomes, and the justification for the lockdowns disappears.
Subtract mortality caused by policy decisions of politicians/bureaucrats/administrators, like seeding nursing homes with infected patients and unwarranted early intubation of patients to avoid potential aerolsolization of virus, and that CFR goes down quite a bit.
I am taking Vitamin D3 x 6 tablets & 1x K2 tablet plus 4x Vitamin C tablets daily. Haven`t had a cold or cough for a very long time. I am glad as you folk have written here, that it is a solid defense against COVID -19.
This data and Nick’s analysis is interesting. I would be careful about making any conclusions at this time, but I would say that the trends are encouraging. I believe that we can also say with high confidence that mere exposure to this virus is not a death sentence for most of the population and that long, severe lock-downs were not necessary. All of the long term economic and social harm that the lock-downs have caused will be blamed on the virus by many, but in actuality it is all due to the overreaction to the virus by our leaders.
the Swedish statistics authority cannot be trusted.
Statistics that are unpalatable in that country do not exist any more.
It’s the China of Europe, where censorship is so bad that it needs not be enforced. Researchers who do honest research on topics like immigration, get attacked by the media and politicians.
When journalists get attacked by migrant mobs, everyone comes out of the woodwork to attach and mock the victim of the assault.
What we are seeing with the pandering to BLM< well, take that and put it on steroids, that's Sweden
OK, for the sake of the argument let’s assume that’s true.
1) Which “authorities” can be “trusted” to supply “honest” mortality data for Sweden (or anywhere else) ?
NB : Please provide links to regularly updated data sources.
2) If the answer to question 1 is “Nobody”, how can you (second-person singular) possibly know how “bad” (/ “good”) the situation “really is” in Sweden (or anywhere else) ?
If you are an authoritarian dictatorship you just use your soldiers as guinea pigs:
https://www.reuters.com/article/us-health-coronavirus-china-vaccine-idUSKBN2400DZ?fbclid=IwAR3fDgDLWuApjIHvloKyFRhN9jPJiuo4qeTjusARfzggWw5_iIkxnOK1KFs
Thank you for an informative article. Some comments to date have been quite insightful. Not to lose sight of the principle point as to whether lockdowns imposed in countries, other than Sweden, have been more effective at containing the contagion I pass on this sad news from here in Ontario courtesy of the Toronto Star:
The National Institute on Aging says that as of May 6, 3,436 residents and six staff members of long term care settings had died of COVID-19, representing 82 per cent of the 4,167 deaths reported as of Wednesday.
Dr. Samir Sinha, research director at the institute, says it is a staggering figure, given the roughly 400,000 residents living in care homes represent just one per cent of Canada’s population.
And it is a much higher figure than was indicated in a study released days ago by the International Long-Term Care Policy Network.
It said people in long-term care accounted for 62 per cent of Canada’s COVID-19 deaths. It also found Canada has the highest proportion of deaths from COVID-19 in long term care settings among 14 countries.
Sinha’s team compiled data from long-term care residences, nursing and retirement homes, public health units and the provinces.
Ottawa has not released national data on the exact number of deaths in the long term care sector.
However, chief public health officer Dr. Theresa Tam confirmed Thursday that about 81 per cent of deaths are “linked to long term care facilities.”
Clearly the stable doors were locked down after all the horses had bolted so far as aged long term residents were concerned. I wonder if this is reflective of government actions in other jurisdictions and what it says about current government lockdown effectiveness.
This article is very misleading. The ONLY way to see if Sweden is doing well with no lockdown is to look at the other Scandinavian countries. Deaths per million for Sweden so far is 525, where as is Denmark 104, Finland 59, and Norway is 45. By this measure alone Sweden had killed 10 times more people than Norway who had strict lockdowns early.
Cases per million shows Sweden is the WORSE of all EU countries. Current as of today 6,700 per million. The next country down from them is Spain and Belgium at 5,300. Looking at a graph of cases per million over time, every EU country has leveled off, while Sweden continues to rise exponentially.
Looking at the rate of tests finding cases is very high for Sweden at 8.3%. Out of 100 tests they are finding 8 who test positive. Compare that to Finland, Norway and Denmark (0,5%, 0.4% and 0.2%). This means those latter countries succeeded, because of lockdown, in slowing the spread to a trickle.
One also has to be careful when using Swedish data. They have not been reporting on the weekends, catching up on Tuesday. Friday is the best day to see what the over all trend is.
As for herd immunity? Dont count on it.
https://hub.jhu.edu/2020/04/30/herd-immunity-covid-19-coronavirus/
Were COVID-19 Lockdowns Worth the Cost?
The evidence suggests Americans are right to wonder.
Jacob Sullum6.29.2020 4:40 PM
https://reason.com/2020/06/29/were-covid-19-lockdowns-worth-the-cost/?utm_medium=email
What would the cost have been for not locking down? Far far worse.
https://foreignpolicy.com/2020/04/01/coronavirus-pandemic-war-games-simulation-dark-winter/
Brazil is going to experience worse case.
Plus:
Lockdown and school closures in Europe may have prevented 3.1m deaths
https://www.imperial.ac.uk/news/198074/lockdown-school-closures-europe-have-prevented/
It shows that the professionals running Sweden are just that bit smarter than the fruit loops running the rest of the world. For people waiting to die in nursing homes dying from natural causes a bit earlier than they might otherwise have done is no crime – destroying the global economy to prevent that is, and amounts to anarchy.
How many years of early loss of one’s life does it take to be a “crime”? 2 years, 5 years, 10 years? By your logic we should just end elderly people’s lives at 80. What’s the point in keeping them alive consuming resources? #BoomerRemover right?
Isnt the role of medicine to preserve life as long as the patient wants? You think not one of these patients wanted to live longer?
Rather callous of you to not care what the patient wants.
This was supposed to be “spreading the curve” with the intention that when you reach the end of the curve you have “herd immunity” with a 60-70% recovery rate.
Instead, what we have is a curve that was starved to look like “spreading the curve” but we were left well short of “herd immunity”, so the curve continues.